![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
75 Cards in this Set
- Front
- Back
|
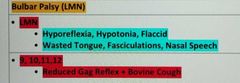
Bulbar palsy |
|
|
|
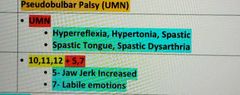
Pseudobulbar palsy |
|
|
|
SCD aplastic crises |
Low Hb Low reticulocyte |
|
|
SCD sequestration crises |
Low Hb high reticulocyte |
|
|
Gout Rx |
Acute attack: First line- NSAIDs (e.g. Ibuprofen, Naproxen) Second line- Colchicine
For long-term Xanthine Oxidase Inhibitors (after 2 weeks of acute attack) First line - Allopurinol "with NSAIDs and Colchicine coverage" Second line - Febuxostat- |
|
|
Relative risk of ectopic pregnancy in MIRENA use |
1:20 |
|
|
Contraception in breast cancer |
Only IUD / Uterine artery ablation (UAA) If menorrhagia UAA |
|
|
Post contraceptive bleeding rx |
• <3 months- Reassure Vaginal Spotting in Depo-Provera/Mirena (Oligomenorrhoea f/b Amenorrhoea) • >3 months/Problematic Bleed- COCP for 3 months WHILE ON Depo-Provera or Tranexamic acid/Mefenamic acid for 5 days • Vaginal spotting in COCP • >3 months- Switch to another contraceptive method |
|
|
Missed pill POP |
Traditional POP- >3 hours Desogestrel (Cerazette)- >12 hours late Action Plan • Take last pill ASAP even if it means taking two pills • Continue rest of pack as usual • Abstain from UPSI for next 48 hours • Emergency Contraception if UPS after missed pills or in last 48 hours |
|
|
Missed pill cocp |
1 Pill missed: 1. Take last pill ASAP even if it means taking two pills 2. Continue rest of pack as usual 3. No additional contraceptives required
2 or more Pills missed: • 1 and 2 + Abstain from UPSI until pills taken for 7 days in a row • Then look for what pills missed • if Week 1- Consider Emergency Contraception if UPSI in 1st week or Pill-free interval |
|
|
Ectopic management |
• Stable- Check beta-hCG • b-hCG<1400- Wait and observe (unlikely ectopic pregnancy). The foetus may be so small to be observed by USG • b-hCG>1400- Proceed to Laparoscopy (confirmed ectopic pregnancy) • hG is not that high>Repeat after 48 hours first (Patient Stable) (Might be Tubal Miscarriage with falling hG) • Unstable- Urgent Laparotomy (Open Salpingectomy or Salpingostomy) |
|
|
Ectopic rx |
Medical Mx- Methotrexate • Hemodynamically stable • No significant pain Adnexal mass <35mm with no foetal heart visible • Serum hCG<5000 IU/Itr (ideally <1500/Itr) Surgical Mx • Hemodynamicall unstable (Laparotomy) • Significant pain • Ruptured ectopic • Cannot come for follow up • Visible heartbeat |
|
|
AFLP |
ELLP (without Haemolysis) + Decreased Glucose +/- Increased Ammonia • Dx- Liver Biopsy |
|
|
Stress incontinence Rx drug |
Duloxetine |
|
|
Urge incontinence Rx drug |
Anticholinergic - oxybutynin/ tolterodine/ darifenacin Mirabegron if anticholinergic contraindicated |
|
|
CTG normal and pathological |
Normal CTG: • Baseline (bpm)- 110-160 • Variability (bpm) - 5-25 • Decelerations (bpm)- None or early
Pathological: Acute Bradycardia/ Single prolonged deceleration >3 minutes > Urgent Intervention and Expedite delivery |
|
|
When to conceive after Gestational trophoblastic disease |
Not until 12 months after completing Rx (chemotherapy)
Not until 6 months after betaHCG counts are normal + barrier contraception 2 weekly screening of urine and serum HCG till normal. |
|
|
Somatization disorder |
So many symptoms and tests without any physical cause Patient refuses to believe negative test results |
|
|
Conversion / dissociative disorder |
Loss of motor or sensory functions without any organic cause Occurs after an event Patient doesn't feign it. It's out of their control |
|
|
Ganser syndrome |
Gangster / prison psychosis Prisoner fakes symptoms for gain |
|
|
Cotard delusion |
Already dead |
|
|
Capgras delusion |
Replaced by an imposter |
|
|
Fregoli delusion |
Multiple people are actually the same person in disguise |
|
|
Psychoactive drug |
LSD |
|
|
TCA OD Rx |
IV NaCl (0.9%) + HCO3 (50-100mL of 8.4%) |
|
|
OPP poisoning rx |
Pralidoxime |
|
|
Fine tremors caused by which drug |
Sodium valproate |
|
|
Pregnant and Still taking Lithium |
Check plasma lithium levels Monthly till 36 weeks of pregnancy & Weekly till birth |
|
|
Drugs not used with Lithium |
NSAIDs(especially Ibuprofen) Aspirin Diuretics SSRI |
|
|
Tardive dyskinesia Rx |
Give depot injection of atypical antipsychotics ( risperidone/ olanzapine) NOT ORAL |
|
|
Cervicitis Rx |
Chlamydia Doxycycline 100mg BD 7 DAYS Or azithromycin 1G P/O fb 500mg for 2 days
Gonorrhea Ceftriaxone 1gm IM single dose Or Ciprofloxacin 500 p/o single dose |
|
|
PID RX |
Opd Ofloxacin + metronidazole Inpatient CDM |
|
|
Endometrial cancer Sx Ix |
Female >51 With post menopausal bleeding Ix Transvaginal ultrasound If endometrial thickness > 4 mm do hysteroscopy with endometrial biopsy (definitive) Progesterone reduces the risk of endometrial cancer |
|
|
Early amenorrhea and premature ovarian failure |
Premature ovarian failure <40 year old Early menopause 40-50 year old |
|
|
Ectopic investigation |
Initial - urine pregnancy test If positive - transvaginal ultrasound If ultrasound shows empty uterus - beta HCG (If stable) (1400) Emergency laparotomy (if unstable) If HCG is not that high repeat after 48 hours could be tubal miscarriage |
|
|
Miscarriage Vs still birth |
Miscarriage before 24 weeks Still birth after 24 weeks |
|
|
Hyperemesis gravidarum rx |
FAST fluids Antiemetic Steroids Thiamine |
|
|
Initial Ix in placenta previa and abruption |
Abruption - CTG previa - TVUS |
|
|
Hypertension terms in pregnancy |
Chronic htn - before 20 wk Gestational htn - new htn after 20 wks without significant proteinuria Preeclampsia - new htn after 20 wks with proteinuria -24 hour urine protein >_0.3g -pcr >_30mg -acr >_ 8mg
Severe preeclampsia - Bp > 160/110 Or preeclampsia with recurring severe headaches, scotoma, epigastric pain with bad labs.
HELLP Eclampsia |
|
|
Pregnancy htn and asthma rx |
No labetalol Give CCB Nifedipine |
|
|
Colorectal Cancer Screening: |
V Fecal Immunochemical Test (FIT). V 60-74 YO every 2 years. |
|
|
Breast cancer screening |
(Mammogram). 50-70 YO every 3 years. Those with high risk > 40-70 YO annually. |
|
|
Breast cancer screening |
(Mammogram). 50-70 YO every 3 years. Those with high risk > 40-70 YO annually. |
|
|
Cervical (Cervix) Cancer Screening: |
(Pap smear - Cervical smear: Cytology, HPV) 25-49 YO - every 3 years. 50-64 - every 5 years. |
|
|
Pregnant and still taking Lithium? |
Check levels Monthly till 36 weeks and then weekly till birth Can cause ebstein anomaly and floppy baby syndrome |
|
|
Serotonin syndrome cause |
SSRI Fluoxetine Citalopram Sertaline |
|
|
Neuroleptic malignant syndrome cause |
Metaclopramide Haloperidol Clozapine Risperidone |
|
|
Genetic disorder with chorea and cognitive impairment |
Huntington's Autosomal dominant Jerky involuntary movement |
|
|
Akathisia cause |
Fidgeting, inability to sit still Due to long term use of antipsychotics (risperidone) |
|
|
ADHD Rx |
Children Methylphenidate (first line) ADHD-focused group parent-training programme Adults Lisdexamfetamine or Methylphenidate first line in adults СВТ
With Insomnia? • First line- Sleep hygiene • Second line- Melatonin |
|
|
GAD first line Rx |
Sertaline |
|
|
Pneumonia consolidation |
Staph causes Cavitation • Klebsiella- Cavitation Upper Lobes • Strep causes Lobar Consolidation • Mycoplasma causes Patchy Consolidation • Legionella- Bi-Basal Consolidation |
|
|
Aspiration pneumonia rx |
Amoxicillin + metronidazole |
|
|
Legionella pneumonia rx |
Macrolides |
|
|
Pneumothorax rx |
Unstable- 02>Needle decompression>ID Stable- CXR
Primary • < 2cm - Conservative (02) • >2cm (or distressed)- Aspirate with Needle • (Aspirate with Needle is different than Needle decompression)
Secondary • <1cm- Conservative • 1-2cm- Aspirate with Needle • >2cm- ICD |
|
|
Carbon monoxide poisoning rx |
Conscious • 100% 02 via tight-fitting mask with an 02 reservoir Unconscious + Hypotensive (SBP<100) • Intubate and Ventilate with IPPV Soot in Mouth- Intubate |
|
|
Flail chest Rx |
Mx • Stable + Normal Sp02 = Analgesia (e.g. intercostal block) • Unstable = ABC > Analgesia (High flow 02 then Analgesia) • Drowsy, Laboured breathing, Worsening RR = Intubate (usually with double lumen endotracheal tube) |
|
|
Atelectasis |
Post op complication within 72 hours |
|
|
Asthma exacerbation management in adults |
Oxygen - salbutamol - steroids If life threatening Salbutamol back to back. Add ipratropium bromide Mgso4 |
|
|
Asthma exacerbation in children rx |
Oxygen - salbutamol - ipratropium - steroids (oral then IV)
If life threatening not improving
IV salbutamol/ IV Aminophylline / IV Mgso4 |
|
|
Tumor lysis syndrome ix |
Serum urate (uric acid only) |
|
|
Smudge cells in |
Cll |
|
|
Aeur rods in which leukemia |
Aml |
|
|
Hodgkin and non Hodgkin age groups |
Hodgkin bimodal Less than 25 and greater than 55 Non Hodgkin 25-40 |
|
|
Atresia |
No Gastric Bubbles- Oesophageal Atresia Single Bubble- Gastric/ Pyloric Atresia Double Bubble (Double bubble sign: esophagus + Stomach)- Duodenal Atresia OR Malrotation and Volvulus Triple Bubble Sign- Jejunal Atresia |
|
|
Pylori. Stenosis acid base |
Metabolic alkalosis hypokalaemia hypocholeremic |
|
|
Malrotation and Volvulus |
• Bilious vomit + Blood in Stool • Ix-Xray- Double Bubble Sign, Barium Enema • Rx- ABCDE>NGT>S |
|
|
Pyloric stenosis |
• Projectile Non-Bilious Vomit + Want to feed + Metabolic Alkalosis (Hypokalemia + Hypochloraemia) + Almond size mass
• Ix- First SE, Then- USG (Pylorus thickening)
• Rx- Electrolve correction>NGT>Ramsted Pylorotomy |
|
|
Pyloric stenosis |
• Projectile Non-Bilious Vomit + Want to feed + Metabolic Alkalosis (Hypokalemia + Hypochloraemia) + Almond size mass
• Ix- First SE, Then- USG (Pylorus thickening)
• Rx- Electrolve correction>NGT>Ramsted Pylorotomy |
|
|
Intussusception |
• Paroxysmal Colicky pain + Child crying + Sausage shaped mass + Red Currant Jelly/Blood stained stool
• Ix- USG- Target Doughnut sign
• Rx- Air/Barium Enema Insufflation> Sx |
|
|
Meckels diverticulum |
• Painless bleed + Rule of 2- 2 year, 2 inch, 2cm away from ileocecal valve
• Ix- Radioisotope scan>Laparotomy
• Rx- Sx |
|
|
Cystic Fibrosis |
• Gene- 7 CFTR • Echogenic bowel on US+ Meconium Ileus + Bilious Vomit |
|
|
Necrotising enterocolitis |
• ABCD in a Premature Baby= Air in bowel wall + Bloody stools + Cannot tolerate feeds + Distension in Premature Baby + Vomiting +Hypoactive
• Ix- X-Ray Abdomen
• Rx Air in bowel/ Distended loops- Stop feed + IV Fluids + Systemic Abs
• Pneumoperitoneum- Emergency Laparotomy |
|
|
GERD |
• Does not want to feed + Non-Proiectile Bilious vomit • Rx- Reduce amount but increase frequency> Gaviscon> PPI H2 blocker |
|
|
Nephrotic syndrome features |
Nephrotic Syndrome- Triad of- Proteinuria (>3g/24hr- Frothy Urine), Hypoalbuminemia (<30g/L), Oedema; |