![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
38 Cards in this Set
- Front
- Back
|
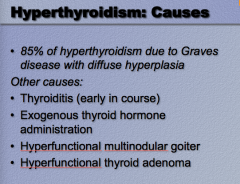
What is 85% of of hyperthyroidism due to? |
Graves disease with diffuse hyperplasia |
|
|
What are some other causes of hyperthyroidism? |
|
|
|
Outline the pathophysiology of Graves Disease: |

Immune mediated production of TSH receptor antibodies:
Antibodies bind to thyroid TSH receptors => thyroid stimulation without negative feedback
Same antibodies bind to other tissue sites => increased production with glycosaminoglycans => tissue effects (exopthalmos, myxedema) |
|
|
What are the signs and symptoms of Graves Disease? |
Pre-tibial myxedema = non-pitting edema Fatigue, weight loss, increased appetite, tachycardia, muscular weakness, exophthalmos |
|
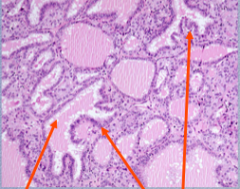
Identify what the arrows are points to.
The thyroid epithelium in Graves disease is _______ (too many cells present)
What is term used to describe the colloid? |
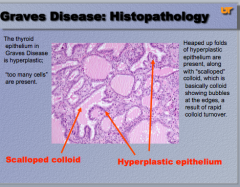
Scalloped |
|
|
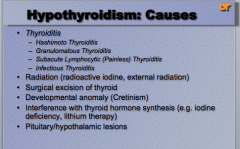
What are the four types of thyroiditis?
What are some other causes of hypothyroidism (radio, cut out, developmental, synthesis, pit) |
|
|
|
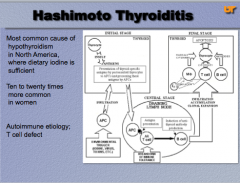
What is the most common cause of hypothyroidism in North America, where dietary iodine in sufficient?
Is it more common in men or women?
What is the autoimmune etiology? Draw the pathway. |
|
|
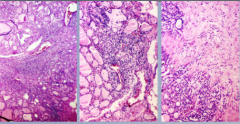
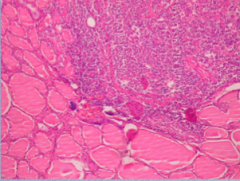
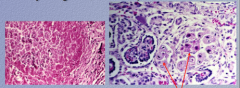
What is the disease? Identify each phase.
Why does early Hashimoto cause HYPERthyroidism while late disease is HYPOthyroidism? |
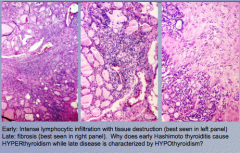
Early: lymphocytic infiltration Late: fibrosis (right panel) Disruption of thyroid follicles with subsequent release of thyroid hormones (hashitoxicosis) |
|
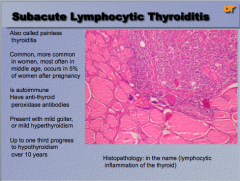
What is the condition? Another name for it?
Who is it more common in (men or women)? Pregnancy?
Is it autoimmune? What is the antibody?
Will you see a goiter or mild hyperthyroidism?
How many progress to hypothyroidism?
|
|
|
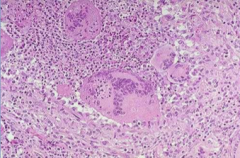
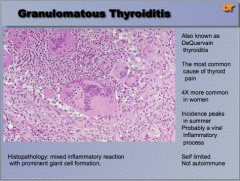
What is the condition? Another name? Most common cause of what? Men or women? What time of year? Why? Is it autoimmune? |
|
|
Disease on the left and the disease on the right? What is the general term for both? |
|
|
|
What is a chronic enlargement of the thyroid gland, not due to a neoplasm, occurring endemically in certain locations, especially regions where glaciation occurred and the soil is low in iodine, and sporadically elsewhere. |
Goiter |
|
|
What are the four types of goiter? |
1. Diffuse/nontoxic/simple/colloid 2. Endemic 3. Sporadic 4. Multinodular
Spectrum of diseases with considerable overlap, of multiple different etiologies |
|
|
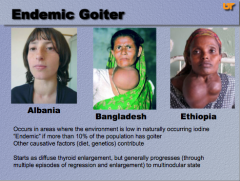
Three areas where endemic goiters occur? What does endemic mean? Two other causative factors? What does it start as but generally progresses to? |
|
|
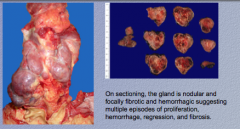
What is shown on the left? |
Large thyroid nearly encasing the trachea |
|
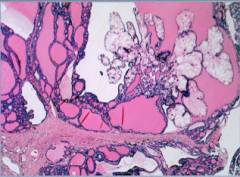
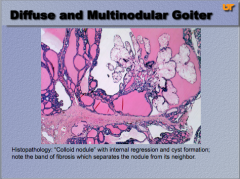
What is shown here? What is the name for the nodule with internal regression and cyst formation? What do the band of fibrosis separate? |
|
|
|
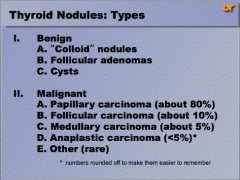
What are the three types of benign thyroid nodules?
What are the four types of malignant thyroid nodules (in order of occurrence)? |
|
|
|
Benign neoplasms outnumber thyroid carcinomas by a ratio of nearly ________ to 1.
How many new cases of solitary thyroid nodules are malignant?
Are most indolent or aggressive? |
|
|
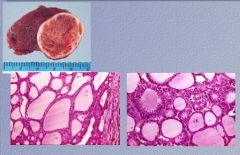
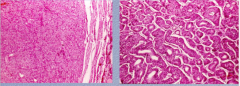
What is shown here? How can you tell? What does it produce? |
Left = follicular adenoma = solid, well circumscribed (looks like benign lesion), lack of capsular and vascular invasion must be confirmed microscopically to ensure it is benign
Follicular adenomas produce colloide to some extent |
|
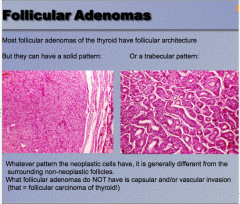
What are the two patterns of follicular adenoma?
How can you distinguish neoplastic cells from non-neoplastic?
Do follicular adenomas have capsular and/or vascular invasion? |
|
|
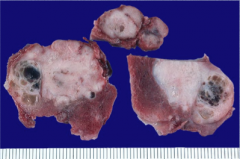
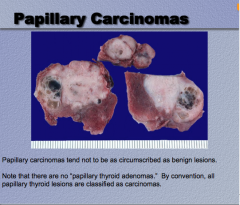
What is this? Are they circumscribed or not? |
|
|
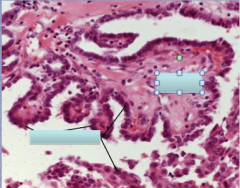
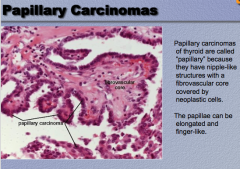
What is shown here? Why are they called this? What are the structures surrounded by? |
|
|
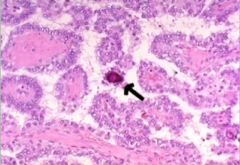
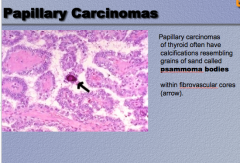
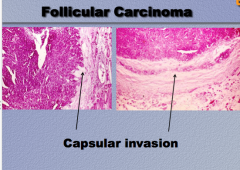
What is the tissue? What is the disease? What is the arrow pointing to? Describe it. |
|
|
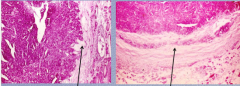
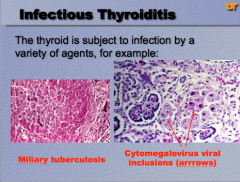
What is the disease? What are the arrows pointing to? |
|
|
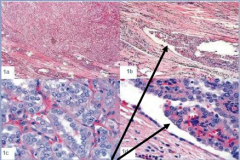
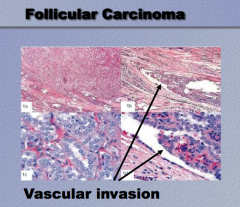
What is the disease? What are the arrows pointing to? |
|
|
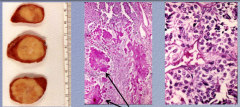
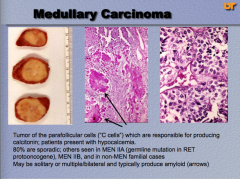
Organ? Location? What are the arrows pointing to? What is the disease?
What is the germ line mutation? What do they produce? |
|
|
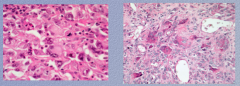
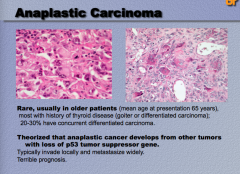
What is the organ? What is the disease? What ages? History of what? What is the theory of the pathogenesis? Prognosis good or bad? |
|
|

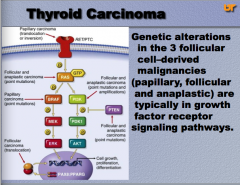
Identify where each thyroid cancer acts in the pathway. |
|
|
|
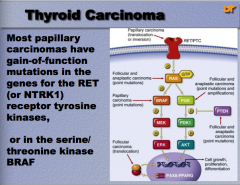
What o most papillary carcinomas have in terms of mutations? (two possible) |
|
|
|
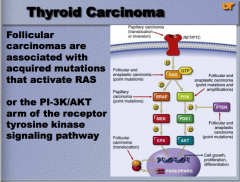
What are follicular carcinomas associate with acquired mutations of? (two things) |
|
|
|
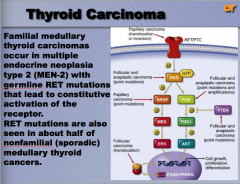
What is the common mutations for familial medullary thyroid carcinomas?
What is part of this mutations also seen in? |
|
|
|
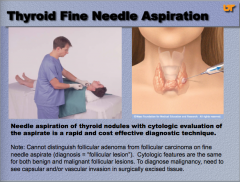
Can you distinguish follicular adenoma from follicular carcinoma on fine needle aspirate? What do you need to do to diagnose malignancy? |
|
|
|
1. Solitary nodules are more likely to be _________ than _________. 2. Nodules in younger patient are more likely to be ___________. 3. Nodules in male are more likely to be __________. 4. Nodules that are functional (that take up radioactive iodine on radionuclide imaging) [hot nodules] are almost always __________. 5. 10% of nodules that are "cold" on radionuclide imaging are ___________. |
|
|
|
Where may ectopic thyroid be present? |
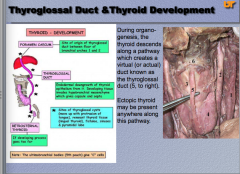
Anywhere along thyroglossal duct |
|
|
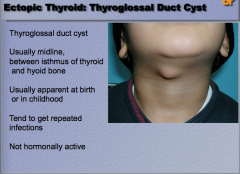
Where is a thyroglossal duct cyst usually located?
When is it usually apparent? What is it susceptible to?
Is it hormonally active? |
|
|
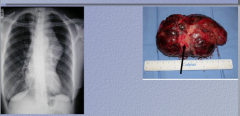
What is shown here? What symptoms did she likely have? What did she have a history of?
|
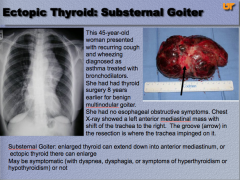
|
|
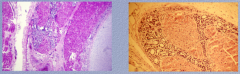
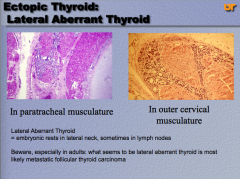
Where is the ectopic thyroid on the left? Right?
Two other locations of lateral aberrant thyroid?
What could it likely be in adults? |
|
|
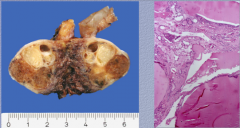
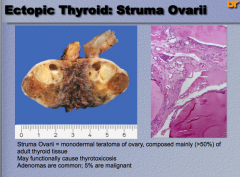
Where is this ectopic thyroid located? What is it mainly composed of?
What may it functionally cause? What is common (what percent are malignant)? |
|