Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
15 Cards in this Set
- Front
- Back
|
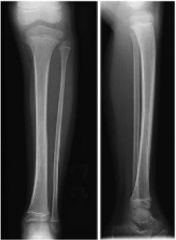
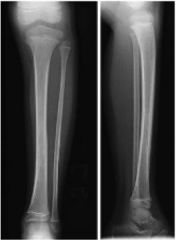
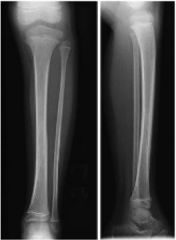
A 3-year and 6-month old child fell while playing with friends 2 hours ago and has avoiding bearing weight on the right leg since that time. The child is afebrile and exam reveals tenderness along the distal tibial shaft with no significant swelling. Radiographs are shown in Figure A and B. What is the most appropriate treatment?
|

Long leg cast application
The clinical presentation and radiographs are consistent with a toddlers fracture of the tibia and the next step in management includes long leg cast application. |
|
|
A 23-month-old girl refuses to bear weight since falling on the playground yesterday. The child is afebrile and her WBC and erythrocyte sedimentation rate (ESR) are within normal limits. On physical exam the leg has no erythema, but does have mild tenderness along the distal tibial shaft. Plain radiographs are negative. What is the most appropriate management?
|
long leg cast
The clinical presentation is consistent with a toddler's fracture, which is treated with a long leg cast. Initial radiographs are often negative but follow-up radiographs may demonstrate a healing periosteal reaction. According to Mashru et al in a review of tibia fractures, toddler's fractures are one of the most common injuries in the child younger than 2 years. They are non-displaced spiral fractures of the tibia caused by low-energy twists and falls. The treatment is application of a long leg cast for 3-4 weeks. |
|
Toddler's fracture
characteristics? also known as ? -age group, children< ? -unlike child abuse injury, which occurs ? -mechanism, low energy trauma with ? -unlike non-accidental injury, which typically involves ? |
Toddler's fracture
characteristics- nondisplaced spiral or oblique fracture of tibial shaft only fibula remains intact -also known as childhood accidental spiral tibial (CAST) fractures -age group-children< 3 years (walking toddlers) -unlike child abuse injury, which occurs in children not yet walking -mechanism low energy trauma with rotational component involves distal half of tibia shaft only fibula remains intact -unlike non-accidental injury, which typically involves proximal half of tibia |
|

Toddler's fracture, Symptoms? (horse)
Physical exam (horse)? (I/P, Prvc, Assoc) |

-Symptoms - pain; bruising; limping or ; refusal to bear weight
-Physical exam- I/P: warmth; swelling over fracture site; tender over fracture site prvc- pain on ankle dorsiflexion Assoc- always have high suspicion for comparment syndrome |
|
Toddler's fracture
Radiographs views? ipsilateral ? findings? |

Toddler's fracture
Radiographs; views; AP and lateral views tibia and fibula are required -ipsilateral knee and ankle must be evaluated to rule out concomitant injury -findings- Toddler's fracture are nondisplaced spiral tibial shaft fracture |
|
Toddler's fracture
acceptable reduction? (traffic light) followup frequency? serial radiographs are performed ? |
Toddler's fracture
-acceptable reduction displaced with 50% apposition;- < 1 cm of shortening; -< 5-10 degrees of angulation in the sagittal and coronal planes -follow up xrays - 2 weeks to evaluate for callus in order to confirm diagnosis in equivocal cases -serial radiographs are performed to monitor for developing deformity |
|

Toddler's fracture- surgical indications ? (pins)
techniques ? (horse) Complications? (beer) |
Surgical Indications-1 (< 5% of tibia shaft fractures); 2 unacceptable reduction (50% app/<1 cm s/<10 A-S/C) 3 marked soft tissue injury; 4 open fractures; 5 unstable fractures; 6 compartment syndrome; 7 neurovascular injury; 8 multiple long bone fractures; 9 >1cm shortening; 10 unacceptable alignment following closed reduction (>10deg anguation)
techniques - external fixation; plate fixation; percutaneous pinning; flexible IM nails -Complications- 1 Compartment syndrome 2 Leg-length discrepancy 3 Angular deformity- varus for tibia only fractures 4 valgus for tibia-fibula fractures; 5 Associated physeal injury; 6 Delayed union and nonunion usually only after external fixation |
|

Supracondylar Fracture - Pediatric
Which of the following elbow apophyses is the last to fuse during growth? mnemonic of the order of APPEARANCE of the individual ossification centers of the elbow is ? & AGE |
Supracondylar Fracture - Pediatric
Internal (medial) epicondyle internal (medial) epicondyle, is the last to FUSE at around 16 to 19 years. While the external (lateral) epicondyle is the last apophyses to APPEAR on radiographs; mnemonic ossification centers of the elbow is C-R-I-T-O-L: C-Capitellum-1yo, R-Radial head-5yo, I-Internal/medial epicondyle-5yo, T-Trochlea-9yo, O-Olecranon-9yo, L-Lateral epicondyle-10yo |
|
What is the advantage of medial and lateral crossed pins compared to two lateral pins in the treatment of supracondylar humerus fractures?
|
Greater experimental biomechanical stability
maximum stability for supracondylar humerus fractures was provided by two crossed pins placed from the medial and lateral condyles in a cadaveric laboratory study. Lee et al also found crossed pins were more stable. |
|

A 7-year-old boy falls off the playground and sustains the injury shown in figure A. What motor deficit is associated with the neurologic injury most common to this fracture pattern?
MC with which extension SC fx MC AIN injury? |
Hand intrinsic weakness
flexion type supracondylar humerus (SCH) fracture, in which the distal fragment is displaced anteriorly. In these fracture patterns, the ulnar nerve is the most likely to be injured, specifically by the sharp spike of the proximal fragment. MC-AIN posterolateral displacement=median |
|

What is the cause of cubitus varus after a supracondylar humerus fracture in a child?
|

Malunion of the fracture
Cubitus varus is typically caused by malreduction of the fracture at the time of fixation resulting in malunion; not usually by growth arrest. |
|
|
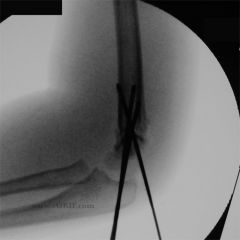
A 10-year-old boy jumped from the playground and sustained the injury shown in figure A. His hand is pulseless and cold. What is the next step in management?
mnemonic of the order of APPEARANCE of the individual ossification centers of the elbow is ? & AGE |
Closed reduction
"Vascular insufficiency at presentation (prevalence, 5%-17%) should be managed initially by rapid reduction and pinning without arteriography." mnemonic ossification centers of the elbow is C-R-I-T-O-L: C-Capitellum-1yo, R-Radial head-5yo, I-Internal/medial epicondyle-5yo, T-Trochlea-9yo, O-Olecranon-9yo, L-Lateral epicondyle-10yo |
|
A 5-year-old boy sustains a type II (Gartland classification) supracondylar fracture which is treated with cast immobilization. Healing results in a mild gunstock deformity. Surgical treatment of this will most likely result in:
type 4 is? |
improved cosmesis
A gunstock deformity, also known as cubitus varus, is the most common complication following a pediatric supracondylar humerus fracture. Cubitus varus typically does not affect range of motion, pain, function or growth. However, cosmetic concerns or recurrent elbow fractures may result. Tardy ulnar nerve palsy may also result, but is not common. Type IV Complete periosteal disruption with instability in flexion and extension |
|

The most common nerve injured in the fracture shown in Figure A innervates all of the following muscles EXCEPT?
(horse) |
The anterior interosseus nerve (AIN) is MC nerve injured with extension type pediatric supracondylar fractures .The AIN, a branch of the median nerve, is principally a motor nerve and innervates:
1 Flexor Digitorum Profundus Index; 2 Flexor Digitorum Profundus Middle; 3 Flexor Pollicis Longus 4 Pronator Quadratus. It DOES NOT innervate Extensor Pollicis Longus, which is innervated by the PIN, branch of the radial nerve. |
|

8-year-old boy has a cubitus varus deformity of his left elbow after a supracondylar humerus fracture was treated in a splint. What is the most common cause of this deformity?
|
Malreduction causing malunion
Supracondylar humerus fractures are the most common elbow fractures in children, accounting for 60-80% of pediatric elbow fractures. This usually is the result of malunion caused by failure to reduce a collapsed medial column or failure to correct rotation at the fracture site. |