![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
104 Cards in this Set
- Front
- Back
|
According to the 'Deviation from social norms theory', what is the definition of abnormality? |
abnormality is a violation of acceptable patterns of behaviour (social norms). For example, it is not a social norm to say that you hear voices in your head (Schizophrenia) |
|
|
Explain the ideas behind 'deviation from social norms' theory |
allows for desirability of a behaviour, both for the individual and for society as a whole. Many people labelled as clinically abnormal behave in a socially deviant way. |
|
|
What are the cultural issues associated with the deviation from social norms theory? |
social norms are not the same in all cultures therefore it may not be possible to decide if someone is breaking social norms by just using one culture's set of social norms. For example it is common in North American cultures to hear voices however in Western society that is seen as abnormal. Therefore we can conclude that the social norms definition is not universal. |
|
|
What are the historical factors associated with deviation from social norms theory? |
cultures can change over time and the ideas about what is normal according to the definition might not be able to keep up with such change so people will be seen as abnormal when society does not. For example, homosexuality was a criminal offence up to 1967 however it is now socially acceptable. |
|
|
Does the deviation from social norms theory distinguish between wether a person is eccentric or abnormal? |
the definition is not reliable because it cannot distinguish between eccentric behaviour and pathologically abnormal behaviour. Eccentric people may break social norms but these people would not be classed as mentally ill. For example, a person streaking at a football game would be displaying eccentric behaviour but according to this definition they would be mentally unwell. |
|
|
Does the deviation from social norms theory evaluate if social deviancy is a bad thing? |
social deviancy is not necessarily a bad thing. Some people are socially deviant because they have chosen a non conformist lifestyle and others because their behaviour is motivated by high principles |
|
|
Does the deviation from social norms theory evaluate if deviancy is abnormal or criminal? |
the definition is unreliable because it cannot distinguish between criminal behaviour and pathologically abnormal behaviour. Criminals break explicit social norms but are not pathologically abnormal but would be abnormal according to this definition |
|
|
What is the failure to function adequately theory's definition of abnormality? |
abnormality is when a person is unable to live a normal life such as going to work, forming close relationships or going outdoors. For example a person with severe depression may not go out of the house therefore they may not be able to maintain or form close relationships with others |
|
|
Explain the ideas behind failure to function adequately theory |
in society we have expectations of how people live their lives however when an individual cannot meet these obligations then we feel like they are not functioning properly. |
|
|
What did Rosenhan and Seligman suggest about the failure to function adequately theory? |
the concept of distress and failure to function adequately can be extended to include a number of behaviours |
|
|
What were Rosenhan and Seligman's seven features of failing to function? |
- Suffering (the person shows a sign of suffering) - Observer discomfort (a person watching the behaviour would feel uncomfortable) - Maladaptiveness (behaviour preventing an individual from achieving major life goals such as enjoying good relationships) - Vividness and unconventionality of behaviour (behaviour differs substantially from how most people behave) - Unpredictability (behaviour is variable and uncontrolled) - Irrationality (a common feature of abnormality) - Violation of moral or social standards (deviating from established standards) |
|
|
What are problems associated with awareness according to the failure to function adequately theory? |
the main problem with defining abnormality is that not all people who experience mental disorders are aware of their failure to function. For example, people suffering from Schizophrenia often deny they have a problem. |
|
|
What are the cultural issues associated with failure to function adequately? |
what is defined as functioning adequately may vary from one culture to another so one cultures ideas about what is normal functioning may be abnormal in another cultures. For example travellers do not have jobs and they live in caravans. For our society this would be abnormal however for their society it is a social norm. |
|
|
Is the failure to function adequately theory objective? |
this definition doesn't recognise the individuals subjective experience. Inevitably, however, such judgements are made by others, and those judgements are influenced by social and cultural beliefs and biases. |
|
|
Are there any exceptions to the rule with failure to function adequately theory? |
there are behaviours that do not fit with this definition. An anxious student before an exam might behave inadequately but such behaviour would not be labelled as abnormal. However, sociopaths might show aggressive behaviour without personal suffering or dysfunction because of their amoral attitudes. |
|
|
Is there a direction of causality associated with failure to function theory? |
inability to cope with the demands of daily living may be a cause rather than an effect of a mental disorder. This might explain why there is a higher incidence of mental disorders among ethnic minorities, owing to prejudice and discrimination, which have been found to impact on psychological well being. |
|
|
What is the definition of abnormality according to deviation from ideal mental health theory? |
instead of defining abnormality, deviation from ideal mental health theory its out to define normality. Abnormality is therefore an absence of normality. Humanist argue that normal people strive to achieve certain goals and abnormality results from a failure to achieve. |
|
|
What are Jahoda's 6 factors which were necessary for living a normal life in deviation from ideal mental health theory? |
- A Positive view of self - Accurate View of Reality - Personal Autonomy - Environmental Mastery - Resistance to stress - Self-Actualisation PAPERS |
|
|
Explain positive view of self? |
a person who is depressed might have a very negative view of themselves and so would not meet this criteria and would therefore be abnormal |
|
|
Explain accurate view of reality |
seeing the world in a true way. A person with schizophrenia might believe that they are emus as part of their delusions. This inaccurate belief will mean they would not meet this criteria and would so be classed as abnormal. |
|
|
Explain personal autonomy |
independence. A person with agoraphobia may not be able to go out or buy food or clothes would be dependent on others to do that. They would not meet this criteria and would so be classed as abnormal. |
|
|
Explain environmental mastery |
being in control of your surroundings. A person with agoraphobia will not be able to go out of the house so they will not be able to master their environment so not meeting this criteria and therefore being classed as abnormal. |
|
|
Explain resistance to stress |
being able to find coping strategies and tolerate stress. A person with anxiety will not be able to cope with additional stress such as A levels so they will not meet this criteria and therefore being classed as abnormal. |
|
|
Explain self actualisation |
reaching your potential. A person with a substance use disorder may be unable to study and work effectively so they can't reach their true potential in that important part of their life. So they would not meet this criteria and so be classed as abnormal. |
|
|
What cultural issues involved in deviation from ideal mental health theory? |
this definition is based on Western ideas of self actualisation and autonomy. In collectivists cultures, it may be abnormal to pursue your own individual ideals and goals and would not be regarded as nor tam to put your own wishes before those of others. Therefore this definition may not be valid for all cultures. |
|
|
Is the deviation from ideal mental health theory difficult to measure? |
the vague criteria for ideal mental health are hard to measure. How can we rate positive interpersonal relations or self acceptance? |
|
|
Is the deviation from ideal mental health theory too difficult? |
very few of us can really say we are self actualised so would be classed as abnormal. This criteria is therefore too demanding for the average person. Furthermore, since a person must meet all of the criteria to be judged normal this also makes the whole definition very demanding. |
|
|
What is statistical infrequency theory's definition of abnormality? |
this definition is based on the idea that certain behaviours are statistically rare in the population. For example, having an IQ of over 130. |
|
|
What effect does desirability have on statistical infrequency theory? |
this definition doesn't allow us to identify what behaviours require treatment. It overlooks desirability; some statistically abnormal behaviours are undesirable, whereas others are desirable (high IQ). To treat mental disorders we need a definition to include behaviours that are not only statistically rare but also those that are undesirable and damaging. |
|
|
How much does a characteristic have to deviate from statistical infrequency? |
A problem with statistical infrequency is deciding how much a behaviour must deviate from the average before it should be considered abnormal. Statistical definitions rely on an arbitrary cut off point, which might be in terms of standard deviations. |
|
|
What affect does time have no statistical infrequency? |
a further problem is that we find that behaviours are not rare at a given time in a particular culture even though they are clearly abnormal in the sense of being undesirable. For example genocides. |
|
|
What is a phobia? |
a phobia is a disorder in which a fearful anxiety occurs in response to specific objects or situations. Although it may be acceptable to show a fear reaction in a threatening situation, the phobic person shows a marked and persistent fear out of all proportion to the actual danger posed by the situation. The sufferer recognises that this reaction is beyond voluntary control and is unreasonable and excessive, and can only be endured with extreme anxiety or stress |
|
|
What are the three categories of phobia? |
- Specific phobia - Social phobia - Agoraphobia |
|
|
What is a specific phobia? |
suffered are anxious in the presence of a particular object or specific situation. For example: spiders, blood and heights. |
|
|
What is a social phobia? |
suffers experience inappropriate anxiety in social situation. Simply thinking about them causes anxiety. For example: meetings, restaurants etc. |
|
|
What is a agoraphobia? |
sufferers are anxious when they are in a situation that they cannot easily, such as when they are in open spaces or a crowd. |
|
|
What are the behavioural characteristics of phobias? |
A phobic person may panic in response to the presence of the phobic stimulus. Panic may involve a range of behaviours including crying, screaming or running away. Children may freeze. Sufferers will make a conscious effort to avoid coming into contact with the stimulus.Suffers will experience high levels of anxiety whilst in contact with the stimulus which may prevent normal everyday activity. |
|
|
What are the emotional characteristics of phobias? |
Phobias are classed as anxiety disorders as they involve an emotional response of anxiety and fear. Anxiety is an unpleasant state of high arousal and prevents the suffers from relaxing or feeling a positive emotion. |
|
|
What are the cognitive characteristics of phobias? |
suffers of phobias process information about phobic stimuli differently from other objects or situations. If a sufferer can see the phobic stimulus it is hard to look away from it.Keeping our attention on something dangerous is a good thing but it is not useful when the fear is irrational. A phobic may hold irruption beliefs. |
|
|
What is depression? |
depression is an affective mood disorder involving a lengthy disturbance of emotions. About 20% of people will suffer from some form of depression. |
|
|
What are the two types of depression? |
major depression (unipolar): reactive depression and endogenous depression bipolar depression (manic depressive) |
|
|
What is major depression? |
- The diagnosis requires five symptoms to occur everyday for a minimum of two weeks. - It is a form of depression occurring without mania. |
|
|
What is unipolar depression? |
- normally occurs in cycles - characterised by clinical symptoms - less common than unipolar (2% suffer) - also involves manic episodes |
|
|
What are the behavioural symptoms of unipolar depression? |
- loss of energy (reduced energy resulting in fatigue and lethargy) - social impairment (reduced levels of social interactions) - sleep pattern disturbance (constant insomnia or over sleeping) - weight changes (significant increase or decrease) |
|
|
What are the emotional symptoms of unipolar depression? |
- loss of enthusiasm (lessens concern without daily activities) - constant depressed mood (overwhelming feelings of sadness) - worthlessness (constant feelings of reduced worth and inappropriate feels of guilt) |
|
|
What are the cognitive symptoms of unipolar depression? |
- delusions (concerning punishment, personal inadequacy,disease) - reduced concentration (difficult paying attention to things - suicidal thoughts (these thoughts can be constant) - poor memory (difficult in retrieving information) |
|
|
What are the behavioural symptoms of bipolar depression? |
- high energy levels (boundless energy giving high work input) - reckless behaviour (dangerous and risk taking) - talkative (endless speech without regard for others) |
|
|
What are the emotional symptoms of bipolar depression? |
- elevated mood (intense feelings of euphoria) - irritability (frustrated if they don't get their own way) - lack of guilt (social inhibition) |
|
|
What are the cognitive symptoms of bipolar depression? |
- delusions (delusional and grandiose thinking) - irrational thought process (irrational decision making) |
|
|
What is reactive unipolar depression? |
it is caused by a stressful event such as the death of a close friend. |
|
|
What is endogenous unipolar depression? |
caused from within the person, for instance it may be due to hormonal imbalances |
|
|
What is obsessive compulsive disorder? |
characterised by obsessive thinking and compulsive behaviour in the form of rituals. Majority of patients suffer from high levels of anxiety - the obsessional thoughts create anxiety in which their compulsive behaviour tries to reduce this anxiety |
|
|
What are the behavioural symptoms of OCD? |
- hinder everyday functioning (obsessive ideas of a forbidden or inappropriate type creates such anxiety that the ability to perform everyday functions is hindered) - behaviours are repetitive - social impairment (anxiety levels are high resulting in inability to conduct interpersonal relationships) |
|
|
What are the emotional symptoms of OCD? |
- extreme anxiety (persistent inappropriate and forbidden ideas create excessively high levels of anxiety) |
|
|
What are the cognitive symptoms of OCD? |
- recurrent thoughts (constantly repeated obsessive thoughts of an intrusive nature) - recognised as self generated (understand obsessions are self invented) - realisation of inappropriateness (understand but cannot control) - attentional bias (perception tends to be focussed on anxiety generating stimuli) |
|
|
What are the classification systems of OCD? |
- DSM-IV: recurrent obsessions or compulsions, past or present recognition that the obsessions or compulsions are excessive or unreasonable, obsessions or compulsions cause marked distress - ICD-10 |
|
|
Are obsessions in internal or external |
internal because they are thoughts |
|
|
Are compulsions internal or external? |
external because they are behaviours |
|
|
What does the genetic explanation of OCD suggest? |
there appears to be a genetic link with people who develop OCD. This is shown in familial studies. |
|
|
What are the 2 specific genes implicated in OCD? |
COMT gene SERT gene |
|
|
What does the COMT gene do related to OCD? |
codes for an enzyme which has the function of breaking down dopamine. A variant of the COMT gene has been found in OCD. This variant produces less enzyme so dopamine is higher |
|
|
What does the SERT gene do related to OCD? |
the SERT gene codes for a protein that transports serotonin. Some OCD suffered have been found to have a mutation of this gene which creates lower levels of a neurotransmitter, serotonin. |
|
|
Which two areas of the brain does the neural explanation of OCD believe are implicated with the illness. |
- orbitofrontal cortex - basal ganglia |
|
|
How is the orbitofrontal cortex implicated with OCD? |
- part of a brain circuit that turns sensory information into thoughts and actions - important part of brain for controlling compulsive behaviour. People with OCD may have an impaired OFC so this mechanism is lost. |
|
|
How is the basal ganglia implicated with OCD? |
- group of structure linked to the thalamus (for coordination of movement) - OCD is often seen in Parkinsons and Tourettes are more likely to have similar symptoms - people who have accidents involving the basal ganglia can induce OCD symptoms - Max et al |
|
|
What are the 2 main neurotransmitters associated with OCD? |
Serotonin Dopamine |
|
|
How does Serotonin affect OCD patients? |
OCD is linked to low serotonin levels. Serotonin plays a role in preventing the repetition of tasks. |
|
|
How does Dopamine affect OCD patients? |
there is a less clear link between OCD and dopamine. High levels of dopamine may contribute to OCD. |
|
|
What evidence is there to support the role of genetics in OCD? |
Familial studies have shown that relatives of OCD sufferers have a greater tendency to suffer from OCD and anxiety related problems. Nedstadt et al (2000) found that first degree relatives of OCD suffered had an 11.7% chance of developing the disorder compared to 2.7% of controls |
|
|
Explain how twins have been used to investigate the role of genes in OCD sufferers |
Monozygotic (MZ) twins share 100% of their DNA. If OCD was genetic, both twins would develop OCD however Miguel et al (2005) found that the concordance rate for MZ twins was 53 - 87% suggesting that although it is not the sole cause of OCD it does play a key role in the development of OCD. |
|
|
Explain the meta-analysis of the 14 twin studies of OCD |
MZ twins (share 100% of dna) are more than twice as likely to develop OCD is their co twin has the disorder in comparison with DZ twins (share 50% of dna). Shows that genetics are not a sole contributor, environmental factors are vital in the development of OCD. |
|
|
What was Menzies (2007) study about neural explanations of OCD? |
He used MRI to produce images of brain activity in OCD patients and their immediate family members without OCD and a group of unrelated healthy people. OCD patients and their relative had reduced grey matter of brain areas including the orbitofrontal cortex. This supports the idea that anatomical differences are inherited and may lead to OCD in certain individuals. |
|
|
Evaluation of the basal ganglia in neural explanations of OCD |
the relationship between OCD and the functions of the basal ganglia are not straightforward. Although nuero-imaging studies have so far failed to identify basal ganglia impairments in all OCD suffers, a review of brain scan imaging found that the orbital frontal region has consistently been elevated in OCD patients compared to controls. |
|
|
What evidence is there to support the role of serotonin in OCD? |
Thoren et al (1980) found increased levels of 5-HIAA in the cerebrospinal fluid of people with OCD. 5-HIAA is the main metabolite of Serotonin. Following successful treatment, levels of 5-HIAA were discovered to decrease |
|
|
How do SSRI's effect OCD? |
Serotonin Reuptake Inhibitors increase levels of serotonin and are beneficial for some OCD sufferers. Furthermore, mCPP can induce OCD like symptoms in users and worsen symptoms in people who already have OCD. Effects of mCPP are found to reduce with SSRIs. |
|
|
How do SSRI's help treat OCD patients? |
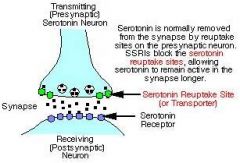
SSRIs prevent Serotonin from chemically diffusing across the synapse by binding to the re uptake site and therefore increasing the amount of serotonin |
|
|
What are the negative effects of SSRI's? |
- They can take several months to start working therefore this is not useful for someone experiencing severe distress - Unsuccessful in treating all OCD sufferers which suggests cause of OCD is not solely low serotonin levels - SSRI's have unpleasant side effects e.g. upset stomach - Many suffered relapse after stopping medication |
|
|
How do BZ's work in treating OCD patients? |
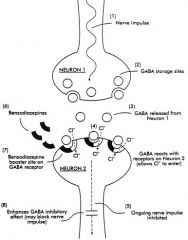
- Benzodiazepines enhance the activity of the neurotransmitter GABA. - GABA slows down the activity of many neurones in the CNS = a calming effect |
|
|
How does the behavioural approach believe phobias are acquired and maintained? |
They are acquired through classical conditioning and are maintained through operant conditioning |
|
|
Explain Watson and Raynor's (1920) experiment of Little Albert |
A baby, little Albert, was conditioned to fear a white rat. This was through associating a neutral stimulus with a fear response. UCS (loud noise) --> UCR (fear) NS (rat) + UCS (loud noise) --> UCR (fear) CS (rat) --> CR (fear) |
|
|
What is the positive evaluation for operant conditioning? |
Ohman et al 1975 Little Albert Study Phobias through observation |
|
|
What is the negative evaluation for operant conditioning? |
- Ethical issues of the Ohman et al 1975 study - Association - Non behaviourist framework |
|
|
What is the aim of all behavioural therapies? |
to remove the conditioned association between the fear and the situation/object |
|
|
What is systematic desensitisation? |
Developed by Joseph Wolpe (1958) - one cannot be in a state of relaxation and fear simultaneously. |
|
|
How does systematic desensitisation work? |
1. first step is to each the sufferer relaxation techniques e.g. focusing on breathing and progressive muscle relaxation 2. a hierarchy of fear is then developed 3. over a period of sessions the patient is taken through their hierarchy whilst associating these fears with deep relaxation |
|
|
What is the goal of systematic desensitisation? |
to reach the top item on the hierarchy whilst remaining in a state of relaxation |
|
|
What is the process of flooding? |
involves putting the phobic individual in a situation where they would be forced to face their phobia |
|
|
What is the negative evaluation for behavioural therapies? |
requires exposure to the stimulus highly stressful procedures may not work with many phobias |
|
|
What is the positive evaluation for behavioural therapies? |
SD is successful for a range of phobias Relatively quick Both effective Most effective when possible to identify a particular object |
|
|
What does the cognitive approach assume about depression? |
the cause of abnormality is irrational and distorted thoughts or beliefs |
|
|
What is depression according to Beck 1967? |
a disorder of thought rather than mood. It is a result of how an individual thinks about themselves, their world and their future. This is called the negative triad. |
|
|
When does the model propose the foundations for thinking this way are laid? |
childhood as a result of unhappy experiences so individuals develop negative schemas that lead to automatic negative thoughts. Events in everyday life can trigger memories in an individual of the circumstances that first led them to acquire negative schemas |
|
|
What 5 things does Beck believe a person with depression will subconsciously do? |
overgeneralisation personalisation minimisation magnification selective abstraction |
|
|
What did Ellis 1987 believe about depression? |
emotional problems and associated maladaptive behaviour is the result of irrational thinking. It is not a life event that causes difficulty but the way we think about them. |
|
|
Explain Ellis' 1987 ABC |
ACTIVATING EVENT: according to Ellis we get depressed when we experience negative events and these trigger irrational beliefs. Events like failing a test or ending a relationship BELIEFS: Ellis identified a range of irrational beliefs. Some beliefs are bad on achieving perfection and always succeeding, whereas others include the belief that their is a major disaster when something doesn't go smoothly CONSEQUENCES: when an activation event tigers irrational beliefs there are emotional and behavioural consequences. |
|
|
What did Beck and Clark 1988 believe about depression? |
certain individuals are vulnerable because they have a certain negative way of thinking i.e. schemas developed as a result of negative experiences. These schemas are triggered by environmental events. Individuals who use there schemas engage in safety seeking behaviours which prevent them for realising the irrationality of their thoughts |
|
|
What is the economic impact of research into abnormality? |
if we can reduce the problems by research we can find the cause of illnesses and effective treatments which will save money |
|
|
What is cognitive behavioural therapy? |
most commonly used psychological treatment for depression. CBT begins with an assessment in which the patient and therapist work together to clarify the patients' problems and identify goals for the therapy. |
|
|
What is the aim of CBT? |
to identify and challenge any irrational beliefs the patient may have |
|
|
What was the key aim of Beck's CBT? |
identify and challenge negative automatic thoughts about self, world and future. |
|
|
What was Ellis' rational emotive behaviour therapy? |
REBT extends the ABC model. D stands for dispute and E stands for Effect. |
|
|
What was the key aim of REBT? |
identify and disput irrational beliefs |
|
|
What is the negative evaluation for CBT? |
- REBT may not be effective for all patients - Severe depression means some patients cannot motivate themselves to engage with CBT - Risk of neglecting environmental factors - Neglects what happened in the past |
|
|
What is the positive evaluation for CBT? |
- Large amount of research to support the effectiveness CBT for depression - 90% success rate for REBT - Cujipers et al 2013 - CBT is a humane way with dealing with abnormality |