![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
29 Cards in this Set
- Front
- Back
|
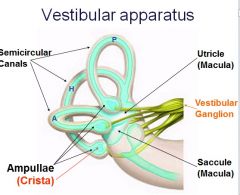
Describe the vestibular apparatus |
|
|
|
What is the ampullary cupula? |
Structure in the vestibular system in ampulla of each of 3 semicircular canals. Provides sense of spatial orientation due to inertia of endolymph |
|
|
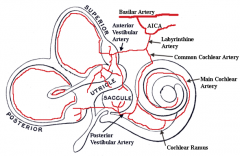
What is the blood supply to the vestibular system? |
|
|
|
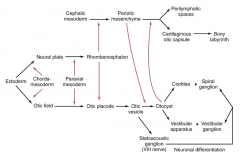
What is the embryological development of the vestibular system? |
|
|
|
From where are the otic vesicles derived, embryologically? |
Thickened otic placodes -> otic pits |
|
|
By what days have the semi-circular ducts differentiated, and what day is the vestibular system fully formed? |
Differentiated - 50 days Fully formed - 56 days |
|
|
What are 3 functions of the vestibular system? |
Detection & conscious perception of head position, movement & gravity
Compensatory eye movements during head movement (image stabilization & tracking)
Postural reflex adjustments following head movements |
|
|
Where do the ascending and descending branches of the vestibular nerve go? |
Ascending - medial lemniscus -> VPM nucleus in thalamus -> CC, to III, IV, VI nuclei
Descending - to cerebellum through vestibular nuclei and inferior peduncle, to vestibulospinal tract |
|
|
What is the connection of the vestibular nuclei to the occulomotor nuclei? To the thalamus? To the cervical spinal cord? To the lumbar spinal cord? To vestibulo cerebellum? |
MLF to III
ML to thalamus
Medial VST - head stabilisation - to cervical
Lateral VST - antigravity - to lumbar
Inferior CP to vestibulocerebellu, |
|
|
What are the motion detectors and vestibular receptors for angular/rotational acceleration and linear acceleration/decelleration? |
Angular (rotational) acceleration: Semicircular canals Vertigo (rotational sensation)
Linear acceleration/deceleration: Utricle & saccule Dysequilibrium (rocking ship sensation) |
|
|
How is rotational acceleration/deceleration detected? |
Deflection of stereocilia towards kinocilium results in increase in firing of vestibular fibre associated with hair cell. Deflection away results in decrease firing rate.
Hair cells have 1 large kinocilium and several small stereocilia. |
|
|
What are features of rotational acceleration/deceleration? |
Canals on either side of head act in a push-pull rhythm Excitation is towards side of rotation Push-push rhythm causes nausea & vertigo Nerve damage causes vertigo & nystagmus due to afferent imbalance. |
|
|
What is the vestibulo-ocular reflex? |
Downwards movement of head - increased IO + SR, decreased SO IR
Upwards - decreased SR, IO, increased IR, SO.
Head moves right, increased firing of right LR to IV nucleus, increased firing in left side cupula. Decreased firing of right |
|
|
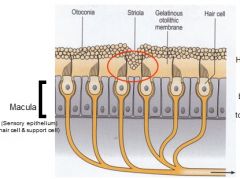
Describe the anatomy of the utricle/saccule. |
|
|
|
How are the hair cells of the macula excited? |
Hair cells of the maculae are excited (or inhibited) by bending of the stereocilia toward (or away from) the kinocilium by opening or closing potassium channels |
|
|
How are the hair cells polarised in the utricles/saccules? N.B. UTRICLES - MEDIOLATERAL SACCULES - ANTEROPOSTERIOR |
Utricles - hair cells are polarized (excited) towards the striola which divides each macula into medial and lateral halves
Saccules - hair cells are polarized away from the striola (divides each macula into anterior and posterior halves)
The hair cells of the utricles and saccule work together to provide for a three dimensional representation of the direction of linear force. |
|
|
What is the function of the macular? |
Maculae detect linear acceleration, deceleration, tilt & effects of gravity |
|
|
What is perilymph, what is the difference between scala tympani and scala vestibuli perilymph? |
Perilymph is a typical extracellular fluid (~ plasma or CSF). The compositions of ST perilymph and SV perilymph are not the same; SV perilymph has higher K+ and lower Na+ levels.
Endolymph is a unique extracellular fluid, with an ion composition - bicarb CHLORIDE POTASSIUM - NO SODIUM |
|
|
What is nystagmus? |
Is an uncontrolled oscillation of the eyes Has a slow phase and a fast phase Direction of nystagmus is specified by direction of fast phase Slow phase is VOR (for image tracking) Fast phase due to cortically derived signal (to allow another object to be tracked) |
|
|
What is normal/abnormal nystagmus? |
Normal - optikokinetic i.e. fixation nystagmus Abnormal - spontaneous nystagmus - abnormal due to damage to vestibular apparatus, brainstem or cerebellum. |
|
|
What is the head righting reflex? |
1. Vestibular neurones <- signals of changing head position from utricle and saccule - signals on forward rotational accel from vertical SC canals 2. MVST neurones process and transmit inhibitory signals to neck flexors 3. Excitatory signals sent to neck extensors - neck movement upwards opposite falling motion
|
|
|
What is rotational nystagmus? |
On abrupt cessation there is a post rotational nystagmus as the SSC endolymph does not stop as quickly and so nystagmus appears in the opposite direction which lasts a few seconds (<15s) |
|
|
What are symptoms and signs of nystagmus? |
Vertigo Syncope Dysequilibrium - rocking ship Oscillopsia - visual jumping/blurring Nystagmus N&V Ataxia Hearing loss, tinnitus - cochlear symptoms |
|
|
What are causes of nystagmus? |
Nerve/inner ear infections Tumours Vascular insufficiency Trauma Endolymph fistulae
BPPV, Meniere's disease, Drug toxicity - quinine & aminoglycloside, Usher's syndrome |
|
|
How do you test for vestibular disorders? |
Eye movements Caloric testing Hallpike manouevre, electronystography, posturography, bárany chair, MRI |
|
|
What is the caloric test? |
Cold water decreases ipsilateral ampulla firing, therefore OPPOSITE, warm increases - SAME COWS - normal |
|
|
What happens to the caloric test if patient is unconscious/has a bilateral MLF lesion? |
Unconscious - cold = same, warm = opposite - no F phase due to lack of input from cortical gaze centres.
Bilateral MLF lesion - cold = ipsilateral eye only - opposite, warm = contralateral eye only - same |
|
|
What is the hallpike manouvre and what does it test for? |
Lower head to table and turn to side, watch for nystagmus, patient is dizzy and exhibits nystagmus - ear pointed to the floor is the affected ear.
Sign of BPPV |
|
|
What is BPPV? N.B. Epley's procedure also tests |
Vertigo due to damaged otoconia from the utricle being displaced into the semicircular canals within the inner ear.
Otoconia from the saccule are not able to migrate into the canals.
The utricle can be damaged by head injury, infection, or other disorder of the inner ear, or may have degenerated because of advanced age. |