Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
67 Cards in this Set
- Front
- Back
|
6 month-old male
Recurrent otitis media Pneumocystis pneumonia Diagnosis |
Recurrent otitis media-->humoral (B cell) deficiency bc can't mount reaction against strep pneumo, h. flu
PCP pneumonia indicates T cell deficiency (which is why this is usually found in people with AIDS) Thus, pt has Severe Combined Immune Deficiency--will see lymphopenia and hypogammaglobulinemia (bc no B cells!) on labs |
|
|
Candida skin test gauges a delayed hypersensitivity reaction.
What cells are required for the response? |
CD4 helper cells
CD 8 cytotoxic cells NKCs Failure to generate a response to this test = anergy, as in SCID |
|
|
Characteristic liver finding of Reye Syndrome.
|
Microvesicular steatosis
|
|
|
Patient is unable to tolerate everyday sounds.
What CN is injured? |
Facial Nerve
Stapedius is innervated by branch of CN VII; paralysis of stapedius allows stapes to oscillate more widely, producing hyperacusis (inc'd sensitivity to sound) Ipsilateral hyperacusis is a common finding in Bell's palsy |
|
|
43 year-old man with abdominal cramps
Small bowel biopsy reveals nests of mast cells within mucosa What is causing his abdominal cramps? |
Gastric acid is secreted by parietal cells which are stimulated by histamine, Ach, gastrin.
In systemic mastocytosis, MAST CELL PROLIFERATION occurs in BM and in other organs. Inc'd histamine secretion will cause GASTRIC HYPERSECRETION OF ACID-->inactivates pancreatic/intestinal enzymes-->diarrhea, may also have gastric ulcerations Will also see syncope, flushing, hypotension, tachycardia, bronchospasm, and pruritius |
|
|
The neurofibromas of neurofibromatosis are derived from ________.
|
Neural crest
|
|
|
Most common site of colon cancer
|
Rectosigmoid colon
|
|
|
51 year-old female presents with symptoms of hypothyroidism. No history of viral illness.
What is the most likely cause and what histologic changes would you see in the thyroid? |
This is Hashimoto's
You'd see mononuclear infiltration consisting of lymphocytes and plasma cells. There are several germinal centers present. |
|
|
6-mercaptopurine and 6-thioguanine inhibit de novo purine synthesis after conversion to active metabolites by __________.
What degrades these active metabolites? What drug can be given to prevent their degradation? |
6-MC become active after interacting with HGPRT
Degradation then results from XANTHINE OXIDASE can give a xanthine oxidase inhibitor like allopurinol |
|
|
56 year-old homeless man
Increased fatigability, exertional dyspnea Significant lower extremity edema Decreased sensation over ankles and feet Cardiac dilation What vitamin is deficient? |
This is wet beriberi: neuropathy + cardiac involvement (as opposed to dry which is neuropathy + motor impairments of distal extremities)
Due to deficiency of thiamine--vitamin B1 |
|
|
15 year-old male
Presents with periodic, sudden onset, arrhythmic jerking movements FMH positive for seizure disorder Diagnosis Treatment |
Pt is experiencing myoclonic seizures (may be confused with motor and phonic tics of Tourette Syndrome, which would be treated with haloperidol)
Treatment would be: valproate |
|
|
Provide drug of choice for:
Partial Seizures Tonic-Clonic Seizures Myoclonic Seizures Absence Seizures |
Partial (simple or complex)--carbamazepine
Tonic-Clonic: Phenytoin, carbmazepine, valproate Myoclonic: Valproate Absence: Ethosuximide, followed by valproate NOTE: VALPROATE INHIBITS Na and K+ Channels (in addition to affecting GABA and NMDA receptors) |
|
|
Which bacteria grow on:
Thayer-Martin VCN (vanco, polymixin, nystatin) |
Neisseria
|
|
|
Which bacteria grow on:
Blood agar containing bile and hypertonic saline |
Enterococci
E. faecalis/faceium |
|
|
Which bacteria grow on:
Cysteine-tellurite agar |
Corynebacterium diphtheriae
|
|
|
Which bacteria grow on:
Bordet-Gengou medium |
Bordetella pertussis
|
|
|
Salmonella vs Shigella:
Method of causing disease (site of invasion, spread, etc.) Which produces H2S gas on triple sugar agar? |
Salmonella:
(and yersinia) penetrate bowel mucosa, gain access to lymphatics, and proliferate in LNs Does release gas Shigella: Mucosal invasion, inactivation of 60S ribosomes Doesn't release gas |
|
|
Protein M is the major virulence factor for ______.
What is its effect? |
Protein M is major virulence factor for Strep pyogenes
inhibits phagocytosis and activation of complement |
|
|
Zolpidem:
Why is it a better choice than benzodiazepines for treating insomnia? How does it work? |
Zolpidem, like benzos, bind and enhance the inhibitory action of GABA on Gaba-A receptor)
It's preferred to benzos because is has less potential for tolerance and addiction. Much lower incidence of withdrawal syx. No muscle relaxing effects, no anticonvulsant props. Note: Zolpidem = AMBIEN |
|
|
Patient's PTT is unaffected by addition of activated Protein C.
Diagnosis. |
Factor V Leiden mutation--protein C normally renders Va inactive. But the mutation prevents this from happening.
|
|
|
How does presentation of acute HBV differ from acute HCV?
|
Acute HBV presents with serum sickness: fever, fatigue, joint pain, urticaria, malaise
Acute HCV is mild, though some may complain of malaise, nausea, or RUQ |
|
|
An inactivating mutation in this enzyme of glycolysis will not allow pancreatic beta cells to detect intracellular glucose.
|
Glucokinase (hexokinase in every other cell)
This mean less insulin will be released, and pt will be prone to hyperglycemia. This is a common mutation in people prone to gestational diabetes. (No G6P means glucose is free to leave cell) |
|
|
ID the fungus:
Spherules packed with endospores |
Coccidoides--southwestern US
|
|
|
ID the fungus:
Pigeon droppings |
Cryptococcu
|
|
|
ID the fungus:
Bat/Bird droppings |
Histoplasma (Ohio River Valley)
|
|
|
What clotting factor does vWF carry?
|
VIII OCHO OCHO OCHO VANWILLEBRANDO
will see prolonged PTT bc of this |
|
|
Ristocetin aggregation test:
How does it work? What is it testing? |
vWF:
Ristocetin activate GP Ib-IX receptors on PLTs and makes them available for vWF binding When vWF is dec'd, there is poor PLT aggregation in presence of ristocetin |
|
|
This opioid drug will cause withdrawal symptoms in those that are dependent on morphine.
|
Pentazocine
|
|
|
BRAF mutations are associated with _______.
|
Melanoma
|
|
|
Prostacyclin effects
|
Vasodilates
Inhibits PLT aggregation Increases vascular permeability |
|
|
Treatment of severe hypoglycemia (inducing loss of consciousness):
In non-medical setting In medical setting |
In non-medical setting: intramuscular GLUCAGON (increases hepatic glycogeneolysis and gluconeogenesis)
in hospital intraVENOUS glucose (never give glucose I.M.) |
|
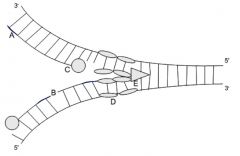
Label
|
A - RNA primers formed by DNA-dependent RNA polymerase
B - Ligase enzyme which binds fragments of lagging strand C - DNA polymerase III D - Single Strand BPs E - Helicase: binds ssDNA at origin of replication, moves into replication fork, and proceeds to separate and unwind DNA |
|
|
64 year-old man
Easy fatigability Constipation Bone pain Renal failure with eosinophilic casts Diagnosis Explain presentation |
Multiple myeloma:
Easy fatigability due to anemia Constipation due to hypercalcemia Bone pain due to produciton of osteoclast activating factor by myeloma cells Renal Failure--secondary to hypercalcemia, AL amyloidosis, hyperuricemia, excess free light chains (BENCE JONES PROTEINS) |
|
|
34 year-old man in a MVA
Suffers from excessive thirst, frequent urination Urinary osmolality after 2 hour-water restriciton is 250, but increases to 700 after ADH injection Patient denies polyphagia What is damaged? |
Hypothalamic nuclei!!!
Damage to posterior pituitary gland produces only transient polyuria. Diabetes insipidus usually results from damage to hypothalamic nuclei or pituitary stalk. |
|
|
32 year-old male
Hospitalized with internal bleeding following MVA Successfully resuscitated, but develops oliguria What happened? What's his prognosis? |
Acute Tubular Necrosis from internal hemorrhage
In short, kidney function shuts off for a few days, slowly recovers to full function over few weeks here are the distinct phases: Initiation: original insult (ischemia)-->cell damage begins to evolve; GFR begins to fall and urine output decreases During maintence (oliguric) phase, renal tubule injury established, GFR stabilizes well below normal; will see GRANULAR CASTS in tubules, along with tubules epithelial NECROSIS, denudation of its BM also Recovery: RE-EPITHELIAZATION of tubules Polyuria and gradual normalization of GFR-->complete restoration of renal function MAY SEE INTERTSTITIAL SCARRING ON LIGHT MICROSCOPY |
|
|
Bacterial cause of repeated pulmonary infections in cystic fibrosis
|
Pseudomonas
|
|
|
Loss of anterior horns of spinal cord (__MN lesion)
+ Loss of lateral corticospinal tract (___MN lesion) = Diagnosis |
Anterior horns = LMN
Lateral corticospinal tract = UMN If have both UMN and LMN lesions-->amyotropic lateral sclerosis |
|

Esophageal biopsy:
Diagnosis Prognosis |
These are KERATIN PEARLS-->squamous cell carcinoma
Note that since there are keratin pearls, this tumor still retains some of its original tissue, in other words, it's well-differentiated. Most important risk factors are EtOH and tobacco use. Usually evolves into progressive dysphagia as tumor gradually obstructs esophageal lumen. Significant weight loss common. Poor prognosis. |
|
|
Effect of initial and prolonged efferent renal arteriole constriction on:
GFR FF |
GFR: Selective vasoconstriction of efferent arteriole increases hydrostatic pressure in glomerular capillaries, and therefore, increases GFR. As efferent arteriolar constriciton increases, there is inc'd oncotic pressure in glomerular capillaries, which decreases GFR.
FF which = GFR/RPF always increases with efferent constriction bc: -GFR increases -RPF (rate at which plasma flows through glomerulus) increases |
|
|
What does it mean when an anesthetic has a high blood/gas partitioning coefficient?
|
It means it's highly soluble in the blood (blood:gas partition). Drugs with high coefficients are more soluble in blood and demonstrate slow onset of action and slow equilibrium with brain.
|
|
|
Schilling test results by phase.
|
1) B12 PO and radiolabeled B12 IV-->if you pee out radiolabeled B12, you have normal absorption, and that means you have a dietary deficiency
If don't pee out, move onto step 2: 2) Radioactive B12 and IF: If pee out radioactive B12, have pernicious anemia If don't pee out, heave malabsorption syndrome, such as panc insuff, bacterial overgrowth, or short gut syndrome |
|
|
Partial vs Complete Mole
-Karyotype -Risk of cancer |
Partial Mole: 69 XXX or XXY, LOW RISK of malignancy
Complete Mole: 46XX or XY (of PATERNAL ORIGIN) 15-20% risk malignancy THis is the one that looks like a bunch of grapes. May experience pre-eclampsia, hyperthy |
|
|
Effect of chronic smoking on diffusing capacity.
|
Smoking decreases diffusing capacity because of alveolar destruction (and destruciton of adjoining capillary beds)
|
|
|
This beta-agonist both increases cardiac contractility and decreases vascular resistance.
How? |
Isoprotenolol:
Increases cardiac contractility by acting on beta-1 receptors At low does, selectively binds beta-2 receptors, causing RELAXATION of vascular smooth muscle |
|
|
Patient with myasthenia gravis takes neostigmine.
Given low-dose edrophonium: -Can either elicit significant improvement or have no effect How would either outcome change your care? |
If edrophonium (Tensilon test)--a short-acting cholinesterase inhibitor--improved syx, you'd increase dose of neostigmine
If it had no effect, she's receiving too much neostigmine and you'd stop it temporarily (note: inappropriately high doses of cholinesterase inhibitors-->excessive ACh in synaptic cleft-->NMJ becomes insensitive to ACh) |
|
|
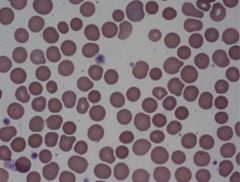
Spherocytes!
Hereditary spherocytosis (RBC cytoskeleton abnlts, most commolny spectrin and ankyrin abnlts) Hemolytic anemia, jaundice, splenomegaly are classic findings Can also find out through osmotic fragility testing |
|
|
Pralidoxime:
What is it good for? |
Will help regenerate acetylcholinesterase; used for ORGANOPHOSPHATE POISONING
|
|
|
Where is alpha-1 antitrypsin formed?
Besides emphysema, what's another concern for individuals homozygous for the deficiency? |
Formed in the liver
Worry about liver dz; homozygous individuals usually demonstrate hepatomegaly, HSM, cholestasis, elevation of hepatocellular enzymes h/o neonatal hepatitis w/cholestasis should heighten suspicion for A1AT deficiency |
|
|
9 year-old girl with positive ASO titer. Experiences joint pain/swelling after sore throat. NOw has holosytolic murmer.
She dies. What did she die from? |
This patient has acute rheumatic fever and likely died of severe myocarditis.
Note that acute renal failure is a possibility, but that it rarely is fatal. |
|
|
What is myofibril relaxation a sign of?
|
Reversible injury in cardiac myocytes--occurs within the first 30 minutes of severe ischemia
Corresponds w/intracellular ATP depletion and lactate accumulation due to anaerobic glycolysis during this period |
|
|
When does mitochondrial vacuolization occur?
|
SIgn of irreversible cell injury (death)
SIgnifies that involved mitochondria permanently unable to generate ATP |
|
|
BP drops 10mmHg on inspiration
|
Pulsus Paradoxus
TAMPONADE |
|
|
Inherited Pulmonary Artery Hypertension:
Genetic pathophys |
ABnormal morphogenic protein receptor type 2 (BMPR2) = first insult
Second insult (infect, drugs, ion channel defects) activates dz process, increasing endothelin (vasoconstrictor), decreasing nitric oxide (vasodilator), and decreasing prostacyclin (vasodilator, platelet inhibitor) Result i vasoconstriction, vasc SM proliferation, fibrosis, thrombosis of pulmonary arteries and arterioles, endothelial cell growth, and elevated pulmonary pressures. Can lead to RVH-->cor pulmonale |
|

Diagnosis
Cause |
Dilated superficial veins (varicose veins) and associated skin changes consistent with stasis dermatitis
Incompetent venous valves in lower extremities allow retrograde blood flow from deep to superficial. Increases the pressure in the superficial veins leading to their dilation. |
|
|
Medulloblastoma vs Pilocytic Astrocytoma:
Pathologic Differences (on slides) |
Medulloblastoma: Sheets of primitive cells with many mitotic figures ("primitive neuroectodermal tumor"--SMALL, ROUND, BLUE CELLS. Abundant mitoses. Poor prognosis.
Pilocytic Astrocytoma: Rosenthal fibers, not blue at all. More pink. Note that these both occur in the cerebellum and can result in ataxia. |
|
|
The QRS complex corresponds to phase ____ of of the ventricular myocyte action potential.
|
Phase 0--when Na+ rushes in
|
|
|
34 year-old female
Proteinuria Facial rash Chest pain that increases with inspiration Radiates to trapezius ridge, partially relieved by sitting up Diagnosis Pathophys |
She has lupus: virtually all pts w/lupus have renal involvement
Inflammation of serous membranes is another common manifestation of lupus--it can cause pleuritis and pericarditis Pericarditis is very common in pts w/SLE Pain increases on inspiraiton (pleuritic) and relieved by sitting up and leaning forward (postural) Auscultation reveals a scratchy sound called a pericardial friction rub best heard when pt sitting upright and leaning forward |
|
|
What chemical signals pyruvate to become glucose?
i.e., acts as allosteric activator |
Acetyl CoA
|
|

Advanced HIV
Diffuse cortical atrophy Enlargement of ventricles Diagnosis |
Hydrocephalus ex vacuo: in diseases associated with cerebral atrophy (AD, Pick disease, etc), ventricular enlargement occurs secondary to brain atrophy.
Such compensatory ventricular expansion is called "hydrocephalus ex vacuo" Although distended ventriculi produce CT scan similar to true hydrocephalus, CSF pressure IS NOT INCREASED. Cortical atrophy is a common sequelae of advanced HIV infection. |
|
|
What two ACh structures in the brain are affected by AD?
|
Basal nucleus of Meynert
Hippocampus |
|
|
Histologic findings of renal artery stenosis caused by:
Malignant HTN Diabetes |
Malignant HTN: homogenous, onion-like, concentric thickening of walls of arterioles (results from laminated SMC and reduplicated basement membranes)
Diabetes: hyaline arteriosclerosis--arteriolar walls will be homogenously thickened and stain pink with hematoxylin-eosin. Hyaline usually result of excessive excessive ECM production by smooth muscle cells. |
|
|
Immune thrombocytopenia purpura:
Pathophys Presentation |
Autoimmune platelet destruction
Presents with ecchymoses, petechiae, mucosal bleeding, thrombocytopenia, but not signs of pancytopenia, marrow failure, or splenomegaly |
|
|
Muddy brown casts
|
Acute TUBULAR necrosis
|
|
|
Acute tubular necrosis often due to ischemia (as in the setting of blood loss):
What regions of the kidney are most susceptible to ischemia? |
Proximal tubules and thick ascending limp of Henle are locaed in outer medulla, an area that even under normal conditions has low blood supply.
In addition, proximal tubules and ascending limb participate in active transport of ions (ATP-consuming). When oxygen delivery to kidney is compromised, these portions of the nephron suffer first. Proximal tubules, Ascending Limb |
|
|
What is renal papillary necrosis associated with?
|
DM
Sickle CELL DISEASE |
|
|
Cancer risks of long-term asbestos exposure (most common and second most common)
|
Most common is bronchogenic carcinoma (greatly increased risk--90-fold increase in fact--if smoker)
Second-most common is mesothelioma (smoking does not increase risk of mesothelioma) |
|
|
What is the inciting event of appendicitis?
|
Obstruciton of lumen
Fecaliths (hard poop), foreign bodies, or tumors may cause obstruction Retained mucus causes appendicular wall to distent, impairs venous outflow; resulting hypoxia causes ischemia and associated bacterial invasion Inflammation and edema of appendicular wall occur, causing further distention. Necrosis may follow. Inflammatory fluid and bacterial contents spill into peritoneal cavity, causing peritonitis. |