![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
286 Cards in this Set
- Front
- Back
|
Verschuren et al. |
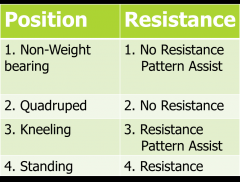
Resistance training is disputed for kids w/ CP • 4 RCT's. All 4 meet guidelines for frequency (2-3). 2 met NSCA guidelines for intensity. None met guidelines for duration (8-20 weeks is guidelines; these were 5-12 weeks) |
|
|
article take home message |
RECOMMENDATIONS FOR CHILDREN W/ CP = RECOMMENDATIONS FOR ALL.Will have a reduce capability so the form of exercise may be different but with same time, intensity and days |
|
|
resistive exercise |
any training that uses a resistance to the force of muscular contraction. Needs to be task specific for children; they do not transfer skills very well due to motor learning |
|
|
modes of RT |
Weight training. Resistive bands/tubing. Hydrotherapy. Functional exercises. Isometrics.Plyometrics |
|
|
RT benefits |
Improve sports performance. Prevents injury- trains neuromuscular system to increase response, trains mm to increase BF and force. Rehab. Enhances general health- cardiovascular fitness, body comp, bone density, blood lipid profiles, mental health. Children will not hypertrophy until they have androgens |
|
|
RT kids pops |
All abilities. 7-18 years old. Pre vs post puberty guidelines and expected outcomes are different. Train more like adults post puberty |
|
|
AAP med eval for |
hypertension, chemo w/ anthracyclines, cardiomyopathy, moderate to severe pulmonary hypertension, Marfan syndrome (affects all CT, weak), seizure disorder |
|
|
AAP safety |
Avoid power lifting, body building, and maximal lifts until done growing- Injury to the growth plates; break off a piece. Educated about health risks of using performance enhancing drugs. Resistive tubing and free weights more appropriate than weight machines |
|
|
AAP pre req |
Address all major muscle groups, no isolation. Stop w/ any sign of illness or injury; evaluated fully. Instructors should have certification. Proper technique and strict supervision are critical |
|
|
AAP intensity |
Use low resistance until proper technique is perfected. Increase load in 10% increments after 8-15 repetitions can be performed |
|
|
AAP duration/frequency |
20-30 min. 5-10 minute warm up and cool down. 2-3x/w on non-consecutive days. Couple w/ aerobic conditioning if general health benefits are the goal. 8 to 10 weeks |
|
|
NSCA general guidelines |
instruction/supervision. env safe. 5-10m warm-up. Begin light loads, focus on correct technique. 1-3 sets of 6-15 reps, variety of UE/ LE exercises. rest 1m b/s sets. increase 5-10%/w as strength does. cool w/ calisthetics & stretch. Perceived exertion. 2-3x/w w/ rest day. Use workout logs, vary program. nutrition, hydration, sleep. Edu parents on proper support |
|
|
perceived training |
Appropriate for 10 and up. HR for others, physical cues- red face, sweaty, fatigue |
|
|
NCSA vs AAP |
rest period 1m b/n sets. More than 1 set. Use perceived exertion |
|
|
NCSA power training |
(not max lifts, low weights, more about motor learning and not hypertrophy) 1-3 sets ○ 3-6 reps |
|
|
NCSA strength training |
(start w/ this and move to power training)1-3 sets6-15 reps |
|
|
mechanisms of improvement in strength for kids |
1. Increased neuronal control (neuromuscular learning); most of changes. Increased firing rate, # neurons firing, improved motor unit recruitment & coordination. 2.Intrinsic m adaptation. hypertrophy small 3.Maturation change; does exercise or growth increase strength. 24h change. M & F respond similarly to RTF stronger earlier on due to earlier puberty |
|
|
how should kids do RT |
benefit the most from practicing and perfecting motor skills. RT can improve m performance and coordination of m groups. Training adaptations are specific to: mov't pattern and speed, the contraction type and forc. |
|
|
blocked periodization |
to continue to adapt we need variability, increase weight, frequency, sets, time. A block is usually several weeks; needs to change after a few and throughout the yea. Individualization, rate of change in body, specificity, intensity, regularity |
|
|
Expected motor improvements w/ RT |
Mod effect on running speed (.53 effect size) Mod effect on jumping distance or height (.54) Large effect on throwing distance & speed (.99) Small effect on improving strength (.38) |
|
|
motor learning principles w/ children |
Short, precise, verbal cues. Children require more feedback. longer periods of practice. Thousands of reps Ex. need to walk 13m before able to walk by themselves. Feedback should be gradually reduced. Ask to reflect on their performance better than adjusting their body position, demo, or lengthy explanations. |
|
|
implementing a RT program |
establish a goal. choose a type of RT. plan training program. monitor progress and outcomes |
|
|
choose a type of RT |
Specific to the mov't pattern and mov't speed. The contraction type and force. The secondary impairments, limitations, and restrictions of the child |
|
|
plan the training program
|
Frequency. Duration. Intensity (amount of resistance) and volume. Rest intervals. Choice and order of exercises. Method of increasing exercise load. Warm-up and cool-down. Program variation. Safety |
|
|
monitor progress and outcomes |
Develop a workout log. Define expected outcomes. Measurement of expected outcomes and goal. Body structure/function
|
|
|
PT role in infection management |
Inspect before/after exercise. Redness, tissue necrosis Palpate for tenderness and edema. Note signs of drainage. Check mobility as it heals. Education on wound care |
|
|
maximum protect phase |
Decrease inflammation and pain, protect tissue, education, start ROM if allowed (PROM, AAROM, or AROM). Mm setting to prevent atrophy, relaxation, TENS. Ranges from a few days to 6 weeks |
|
|
moderate protection phase |
No pain at rest and some no/low pain ROM. Restore ROM and arthrokinematics, improve neuromuscular control and stability, gradually increase strength. Begins at 4-6 weeks and lasts 4-6 weeks |
|
|
minimum protect/return to function phase |
Full or almost full pain free ROM w/ a stable capsule if involved. Restore functional strength and increase functional activities. Begins 6-12 weeks and last 6m and up to a year |
|
|
DVT risks
|
Total knee/hip, Post op/fx immobilization, Bed rest, Sedentary life/sitting during long travel, Trauma to venous vessels, Limb paralysis, Active malignancy past 6m, Hx of it, Advanced age, Obesity, CHF, oral contraceptives, Pregnancy |
|
|
ways to reduce DVT |
Anticoagulants, Elevating legs, No prolonged sitting, Ambulate ASAP, Pumping exercises, Compression stockings, Sequential compression units |
|
|
open sx |
Deep cut so operation field is fully visible Extensive disturbance of soft tissues. Through skin, fascia, mm, and joint capsule. Lengthy rehab and healing |
|
|
arthroscopic sx |
Outpatient more often. Several small incisions in skin, mm, and joint capsule for insertion of camera and tools. Minimal disturbance of soft tissues.Rehab quicker |
|
|
why repair a tendon quick |
Otherwise the tendon will retract making the procedure harder to do. Within a few days |
|
|
cemented |
uses an acrylic based cement, tends to break down, causes loosening and pain. Used in older, sedentary patients |
|
|
uncemented |
Less likely to loosen. Younger and more active get it. Biological fixation- microscopic ingrowth of bone into porous coated prosthetic surface. Macrointerlock- b/n a nonporous component and bone w/ a bioactive compound applied to the component to improve osseous integration. Press fit- tight fit b/n bone and implant. Screws, bolts, nails |
|
|
hybrid |
noncemented component of one joint surface and a cemented component on the other |
|
|
arthrodesis |
fusion of joint; keep function w/ reducing pain |
|
|
osteotomy |
cutting and realigning of bone; done with arthritis, improperly formed hip |
|
|
open reduction internal fixation ORIF |
fx came out of skin, use a wire, plate, screw to hold the fx together |
|
|
epicondylitis |
Discontinue aggravating activity. Isometric. Concentric. Eccentric |
|
|
lateral epicondylitis
|
Isometrics: start in more elbow flex and then do isometrics. Some pain good (3/4 out of 10). As it gets better more elbow ext and wrist flexion Concentric: bend elbow and ext wrist Eccentric: slowly move elbow ext & wrist flexion Add weight. Return to function depends on activity. Many in manual labor |
|
|
medial epicondylitis
|
Isometrics: start in more elbow ext and then do isometrics. As it gets better more elbow flex and wrist ext Concentric: elbow ext and wrist flex Eccentric: slowly move into elbow flex and wrist ext. Return to function depends on activity |
|
|
D1 flexion
|
GH flex, add, ER Elbow flex Supination Wrist flex, radial deviation Finger flexion |
|
|
D2 flexion
|
GH flex, abd, ER Elbow ext Supination Wrist ext and RD Finger ext |
|
|
stress urinary incontenence |
Involuntary leakage of urine on effort or exertion, or on sneezing or coughing. Correlated with parity (# of children had), age, overweight. Exercise- Improve support of bladder and urethra. Improve closure of urethra. well accepted evidence for, but how many, position, hold? |
|
|
Urge urinary incontinence |
Involuntary leakage accompanied by or immediately preceded by urgency |
|
|
overactive bladder |
Urinary urgency, with or without urinary incontinence, usually accompanied by frequency =/> than 8/day, and nocturia |
|
|
Post-prostatectomy incontinence |
Incontinence occurring after prostate surgery, likely caused by bladder dysfunction or urethral sphincter dysfunction due to muscle or nerve injury. |
|
|
Fecal incontinence |
Involuntary passage of feces |
|
|
pelvic organ prolapse |
Abnormal descent of pelvic organs (uterine prolapse, cystocele, rectocele) |
|
|
Peripartum low back and pelvic girdle pain |
Pain in the low back or pelvic girdle occurring during or after pregnancy |
|
|
high risk pregnancy |
Pregnancy in which the mother, fetus, or newborn is at risk of increased morbidity or mortality before, during, or after pregnancy. |
|
|
Diastasis recti abdominus |
Separation of the two sides of the rectus abdominus at the linea alba with a widening of the linea alba greater than 2 cm |
|
|
Peripartum incontinence |
Urinary incontinence during or after pregnancy |
|
|
Cesarean birth |
Surgical delivery of baby through wall of uterus instead of through vagina |
|
|
Pelvic pain syndromes |
Pain in the pelvic floor musculature or surrounding structures; may be associated with a variety of diagnoses. |
|
|
superficial pelvic layer |
Urogenital triangle. Superficial transverse perineal m. Bulbo- and ischiocavernosus mm. External anal sphincter. Actions: support, sexual, sphincteric |
|
|
middle layer of pelvic layer- urogenital diaphragm |
Compressor urethrae, urethrovag sphincter, deep transverse perineal. Innervation: Dorsal n. of penis/clitoris (branch of pudendal, S2-4). Function: Sphincteric (close urethra). |
|
|
deep layer- pelvic diaphragm |
Levator ani- Puborectalis. Pubococcygeus. Iliococcygeus. Coccygeus (moves tail side to side) Function: support (biggest area to work on), sexual |
|
|
accessory mm of pelvic floor |
piriformis and obturator internus. Relevance: Proximity- hip and pelvic floor issues are largely related. Innervation levels. Interplay between hip, l/s, pelvic floor. |
|
|
causes of SUI
|
Urethral hypermobility- females move more ant/post, less passive tissue resistance due to shorter urethra. Weak muscles- vaginal birth. Chronic coughing/straining. Decreased estrogen- menopause, affects urethral tissue. |
|
|
PERFECT model
|
Exercise prescription based on patient’s strength and endurance P = power (MMT) E = endurance in seconds (type 1); do these first R = repetitions of endurance hold (type 1) F = fast contractions (type 2 fibers) PERFECT score of 3/6/5/10 |
|
|
Kari bo approach |
SUI. Based on exercise physiology and principles of strength and conditioning. 8-12 reps of 6-8 sec holds, multiple positions, followed by 3-4 maximum quick contractions, 3x/week. less individualized, doesn't help if really weak |
|
|
PERFECT rationale |
Levator ani are 70% type I and 30% type II. E and R components of PERFECT address type I.F component addresses type II. |
|
|
pros and cons perfect and kari bo |
PERFECT Pro: Individualized Con: Does not follow standardized principles of strengthening programs Bo Pro: follows established strengthening principles Con: not as individualized |
|
|
perfect vs kari bo |
No direct comparisons. Recommendations for ex prescription- Consider fiber type, Overload (cones vs increasing sets and reps and decreasing rest time), Position, Neural adaptation vs hypertrophy,Co-contraction of transversus abdominus? It requires hypertrophy!! |
|
|
TA and incontinence |
PFM contractions and TrA contractions normally occur together, many w/ incontinence lose this ability. Research: Unclear whether adding TrA to training program improves outcome. May help if cannot get a contraction |
|
|
causes of OAB and UUI |
Diet, bad bladder habits, genetics |
|
|
treatment for UUI and OAB |
Behavioral modification. Exercise. Behavior modification- Avoid “just in case voiding.” Establish normal voiding interval- q 2-4 hours during the day, 0-1x/night. Recognize contributing dietary factors (OAB)- Caffeine. Artificial sweeteners.Acidic foods and beverages. |
|
|
exercises for UUI and OAB
|
Quick pelvic floor m. contractions- Cause reflex inhibition of detrusor decreasing feelings of urgency. Practice: deep breath, relax, contractions. Endurance exercise prn. E stim- Setting causes reflex inhibition of detrusor. |
|
|
post prostatectomy UI |
Caused by surgery for prostate cancer. 8-56% of men treated have UI 1 year post. Recommendations from research: Ensure correct contraction, Use estim prn |
|
|
bowel function |
Normal function: 1. Stool enters descending colon. Contracted PR (puborectalis) “kinks” colon; EAS and IAS both active a no voiding 2. When ready, PR, EAS, and IAS all relax and voiding occurs Probs: 1. No “unkinking” = constipation 2. Inadequate contraction of any m. = incontinence of feces or gas |
|
|
fecal incontinence
|
Neural considerations- EAS is voluntary. Inferior anal n. S2-4, can rehab. IAS is involuntary. Pelvic splanchnic nn. S2-4. Tear during childbirth- grade 4 through IAS, incontinent for a while, cannot rehab, build up other mm
|
|
|
Cystocele and urethrocele |
anterior defect. Bladder or urethra bulges into vagina |
|
|
rectocele |
posterior defect. Rectum bulges into vagina |
|
|
uterine prolapse |
uterus drops down into vagina. more common w/ a straighter uterus |
|
|
Pelvic floor mm strengthening for prolapse
|
PT avoid to sx. Exercise beneficial even if sx chosen. Avoid Valsalva – extra important! Gravity-assisted PFM exs- if bad; elevate pelvis in supine. Evidence: 1:1 PT decreases POP s/s (NNT of 3). Changes sustained 2 years later |
|
|
biofeedback for prolapse |
Types: Intravaginal (or rectal) sensor. Ultrasound imaging. Tactile feedback. Useful for people with difficulty learning how to contract PFMs. |
|
|
vaginal weights for prolapse |
Weighted device placed in vagina above levator ani. Promote endurance training.Progress by increasing activity level (walking vs exercise), weight, duration of use. Not used as much- functional? |
|
|
estim for prolapse
|
Indicated: very limited PFM contraction ability. Similar parameters and contraindications as estim for other mm, + contraindicated with active infection, pregnancy. For women and men. Also used for urinary urgency. |
|
|
posture changes due to forward shift of center of gravity due to prego
|
Forward head. Rounded shoulders. Increased lumbar lordosis. Changes frequently lead to pain- Prevalence of LBP in pregnancy is 47-82% (Kalus, Wang) |
|
|
posture exercises for prego
|
Neck strengthening/stretching. Mid trapezius/rhomboid strengthening. Pectoralis stretching. Low back stretch. Special attention to avoiding LOB. Encourage maintenance in post-partum period. |
|
|
Causes of peripartum LBP |
Altered load due to weight gain, Change in COG, Decreased ligamentous stability due to hormonal changes. Do stabilization exercises work? |
|
|
research on postpartum LBP
|
Exercise with emphasis on global musculature not helpful (Mens ’00). Emphasis on local mm. followed by exercise for global mm. decreased pain (Stuge ’04) |
|
|
aerobic exercise guidelines during prego |
Healthy pregnant and postpartum women:150 m/w moderate intensity. 20-30 m/d most/all days. Okay to continue “vigorous” exercise, provided health is maintained. Upper limit not established; use pre-pregnancy activities as guideline |
|
|
aerobic exercise effects on fetus |
Exercise in early and mid pregnancy stimulates placental growth (Clapp 2006). Continuing to run during pregnancy increases placental volume |
|
|
aerobic exercise safety and prego |
Safe and healthy to continue pre-preg exercise level, even very intense exercise, unless joint pain or incontinence develops. Safe to start low-level exercise program even if inactive before. Start slowly; monitor closely. HR moitoring not good- to variable, RPE 13-14 on Borg 6-20 scale |
|
|
aerobic exercise and effects on the woman |
improved long-term fitness into perimenopausal period. Decreased gestational diabetes risk. Decreased rate of C section. Improved fitness; smaller babies (maybe). Decreased postpartum recovery time |
|
|
excessive weight gain and prego |
Excessive gain correlated w/ HTN, post-partum overweight, delivery complications (C-section), overweight babies. Only need 300 cal/day extra. Guidelines for weight gain:28-40# if underweight 25-35# if normal weight 15-25# if overweight 11-20# if obese |
|
|
pyshiological and morpholigal changes in prgo |
Resting HR ↑ Stroke volume and blood volume ↑ Change in COG Change in weight |
|
|
relative contraindications for aerobic exercise during prego |
Anemia. Cardiac arrhythmia. Chronic bronchitis. Poorly controlled type 1 diabetes. Extreme obesity or extreme underweight. Hx of extremely sedentary lifestyle. Intrauterine growth restriction. Poorly controlled HTN. Orthopedic limitations. Poorly controlled seizure or thyroid dz. Heavy smoker |
|
|
absoulte contraindications to aerobic exercise in prego |
Severe heart or lung dz. Incompetent cervix or cerclage. Pre-term labor. Multiple gestation at risk for pre-term labor. Persistent 2nd or 3rd trimester bleeding. Placenta previa after 26w. Premature rupture of membranes. Prego induced HTN or pre-eclampsia. Severe anemia |
|
|
safe exercise for prego woman |
Walking Swimming Stationary cycling Aerobics Yoga* Pilates Running or jogging* Strength training* *Running and strength training if done previously. Yoga: avoid hypotensive positions and dec. venous return |
|
|
exercise to avoid during prego |
Contact sports (boxing, soccer, basketball)High fall risk sports (skiing, surfing, off-road cycling, gymnastics, horses)Scuba divingSky diving“hot yoga” |
|
|
high risk pregnancy |
mother, fetus, or newborn is at risk or may be at risk of increased morbidity or mortality before, during, or after pregnancy causes: preterm labor, multiples, vaginal bleeding, placenta previa, incompetent cervix, hx of complications |
|
|
bed rest |
should not be routinely recommended- not effective prevention for preterm birth for high risk pregnancy |
|
|
guidelines for bed rest exercises |
Several exercises 2-4x/day. Position: semi-reclined, sidelying, or ¾ sidelying. Avoid increases in IAP- exhale with exertion. Examples: Backward shoulder rolls. Ankle pumps. Hip ab/adductionPNF patterns. Abdominal drawing in. Cervical ROM. Heel slides. Quadriceps and gluteal setsPF contractions. |
|
|
diastasis recti abdominus |
Separation of 2 sides of recti > 2 cm. Due to physical stress + laxity from hormones. Decreased abdominal musculature capacity leads to probs w/ posture, trunk stability and motion, urination and defecation. Exercises to correct:Approximate 2 sides of rectus w/ hands or w/ sheet, Perform slight posterior pelvic tilt and gently exhale while lifting head |
|
|
external support and prego |
Helps w/ compressed pelvic joints. Lifts abdomen. Comfortable; many women will wear it at night. While strength will not be bad the changes often happen to slow and this can help. SI pain, abdominal pain, sleep better, can continue to exercise longer |
|
|
peripartum UI |
Prevalence of UI in pregnancy: 40-50%. 34% continent during pregnancy will develop postpartum UI. Exercise during pregnancy helps prevent UI in late pregnancyExercise in early postpartum period for women with UI decreases UI at 1 year |
|
|
recommendations for exercise and peripartum UI |
Ensure correct contraction. Perform 3x8 submax contractions held 8-10s, followed by 3-4 fast contr, 2x/d throughout prego. Perform exercises in multiple positions. Influence of episiotomy on muscle recovery. Cut through, or lateral to, perineal body |
|
|
episiotomy for peripartum UI |
Immediately postpartum: No difference, doesn't prevent perineal laceration, pain levels, pain med use. Long-term: Does not prevent incontinence, reduce incidence of impaired sexual function. Pain w/ intercourse more common among women w/ episiotomy. (Hartmann 2005) |
|
|
C section |
Rate in US: Approx. 1/3 of all deliveriesRange: 3% - 70%Major abdominal surgery affects muscles of abdomen. Consider effect on lifting ability. |
|
|
categories of C section |
Elective/Planned: Less physical stress on pelvic joints and pelvic floor because not pushing.Many OR hospitals banned elective sections in 2011 Unplanned: Higher strain on pelvic floor mm. and pelvic joints, especially in certain positions |
|
|
C section exercises |
Diaphragmatic breathing and huffing. Ankle pumps. Quads and gluteal iso. Bridging w/ abdominal drawing in. Walking short distances. Pelvic floor contractions. 10 reps several times per day. Can begin day of sx. Avoid increases in IAP until uterus is healed (6-8 weeks)Lifting baby?? |
|
|
pelvic pain syndrome |
Variety of conditions affecting tissues around pelvic floor musculature- Endometriosis, Pelvic organ prolapse, Fibromyalgia, IBS, PID, PCOS, Vaginismus, vulvodynia, dyspareunia. Chronic Pelvic Pain Syndrome- Interstitial cystitis/painful bladder syndrome. Chronic prostatitis |
|
|
PT and pelvic pain syndrome |
Address musculoskeletal dysfunction associated with pathology. Does not cure pathology. Examples of musculoskeletal dysfunction:Deconditioning due to limited activity, Adaptive shortening of external and internal musculature |
|
|
pelvic pain tx |
General conditioning: Cycling and high-impact may aggravate PFMs, Walking and low-impact: better. Stretching peri-pelvic musculature. Strenghtening- Hamstrings. Hip add, flexors, rotators. Exercise for internal musculature: Stretching w/ dilators, EMG, General relaxation techniques, Strengthening prn. Multi modal tx |
|
|
PT goals and C section exercises |
Goals:Decrease effects of anesthesia. Facilitate m. recovery while protecting incision. Minimal research; recommendations are from general recommendations post-abd surgery |
|
|
EMG and pelvic pain syndrome |
pelvic floor tension myalgia may be a contributing factor to CPPS; maximum muscle contraction can promote maximal muscle relaxation. Electrodes placed on perineum, vaginally, or rectally. Max contraction followed by max relax |
|
|
exercise and sensitive NS |
Chronic pain causes central sensitization. Complex interaction of tissue injury and patient beliefs about injury. Can result in decreased inhibition of pain, and ultimately increased disability and decreased functioning. Exercises to promote sensory awareness, such as pelvic tilts and guided sensory training in various postures. Deep breathing, cardio, yoga |
|
|
function |
Those activities identified by an individual as essential to support physical, social and psychological well-being and to create a personal sense of meaningful living |
|
|
functional testing |
Assess pts ability to move through and control 3 planes of mov't. quantitative and qualitative data. Used to determine if pt. can participate in their work/sport/activity safely w/o functional limitations. Isokinetic strength does not correlate strongly w/ functional tasks. Monitor progress, ID dysfunction, progress tx, reduce re-injury risk (ACL 15x retear, 30% another reinjury 1y) |
|
|
safe functional test selection |
Tissue healing times. Do they have the strength capacity the test? proper warm up Avoid testing in fatigued state. However many injuries are happening in a fatigued state; some train in a fatigued state on balance and stability.least fatiguing/high skill test before endurance or strength testing. 5 mins rest b/n tests to restore phosphagen energy system |
|
|
ATP-PC energy source phosphagen |
20-30s. work:rest ratio = 1:12 to 1:20 for work at 90-100%1:3-1:5 for work at 75-90% |
|
|
Phosphagens and anaerobic glycolosis energy source |
30-90s. work:rest ratio 1:3 to 1:4 |
|
|
Anerobic glycolosis and aerobic metabolism energy source |
90-180s. Work:rest ratio 1:1 to 1:3 |
|
|
Oxygen (aerobic metabolism) energy source |
after 2nd min. work:rest ratio 1:1 long duration less intensity1:3 short duration higher intensity |
|
|
selecting a functional test |
safety, relevant to them, specificity to their sport and injury hx, validity, accuracy, practicality |
|
|
criteria for functional testing |
at least 75% of the uninvolved side strength. ROM w/in 10% of uninvolved side. Pain <3/10 on VAS. Rules for how you test: Be consistent on how you test for the same client. Avoid unwanted compensation. Allow 3 practice tests but remember that practice makes perfect- no practice at home |
|
|
trunk functional mov'ts |
prone bridge ( Female 51.2 +19.9 Male 92.9 +29.3), side bridge (L 85 +36 R 81+36), back extensor enurance test (113.86s +/- 45.59s). |
|
|
LE functional tests |
single leg squat, star excursion balance test, single leg hop, t test. |
|
|
single leg squat |
assess strength, balance and neuromuscular control on single leg. No stats on the test and somewhat subjective. Have pt stand on 1 leg w/o shoes and hands on hips- Instructed to squat down as far as possible bending at the hip knee and ankle. Watch for compensation in frontal plane and sagittal plane |
|
|
star test |
Used to determine balance and postural control. Pt is asked to reach as far as possible in 8 different directions at 45 degree increments while maintaining balance on fixed stance foot. Most research ant, med-ant, med, med-post. >4cm R/L diff 2.5x more likely LE injury. chronic ankle instability- sig shorter diff in |
|
|
single leg hop |
assess knee function. side to side comparison. Progression. any LE injury rehab for progressing. in conjunction w/ other tests (figure 8, up down test, side hop). Ensure proper warm up/education and trial sessions (25%, 50%, 75% efforts) Jump as far, hold 2s, mark heel. high correlation to knee extensor torque. <88% at 6m ACLR less success long term |
|
|
t test |
Pt sprints 10 yd forward touches R hand to base of cone. Side shuffle L 5 yd and touch base of cone w/ L hand. Side shuffle R 10 yd and touch base of cone w/ R hand. Side shuffle L 5 yd and touch base of cone w/ L hand. Backpedal 10 yd. Do 2x, take best time Rest 1-2 min b/n trials Stats Tests speed, agility and postural control in all planes of movement |
|
|
UE functional tests |
modified pull up, single arm shot put, shot put CKCU Test, functional throwing performance index, softball throw for distance |
|
|
modified pull up |
Get arms parallel to floor- do not need to get chin to it Max reps or # in 15s. Best predictor of performance for softball throw for distanc. Normatives but need more data. men 9-17 female 4-9 |
|
|
single arm shot put |
Tests power and strength of upper extremity Patients sits in chair with legs out straight Patient ‘puts’ a 2.72kg shot put with dominant hand25%, 50%, 75%, 100% effort. high reliability. normative data |
|
|
shot put |
Patients seated against wall with knees at 90 degrees Throws a 10# shot put with both hands from the chest Reliability improves with controlling angle of release. Gillespie and Keenum 1987 Reliability r=.95. Johnson and Nelson 1979Significant correlation with bench press powe |
|
|
CKCU Test |
measure strength, endurance and CKC stability in the UE. Pt on knees for females and toes for males w/ hands just inside the tape lines which are 36 in apart. Instruct pt to move as quickly as possible and cross over touching each line alternatingly. Count # of touches in 15 s. Normative 18-20. reliable |
|
|
progression?? when |
Perhaps when they can perform at 85-90% of the uninvolved side or as compared to normative data |
|
|
selelct functional mov't assessment |
Algorithm to assess and classify movement and help direct the practitioner in manual techniques and exercise prescription |
|
|
regional interdependence |
concept that seemingly unrelated impairments in a remote anatomical region may contribute to, or be associated with, the patient’s primary complaint. |
|
|
injury causes altered motor control FSMA |
Previous injury is the best indicator for future injuryAnkle instability star excursion testingEMG studies for TA and LBP. regional interdependence |
|
|
crossed syndrome |
Upper- inhibited deep neck flexors, lower traps and SA; and facilitated upper trap and levator, SCM, pecs Lower- inhibited abs, glut min/max/med, facilitated RF, iliopsoas, thoracolumbar extensors |
|
|
FSMA neurodevelopment |
Patterns not individual muscle activationBreathing, rolling, prone on elbows, crawling, tripod, kneeling, standing, walking, running. Make sure the patterns are all correct, sequencing correctly |
|
|
top tier assessment gross mov'ts |
Active Cervical Flexion Active Cervical ExtensionActive Cervical Rotation/SidebendUpper Extremity pattern 1&2 (ER overhead and IR behind back)Multi-segmental Flexion Multi-segmental ExtensionMulti-segmental RotationSLSDynamic Leg swingOverhead squat |
|
|
top tier assessment provaction tests |
Impingement sign- pull arm across body. Horizontal Adduction- hand to opp GH and lift up. Pain w/ either? |
|
|
SFMA scoring |
Functional Non-painful (FN)Functional Painful (FP)Dysfunctional Painful (DP)Dysfunctional Non-painful (DN). No coachingObserve from the front, side and backIs there pain? |
|
|
SFMA active cervical flexion |
Should be able to touch chin to sternum w/ mouth closed |
|
|
SFMA active cervical ext |
Look to ceiling; about 10 degrees from parallel to ground |
|
|
SFMA active cervical rotation/sidebend |
Chin to collarbone, mouth closedNo shoulder elevation- usually suttle |
|
|
SFMA UE pattern 1 and 2 |
Up and over, touch opp shoulder blade- Down and up to touch shoulder blade- inferior angleWatch for lordosis, hinge at TL junction |
|
|
SFMA multi segment flexion |
Touch toes w/ no knee flexionTL junction over toesSacral angle >79 degrees |
|
|
SFMA multisegment ext |
Arms over head, arms in line w/ ears bend backASIS ant to toesSpine of scap post to heelsUniform spinal curve |
|
|
SFMA multisegment rotation |
Twist all the way to each sideStand directly behindShould see opp shoulder, no loss of height or vertical deviation, 50 degrees rotation at pelvis and shoulders |
|
|
SFMA SLS |
1 knee up to 90 and hold 10 seconds, no handsEach side, then do each side with eyes closedNo change in foot position, no loss of height, no arm flailing |
|
|
SFMA dynamic leg sign |
Stand on one side and swing other legLook for trendelberg, excessive pelvic rotation, leaning. No change in foot position, no loss of height, no arm flailing |
|
|
SFMA overhead squat |
Using a broom/stickFeet GH apart, arms over head and out to side, elbows at 90 then reach upSquat, keep heels on groundHip need to break 90, dowel remain up, tibia in line w/ trunk, toes do not rotate out. Do last. If anything in previous tests where no functional then this will not be functional. |
|
|
TED |
Mobility. tissue extensibility dysfunction. Crosses multiple joints Neural tension Muscle shortening (HS tightness) Active/Passive muscle insufficiency |
|
|
JMD |
Mobility. joint mobility disfunction. At 1 joint. OA. Fusion. Adhesive Capsulitis. Dislocation/Subluxation |
|
|
mobility tx |
Joint mobilization SNAGS/NAGS, MWM Taping Active Release Techniques Stretching Static/dynamic |
|
|
stability |
Static and Dynamic. Motor Control Dysfunction- HS dominance. Apical breathing. Prime mover compensation (hip flexors) |
|
|
stability tx |
Lumbar stabilization/cervical stabilization exercise. Taping/Bracing/Orthotics. Balance. Perturbations. Muscle firing sequencing. Hip stabilization exercise. Scapular stabilization Open chain/closed chain |
|
|
SFMA breakouts |
Recommend to start with dysfunctioal nonpainful mov't patterns. Algorithm tests all regions involved in the movement to isolate the limitations. Active vs passive. Weight-bearing vs non weight-bearing. Unilateral vs bilateralSingle joint vs multiple joints |
|
|
multisegment flexion breakout |
Single leg forward bendLong sitting forward bendActive Straight leg raise testPassive Straight leg raise testProne Rocking (Childs pose)Supine bilateral knees to chestRolling breakout |
|
|
rolling breakouts |
Legs are 'paralyzed'-Use the are opp of side you are rolling to to roll you to your stomach.Slow and controlled.Gh felx, H add, obliques.Use foam roll to prop up if they cannot get it.Then arms are paralyzed and only use opp leg to turn.Supine to prone UE lead.Supine to prone LE lead.Prone to supine UE lead.Prone to supine LE lead. |
|
|
mobility then stability |
reset, reinforce, reload. corrective exercises are in 4x4 model |
|
|
reset |
Manual techniquesImproved motor control with joint compression (PNF)Address chemical response (inflammation) |
|
|
reinforce |
Taping. Ergonomic changes. Orthotic. Bracing. Posture. Avoiding aggravating factors |
|
|
reload |
Corrective exerciseStretching/mobilizationStabilizationStrengthening |
|
|
corrective exercise 4x4 model |
|
|
|
lactate threshold |
The highest VO2 w/o a sustained rise in lactic acid. blood lactate/lactic acid may have a - effect on mm preformance due to increase in H ions, leads to increase in acidity of inter cellular environment. acidosis bad for mm contraction. |
|
|
bioenergetics |
Creatine phosphate for things 10s Anaerobic system- glycolysis 60-90s; lactic acid? Oxidative system >90s |
|
|
VO2 |
Measure of person’s ability to take in and useoxygen. O2 deficit: increase in uptake until = demands. Oxygen uptake remains above resting levels to restore the body to the pre-exercise conditio. 2 day to make any change, 3-5 recommended, elite 6x/w |
|
|
HR as exertions measurement |
HR max age predicted or Karvoene (HHR) Good correlation b/n HR and VO2 |
|
|
RPE |
Not used much w/ athletes b/c pain thresholds higher. 6-20; add a 0 = 0 HR |
|
|
long slow distance |
type of aerobic endurance training. Equivalent to approximately 70% VO2max Distances greater than race distance |
|
|
pace/temp aerobic endurance training |
Intensity close to or slightly higher than race/competition intensity Equal to lactate threshold |
|
|
interval training endurance training |
Intensities close to VO2max Work to rest ratio 1:1 |
|
|
rep training aerobic endurance |
Conducted at intensities greater than VO2max Typically last 30-90 seconds Work to Rest ratio 1:5 |
|
|
fartlek training- aerobic endurance |
Swedish for “Speed Play” Combination of a number of previously mentioned methods Involves easy running combined with either hills work or short fast bursts of running |
|
|
ACSM VO2 intensities |
The min training intensity threshold for improvement in VO2 is 40-50% to 85% of VO2max or 55-90% of maximum (HRRmax). Lower ranges for sedentary and unfit individuals For athletic population greater than 70% of VO2max or 75% of HRR |
|
|
resistance training steps |
Needs analysis Exercise selection Training frequency Exercise order Training load and repetitions Volume Rest periods |
|
|
Needs analysis (1) |
Eval sport- mov't, physiological, injury analysis Assess the athlete- training status, understanding, development |
|
|
exercise selection (2) |
specific to their activity, mm they use. Variables- equipment, time per session |
|
|
core exercises |
Recruit one or more large mm areas (i.e.; chest, shoulders, back, hip or thigh), involve 2 or more primary joints and receive priority when one is selecting exercises because of their direct application to the sport |
|
|
assistance exercises |
Recruit smaller muscle areas (i.e.; upper arm, abdominals, calf, neck, forearm, lower back and anterior lower leg); only involves one primary joint and are considered less important to improving sport performance. |
|
|
training frequency (3) |
# of session. Factors: training status, load and exercise type, sport season |
|
|
Hamstring and quad ratio |
The strength ratio of hamstrings to quadriceps should be at least 60 percent but ideally 75 percent. Suggested that higher H:Q torque ratios, and not muscle strength per se, are associated with a lower metabolic cost of running. |
|
|
exercise order (4)
|
Power, other core, then assistance exercises. Upper and lower body (Alternated). “Push” and “Pull” Exercises (Alternated. Supersets and compound sets |
|
|
superset |
two sequentially performed exercises that stress two opposing muscles or muscle areas (i.e.; agonist and antagonist) |
|
|
compound set |
sequentially performing two different exercises for the same muscles. |
|
|
training loads and reps (5) |
amount of weight assigned to an exercise set. rep max. based on goal of training and resistnace goal |
|
|
volume (6) |
amount lifted that training session. hypertrophy- 6-12 reps. endurance- 12 reps or more |
|
|
rest periods (7) |
goal? strength, power- longer period. hypertrophy- short to mod. endurance- very short |
|
|
clean |
clean and jerk, snatch. divide into things that make sense into the sport. engage nearly all of your muscles to move weights farther and faster than conventional exercises, and they activate your fast-twitch muscle fibers— the muscles with the greatest potential for size and strength. |
|
|
CNS adaptations |
Increased activity in motor cortex. § …especially as the level of force developed increases and when new exercises or movements are being learned |
|
|
PNS adaptations |
“Selective recruitment” of fast twitch muscle fibers- Bypassing traditional “size principle” and fire the fast twitch first. Ex- lifting car. Increase rate of motor unit firing. Increased size end plate at neuromuscular junction. Enhancement of muscle spindle (stretch reflex) response. |
|
|
agility |
broadly defined as an athlete’s collective coordinative abilities |
|
|
adaptive ability |
modification of action sequence upon observation or anticipation of novel or changing conditions and situations |
|
|
balance |
Static and dynamic equilibrium |
|
|
combinatory ability |
coordination of body movements into a given action |
|
|
preseason |
Focus on increasing intensity ® Address specific deficiencies |
|
|
in season |
Focus on maintaining fitness level. Frequency and Duration of exercise can vary without adverse effects on VO2max.However a small drop off in intensity can reduce VO2max significantly. |
|
|
post season |
Main focus on recovery |
|
|
periodization |
the systematic planning of athletic or physical training. The aim is to reach the best possible performance in the most important competition of the year. It involves progressivecycling of various aspects of a training program during a specific period |
|
|
periodization phases |
macro, meso, microcycles |
|
|
macrocycle |
long term goal. Emphasis on an athlete’s developmental status |
|
|
mesocycle |
medium term goal. Exploit complementary training effects at optimal times and minimize the compatibility problems associated with concurrent training |
|
|
microcycles |
short term. Task specificity- Sport specificity. Matching metabolic pathway.Fatigue management. |
|
|
hard style |
Much like sprints; general fitness; slight more variety 2 categories of exercises: ballistics and grind. Strong first, RKC, strength matters |
|
|
ballistic hard style |
accelerate the kettle bell and it continues floating. Kettle bell swing, clean, snatch Steep learning curve b/c no slow down. Requires tension and relaxation at same time- cyclical. Goal: is to apply maximal power into every lift no matter the weight. swing is foundation |
|
|
grind hard style |
if I stop applying force the kettle ball will stop moving. Squat variations, Turkish get up, army shoulder press. Goal: Get max tension throughout entire system to get most mov't in desired joints & stability in others 5 reps or less w/ high sets. Radiation. get up is foundation |
|
|
GS kettle bell style |
Competition style kettle bell lifting. Being as efficient as possible, loose, relaxed and smooth. Very specialty; not general fitness. Snatch, clean, jerk |
|
|
fitness kettle bell style |
Misuse of equipment- as a dumbbell w/ a handle |
|
|
radiation |
part of grind hard style kettle bells. a skill that needs developing, conscious effort to pulling all slack out of system. Hard work Strong and safer |
|
|
momentum and kettle bells |
Huge. Setting weight on foot vs dropping weight on foot. The weight you are lifting x 10 This is why TRAINING IS REQUIRED |
|
|
kettle bell technique |
Hip hinge- most of motion here, spine stays the same, 45 degrees to ground, GH higher than hips, hips higher than knees. Core- no excessive T arch. Supine, knees over hips, press w/ hands and tighten abs until no change b/n ribs and ab. |
|
|
dead lift, this before swing |
1. Stand over with kettle bell b/n heels (for teaching, may move forward later on)2. Pinky fingers in hips, bend hips until hands can touch kettle. Loads hips and keep cylinder more 3. Stand up w/ it. Make sure the core stays the same cylinder. Be really tight everywhere. 4. Back down |
|
|
get up |
Foundation for grind mov'ts. Supine, arm up, w/ weight in hand. Move from a flat back position to standing to back to flat back w/o bending arm. Different styles. Supporting the weight. 5 steps. alignment first then tension. curl around, in center, roll then lift. wrist straight. resisting the rotation |
|
|
kettle bell swing |
trunk is a tree, arms and bell are swing. foundation for ballistic mov't. same as dead lift but now 1 ft behind bell. |
|
|
physical fitness |
ability to carry out ADL w/ vigor and alterness w/o undue fatigue |
|
|
exercise |
PA that is planned, structured, repetitive, that has a final or intermediate objective- the improvement or maintance of physical fitness |
|
|
energy expenditure |
total amount of energy expended during exercise including resting energy expenditure |
|
|
PA |
any bodily mov't produced by skeletal mm that results in energy expenditure above resting levels |
|
|
MET |
an index of energy expenditure, the ratio of the rate of energy expended during an activity to the rate of energy expended at rest 1 MET = the uptake of 3.5 mL/kg/min; sitting at rest |
|
|
MET minutes |
quantifies the total amount of PA performed in a standardized manner across individuals and activitiesMETs x mins x days done |
|
|
CV/respiratory benefits from exercise |
Increase O2 uptake (# mito, CO, mm fiber changes, # myoglobil, # RBC), capillary density in skeletal mm, lactic acid threshold, exercise threshold for onset of dz s/s. Decrease HR and BP. |
|
|
reduction in CV dz risk w/ exericse |
Decrease systolic/diastolic BP, tryglicerides, intra-abdominal fat, insulin needs, blood platelets adhesiveness, inflammation. Increase HDLs- take fat from periphery to GI, liver, to excrete |
|
|
decreased mobidity and mortality w/ exercise |
Lower death rates CAD.Lower rates of- CVD, CAD, CVA, type 2 DM, metabolic syndromes, osteoporotic fx, colon cancer, breast cancer, gall bladder dz |
|
|
other benefits of exericse |
Decreased anxiety, depression, risk of fall, injury in older adults.Increased cognitive function, physical function and I living in older adults, feelings well being, performance of work, rec, sports |
|
|
preparticipiation PE |
BW- BMI, waist girth, body comp.Apical pulse- murmors, gallops, clicks, rubs.BP- seated, supine, standing.Auscultation of lungs.LE palaption for edema and arterial pulses.Inspection of skin for those w/ DM. |
|
|
low to mod risk lab tests |
Total cholesterol (<200), LDL (<100), HDL (>45) cholesterol.Tryglycerides (<150).Fasting plasma glucose (70-110).Thryoid function if dyslipidemia is present. |
|
|
high risk lab tests |
If high BP or high other tests. Resting 12 lead ECG, Holter monitor, coronoary angiography, echocardiography.Carotid ultrasound & other peripheral vascular studies.CXR.Blood chemistry panel and CBC |
|
|
modes of exercise testing |
Field tests-Cooper 12 min walk/run test; 6 min walk test; 1.5m test for time. Motor driven treadmill.Mechanically braked cycle ergometers. Stop test. |
|
|
aerobic exercise frequency and duration |
>/= 5d/w mod exercise or >/= 3d/w vigorous exercise or a combo 3-5 30-60min/d (150min/w) of purposeful, mod intensity.Or 20-60min/d (75min/w) of vigorous exercise or a combo. |
|
|
aerobic exercise type, volume, pattern, progression |
regular, purposeful exercise- major mm groups and continuous and rhythmic in nature 500-1000 MET min/w; >/= 7000 steps 1 session or >/= 10 min to accumulate the desired duration and volume; interval training may be effective gradual, adjust volume, frequency, duration, and/or intensity |
|
|
RT frequency, intesnsity |
each major mm group 2-3x/w 60-70% 1 RM (mod-hard) for novice to intermediate; >/= 80% 1 RM for experience, build mass; 40-50% (very light-light) 1 RM for older persons beginning RT, <50% (light-mod) 1 RM for endurance |
|
|
RT volume, reps, sets, pattern, progression |
each major mm group; variety is best 8-12 reps strength/power; 10-15 reps strength in middle age to older; 15-20 reps endurance 2-4 for stength and power; 1 for older and novice; 1-2 sets for endurance rest intervals 2-3 min b/n sets; rest 48h b/n session for a single mm group. gradual, resistace, reps, sers, frequency |
|
|
flexibility time and type, pattern |
PNF 3-6s; 20-75% max voluntary contraction followed by 10-30s assisted stretch is desired series of exercises for each mm group; static (active or passive), dynamic, ballistic, PNF all effective 2-4 of each, most effective when warmed up first |
|
|
neuromotor freq and intensity, type, pattern/volume, progression |
>/= 2-3x/w; >/= 20-30min/d effective intensity not determined balace, agility, coordination, gait, proprio; multifaceted- tai chi, yoga not established not established |
|
|
normal aging |
Will happen to us all.INcrease SBP.Decrease max HR, VO2 max.Artherosclerosis.Loss of motor neurons.Pereferntial loss of type II mm fibers.Overall decrease in lean mm and increase in fat mm-Less water content; dehydrated easier.Chainges in collagen-Increased stiffness; loss of elasticity |
|
|
sarcopenia |
age rleated loss of mm mass.Mm strength decreases w/ age.Begins at 40, most noticable after 60, accelerates at 80.Can loose up to 35% mm mass.Motor neuron loss- denervated fibers gets inn by adjacent nn.This loss is not enough to cause changes in function. |
|
|
collagen changes w/ age |
water loss in supporting matrix increased # crosslinks decreased elastisity |
|
|
wawter loss in supporting matrix |
Discs have less water, lose height. Articular cartilage can break down easier. Decreased ability to absorb shock. Decreased ROM |
|
|
increased # cross links |
Decreased ROM.Increased stiffness.Greater chance of avulsion vs rupture.Increased passive tension requiring more effort for mov't. |
|
|
age related increased risk |
HTN. Arthritis. Heart dz. Cancer. Diabetes. Hearing loss. Medication ADR's/side effects |
|
|
the 4 F's |
FunFunctionFrailtyFailure. Cross a threshold where they are at some point not able to do things that are fun anymore- can only do what is functional.From this then may cross a thershold where they become frail and does not have all the capacity to complete their ADLs.Then failure. Individual thersholds |
|
|
vigor |
overall physiological capacity |
|
|
fun |
physiological state that allows for unrestricted partipication in work, home and leisure activities |
|
|
function |
can do most work and home activities, may be modify how, start to self restrict their leisure activities |
|
|
frailty |
managing basic ADLs but that takes up all their capacity, limitations in community activites, may need assistance. Loss of reserve |
|
|
failure |
requires assistance w/ IADLs and ADLS, possible bedridden |
|
|
TUG Gait speed 6m walkl test 30s chair stand 4 square step test and 4Fs |
<8s, 9-20s, >20s -- >1.5m/s. 9-1.5m/s. 3-.8m/s <.3m/s 500m, 350-500m, 200-350m, <200m >15 reps, 8-15 reps, <8 reps, 0 reps <10s, 10-15s, 15-20s, >20s
|
|
|
CDC exercise recommendations older adults |
Option 1-2.5h /150min of mod aerobic/w.RT 2+ d/w major mm groups. Option 2-75 vigorous aerobic.RT 2+d/w. Option 3-Equivalent mix of mod-vigorous aerobic.RT 2+d/w. |
|
|
activity levels by age |
45-64y- 42% in no activity/exercise 65-74y- 50% 75+- 66% (16% could not lift 10#.21% could not walk up 10 strairs.29% could not walk .25mile.28% could not stoop, crouch, kneel.) |
|
|
HR max methods |
220-age (less reliable once over 40, underestimates) 208-.7(age) preferred method once over 40, underestimates when younger than 40 |
|
|
RT intensity for older adults |
60% 1RM min overload for mm adaptations; gains lost faster if stopped b/c motor learning.80% 1RM results in greater strength gains and cab be tolerated by even frail older adults. |
|
|
determing right resistance older adults |
Pick a resistance, do a couple reps, then have them rate b/n the 3 options- fairly light, somewhat hard, very hard. If somewhat hard- continue until they cannot- stop w/ fatigue. Increase speed, form decreases, tremor, concentration look, not full ROM. |
|
|
right resistance responses, %, # reps older adults |
Fairly light-somewhat-30-60%.12-15 rep; 60% about 15.Somewhat hard-hard-70-80%.8-12 reps.If less then somewhat hard w/ first few reps increase, if hard may need to drop down. 10% increases when able to do more than 15-Initial gains 6-8w.Long lasting gains 12-16w.May want to start around 40% if deconditioned and then be up to 60% by 4th session or so. |
|
|
RT sets, frequency, duration and older adults |
1 set in untrained is good.More sets- greater gains, also greater risk of injury.Time is also a factor for how many sets.Frequency should be 2-3x/w w/ 24-48h rest b/n groups.12-16 weeks. |
|
|
RT modes and older adults |
Functional greater gains in actual function.Resistance training group had greater gains in strength; did not carry over to function. |
|
|
power and older adults |
strength w/ speed.Often impaired in older adults.Need it for losses of balance, functional sit to stands and stairs. 20% 1RM and up to 60%.Fast con and slower ecc.OKC (speed in con) and functional exercises. 30s sit to stand |
|
|
home health |
provide services in the pt.'s home.Wide range.Less expensive, more convienty, just as effective as a hospital or SNF. Covered by ins45-60min. Interventions around and in home. High collaborative, be careful of overlapping services |
|
|
criteria 1 |
the pt. must either. Have a condition such that leaving homs is medically contraindicated. Illness/injury requires supportive devices, special transport, need help |
|
|
criteria 2 |
one of the above (contraindicated, inable to leave)+ there must be a normal inability to leave home and leaving home must require considerable and taxing effort |
|
|
goal of home health PT |
Safe and function at home vs in community.Most want to stay at home.Ther ex: develop pt's physical, physiological, and functional strength to ensure safe return to function within their home |
|
|
OASIS |
(outcome and assessment info set)Interventions are based on this tool. Outcomes are tracked w/ this tool. home health |
|
|
OASIS categories |
Functional capacity- physical performance testBarthel index2 min step test. TOUR Strength MMT TransfersTimed up and goSupine to sitting in chair transfers. BalanceDynamic gait indexFunctional reach4 square step test Walking6 min walk test50ft walk test |
|
|
Home as a gym |
Chair, recliner, lift chair (measure what they can get up from, set a goal to lower).Steps, stiars- multidirection.Towels.Sinks, counters.Pulleys, bands.Weighted vests.Tape measure, stop watch, slide board.All must be disinfected before you take it out., |
|
|
variables in home health program |
Set, reps.Time of day- highly variable, start at best time then move to worst times.Level of support available.Distractions- pets, TV, family, caregivers.Location- room, living community, mail box. |
|
|
dosing in homehealth program |
Priotitize functional ones.Greater than 60% 1RM.Speed matters-Super slow resistance can increase strength gains by 50% compared to normal speed.High velocity training can increase peak power in older women. |
|
|
HH strength tools |
Gravity.BW.Everyday weights.Weights.Resistance bands.Weighted vests/belts. Canned food- 12-16ozBox sugar- 1#Liter of water 2.2#Bag flour 5#Gallon water 8# |
|
|
Theraband 1 RM |
unpublished methodology.High variability w/ the length and how much weight that actually is. Requires: Appropriate/approximate color of band.Approximate 1RM.Length of arc of motion- tape measure.Resting length of band- where it is secured to hand- mark on band where each should be for consistency. |
|
|
transfer training HH |
Break down into constructive parts and trained individually.Involves: Global muscle strength, Local muscle strength, Power, Coordination, Balance. |
|
|
gait training HH |
Location, distance, device, skill and safetyModify- reps, length, time, speed, surface, time of day |
|
|
ADL HH |
Showering, grooming, dressing, cooking, housekeeping, entering and exiting.Involves: global mm strength, endurance, ROM, strength against gravity, balance.Progress sitting to standing, assisted to unassisted.Integrate into a part of their life- before getting out of bed, stand up 3x each.. |
|
|
HEP HH |
2-3 exercises.Task specific.Involve family or not?Written w/ pictures, exlpanation, and location for them.Integrate into a part of their life- before getting out of bed, stand up 3x each.. |
|
|
adhernece |
Patient contributes to plan, pt and clinician come to agreement on a plan; Pt follows plan.Adherence implies less paternalism and lower power differential between clinician and patient than compliance |
|
|
compliance |
Patient does as told. Pt is passive recipient |
|
|
concordance |
Suggests total involvement by pt in decisions and plan |
|
|
self efficacy |
belief in capability to complete an actionExercise task self efficacy- belief in ability to PHYSICALLY COMPLETE a task. barriers- fatigue, time. exercise barriers self efficacy- I can do ability in face of barriers. Get task efficacy first |
|
|
fostering adherence behavrioal theories |
self efficacy. outcome expectations. health benefits. stages of change |
|
|
outcome expectations w/ adherance |
What results someone expects from a behavior.More likely to change if change will lead to desirable outcome.Less likely if they believe they will fail, or will produce undesired outcome |
|
|
health beliefs w/ adherance |
Beliefs about condition influence willingness to change.Ex: “Bad backs run in my family” People will “act” (make changes) if they:Believe condition has serious consequences, they are susceptible to condition and action will decrease it,. they can be successfully. PT recognize what they bellieve and try to edu |
|
|
stages of change |
Precontemplation – no intention of making change. Contemplation – intends to make change. Preparation – taking steps toward making change; plans to make changes soon. Action – has changed the behavior (< 6 mos). Maintenance – has changed behavior (> 6 mos). |
|
|
how to increase self efficacy |
1. Successfully complete task2. Be told that they can “ “3. See someone else “ “ |
|
|
motivational interviewing |
conversation method that allows patient and provider to work together to make plan for achieving desired outcome. Pt. makes plans. Open-ended questions to explore thoughts and beliefs about condition and exercise. Use reflection and the pt's language. Cause? Role of exercise? Time for it? |
|
|
behavioral contracts/goal setting |
Use a patient/client-generated goal to create an action plan.SMART or ABCDEF.Enhances buy-in and accountability. |
|
|
replase prevention |
Identify situations likely to negatively influence ability to perform HEP.Create plans for maintaining HEP during these situations. |
|
|
Relapse remediation |
if-then” rules – a plan for slip-ups.“If I stop my HEP during my vacation, then I will re-start it within two days of returning home.” |
|
|
# exercises |
No more than 3!Under 3: best adherence (3,4).Important to explain HOW and WHY to do exercise.Provide a reference.Handout.Video or picture on phone. |
|
|
HH intervention categories |
Strength ADL Transfers gait Balance/fall prevention |