Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
10 Cards in this Set
- Front
- Back
Acute scrotal pain
|
1. pain predominant
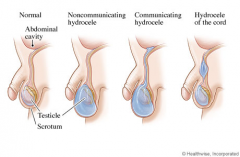
testicular torsion: medical emergency need surgical detorsion and orchiopexy(fixation of both testes) cremasteric reflex: positive if there is elevation of the testis in response to stroking the upper inner thigh It is negative in testicular torsion and boys < 6 months Negative cremasteric reflex and abnormal testicle lay are high suggestive of testicular torsion. Doppler U/S or nuclear scan of scrotum can help diagnosis of testicular torsion in the case of clinical uncertainity torsion of the appendix testis epididymitis: pain relief with scrotum elevation, not reliable for diagnosis, U/A is recommended for all suspected epididymitis, urethral swab is recommended for STD induced epididymitis 2. swelling predominant hydrocele: typically not painful positive translumination of scrotum, a cystic scrotal fluid collection between the parietal and visceral layers of the tunica vaginalis that can communicate, increased size during the day and with Valsalva maneuver |
|
|
Varicocele
|
Venous drainage of the testes involves a complex network of veins called the pampiniform plexus, which are responsible for keeping the temperature of the scrotal sacs below the normal body temperature. Seminiferous tubules make up most of the testicular mass, and are very sensitive to an ↑temperature .Dilation of the pampiniform plexus (varicocele) results in an ↑temperature of the scrotal sacs → testicular atrophy
Androgen-secreting Leydig cells are more resistant to an↑ in temperature caused by varicoceles therefore impotence is not common in varicocele. Varicoceles are more common on the left side because the left spermatic vein enters the left renal vein at a 90-degree angle. The right spermatic vein drains at a more obtuse angle directly into the inferior vena cava, thereby facilitating a more continuous flow. Processes that cause IVC obstruction(clot, tumor) should be ruled out in patients who have bilateral varicocele, right varicocles or varicocele that does not disappear in the supine postion (abdominal CT) |
|
|
Scrotal trauma
|
Surgical exploration should be performed immediately in scrotal trauma cases wherein there is evidence of significant trauma (hematoma)on PE.
|
|
|
Sphincter-sparing sugery for patients with rectal cancer
|
An important determining factor is the location of the tumor
Proximal non-metastatic rectal cancer --- lower anterior resection+radiation+chemo if node + Distal rectal cancer ---- local resection(spincter-sparing operation) if mobile, non-ulcerated and relatively small (<4cm) or abdomino-perineal resection (extensive radical operation) Patients with a big tumor are sometimes treated with preoperative irradiation and concurrent chemotherapy prior to a planned resection which may permit a spincter-preserving local resection |
|
|
Fat embolism
|
A clinical diagnosis, 24-72h after severe trauma
Triad: respiratory insufficiency + neurological impairment + petechial rash,(trunk) by occlusion of dermal capillaries by fat globules –extravasation of RBC, the rash is considered pathognomonic Can have fever, tachycardia and altered mental status. Ventilation/perfusion scans may demonstrate a mottled pattern of sub-segmental perfusion defects with a normal ventilatory pattern. Treatment: early immobilization + operative fixation of fractures |
|
|
Acute arterial occlusion
|
usually presents with five Ps: pain, pallor, pulselessness, paresthesias and paralysis. The sudden onset of symptoms in a previously asymptomatic patient is most likely due to an embolus while a history of gradually progressive symptoms in a previously symptomatic patient is consistent with thrombosis
Most of the emboli are from a cardiac source , with a few coming from the arterial aneurysms or atherosclerotic plaques. It is important to find the exact cause of cardiac emboli to prevent further recurrences. After an embolectomy, the surgical specimen should be sent for histological examination to ascertain the exact source of emboli. Atrial myxomas are the most common primary cardiac tumors (LA>RA>LV). The tumors are typically pedunculated with a stalk arising from the atrial septum. These can be extremely friable, resulting in embolization of the part of the myxoma to the systemic circulation. Some large tumors may initially present with signs and symptoms of mitral valve obstruction (diastolic murmur or tumor plop), rapidly worsening heart failure in otherwise young healthy individuals or new onset of AF. Once the diagnosis of atrial myxoma is made, it should be excised as soon as possible to reduce the risk of recurrent embolization |
|
|
Thyroglossal duct cyst
|
1/3 present after the age of 20
Midline neck mass that moves with protrusion of the tongue Have high chances of getting infected due to the connection with the oropharynx Ectopic thyroid tissue is present in a large number of patients within the thyroglossal duct cysts, but sometimes this is the only functional tissue present, so thyroid function assessment + imaging studies like a thyroid nuclear scan, U/S or CT is mandatory before subjecting of the patient to surgery, CT is more useful because it clarifies the anatomy of the thyroglossal duct cyst in relation to the surrounding structures |
|
|
Klinefelter’s syndrome
|
Related to gynecomastia (decreased testosterone-to-estrogen ratio, low testosterone levels→LH increase →increased estrogen)
The strongest known risk factor for male breast cancer, 50-fold increase |
|
|
Anal abscess
|
Glands that encircle the anus become blocked and the bacteria within grow unchecked.
Severe constant pain+/- fever/maaise PE: erythematous indurated skin or fluctuant mass over the peripheral or ischiorectal space Treatment: incision + drainage of the abscess + antibiotics (if DM, immunosuppressive, extensive cellulitis or valvular heart disease) Periana/small ischiorectal abscesses --- office Larger ischiorectal abscesses --- surgical intervention Complication: fistula from the involved anal gland to the overlying skin, require surgical repair (present with an anal abscess that persists after incision and drainage or pustule-like lesion in the perianal or ischiorectal area that conitually drains) |
|
|
Porcelain gallbladder
|
Calcium salt deposits in the wall of a chronically inflamed gallbladder + Thin/faintly visible /amorphous/patchy/thick calcification + Large gallbladder
Associated with gallstones Plain radiography can detect it (abdominal X-ray shows a curvilinear calcification in the right hypochondrium), CT can confirm the diagnosis (high sensitivity and specifity) Treatment: elective cholecystectomy due to high risk of gallbladder carcinoma |