![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
169 Cards in this Set
- Front
- Back
|
THE NEAURAL TUBE IS IMPORTANT BECAUSE...? |
IT GIVES RISE TO ALL STRUCTURES FOR NERVOUS SYSTEM |
|
|
WHAT ARE THE PRIMARY BRAIN VESICLES THAT DEVELOP DURING WEEK 4? |
Prosencephalon (forebrain) Mesencephalon (midbrain) Rhombencephalon (hindbrain) |
|
|
ANY ANOMALIES RELATED W/ THE CNS MEANS WHAT? |
Neural tube defect |
|
|
WHAT IS THE MOST COMMON NEURAL TUBE DEFECT? |
Anencephaly |
|
|
WHAT IS ANENCEPHALY AKA? |
Aprosencephaly and atelencephaly |
|
|
IS ANENCEPHALY COMMON? |
No, it only occurs approx 1 in 1000 pregnancies and is not common in US --- only in England |
|
|
THERE IS A GREATER RISK FOR ANENCEPHALY WHEN...? |
Woman has history w/ prior pregnancy with open neural tube |
|
|
WHAT CAUSES ANENCEPHALY? |
Failure of closure of neural tube @ cranial end |
|
|
ANENCEPHALY IS MORE COMMON IN LADIES WITH WHAT? |
Uncontrolled diabetes and high in zinc |
|
|
WHAT IS THE RESULT OF ANENCEPHALY? |
absenceof cranial vault, complete or partial absence of forebrain, presence of brainstem, midbrain, skull base, facial structures |
|
|
WHAT IS INCLUDED IN PRENATAL DIAGNOSIS? |
Prenataldiagnosis often made with sonographyfollowing referral for high maternal serum alpha-fetoprotein (AF) levels |
|
|
WHAT IS ANENCEPHALY ASSOCIATED WITH? |
Canbe associated with Meckel-Gubersyndrome, trimsoy13, trisomy 18, or Amniotic bandsyndrome |
|

|
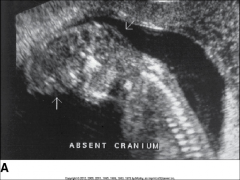
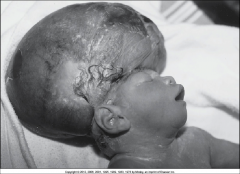
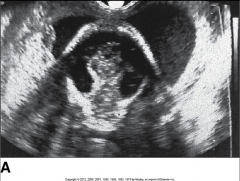
Ananencephalic fetus; absence of the brain and calvarium isidentified. Note the froglike appearance. |
|
|
Aprofile of the anomaly. |
|

|
Echogenicfoci were noted in the heart; amniocentesis revealed trisomy 13. |
|
|
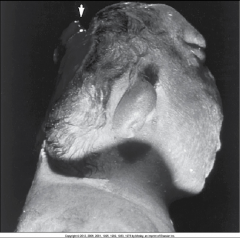
FIGURE59-2 Postmortemphotograph of anencephaly. The arrowpoints to the rudimentary brain (cerebrovasculosa). |
|
|
WHAT ARE OTHER SONOGRAPHIC FINDINGS OF ANENCEPHALY? |
Polyhydramnios Coexistingspinabifida and/or craniorachischisis Cleftlip and palate Hydronephrosis Diaphragmatichernia Cardiacdefects Omphalocele Gastrointestinaldefects Talipes |
|
|
WHAT IS ACRANIA? |
Lethal anomaly aka exencephaly and manifestsas absence of cranial bones with presence of complete, although abnormal,development of cerebral hemispheres |
|
|
WHEN WOULD ACRANIA OCCUR? |
4th gestational week |
|
|
HOW SHOULD YOU ESTABLISH DIAGNOSIS FOR ACRANIA? |
Presenceof significant brain tissue and lack of froglike appearance should establishdiagnosis |
|
|
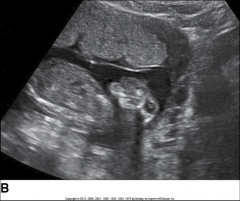
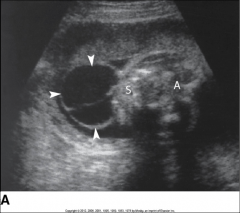
Thepresence of brain tissue without the presence of a calvarium. FIGURE 59-4A Acrania.Patient presented with an elevated maternal serum alpha-fetoprotein. Note theamnion (arrows)along the back of the fetus. Amniotic band syndrome was the probable cause |
|
|
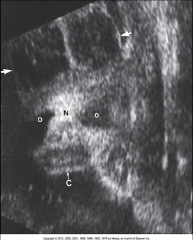
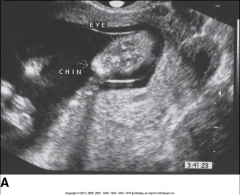
FIGURE 59-5 Coronalfacial view showing absence of the parietal bones (arrows), withhighly visible brain tissue (arrows)representing acrania or exencephaly. c,Chin; N, nose; o,orbits |
|

|
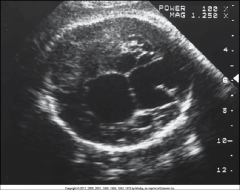
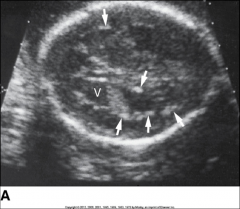
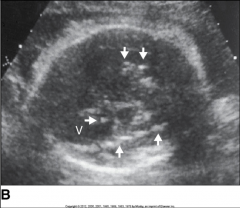
FIGURE 59-6 Inthe fetus shown in Figure 59-5, a transverse view shows the disorganized andfreely floating brain tissue (arrows). Thebrain anatomy is enhanced because of the absence of skull bones. Note theherniated ventricle (v) and sulcalmarkings |
|
|
FIGURE 59-7 Sameneonate shown in Figures 59-5 and 59-6, with acraniashortly after birth. The infant died within a few hours. |
|
|
WHAT IS A NEURAL TUBE DEFECT IN WHICH MENINGES ALONE OR MENINGES AND BRAIN HERNIATE THRU DEFECT IN CALVARIUM? |
Cephalocele |
|
|
WHAT TERM IS USED TO DESCRIBE HERNIATION OF MENINGES AND BRAIN THRU DEFECT? |
Encephalocele |
|
|
WHAT TERM IS USED TO DESCRIBE HERNIATION OF ONLY MENINGES? |
Cranial meningocele |
|
|
CEPHALOCELE OCCURS AT WHAT RATE? |
1 to 3 in 10,000 live births |
|
|
Prevalenceof 4:1 females over males; 6:1 prevalence of Caucasian over African-American describes what anomaly? |
Anencephaly |
|
|
WHAT PARTS ARE INVOLVED WITH CEPHALOCELE? |
Occipitalbone Parietal Frontal Temporalregions Otherbones of calvarium |
|
|
CEPHALOCELE MEANS... |
PROTRUSION OF THE BRAIN ... a pouch |
|
|
IF THE POUCH OF CEPHALOCELE CONTAINS MENINGES ONLY, WHAT IS IT CALLED? |
Meningocele |
|
|
IF THE POUCH OF CEPHALOCELE CONTAINS BRAIN TISSUE ONLY, WHAT IS IT CALLED? |
Encephalocele |
|
|
IF THE POUCH OF CEPHALOCELE CONTAINS MENINGES AND BRAIN TISSUE, WHAT IS IT CALLED? |
Encephalomeningocele |
|
|
IF THE POUCH OF CEPHALOCELE CONTAINS MENINGES, BRAIN TISSUE, LATERAL VENTRICLES, WHAT IS IT CALLED? |
Encephalomeningocystocele |
|
|
WHAT ARE US FEATURES OF CEPHALOCELE? |
Extracranialmass, which may be fluid- filled (cranial meningocele) orcontain solid components (encephalocele) Abony defect in skull Ventriculomegaly; ismore commonly identified with encephalocele
Polyhydramnios |
|
|
WHAT ARE CHROMOSOMAL ANOMALIES AND SYNDROME THAT HAVE BEEN ID'd WITH CEPHALOCELE INCLUDES...? |
trisomy13 and Meckel-Grubersyndrome |
|
|
WHAT IS SPINA BIFIDA? |
Wide range of vertebral defects that result from failure of neural tube closure so there is a cleft, or opening in spine |
|
|
WHAT MAY PROTRUDE THROUGH DEFECT W/ SPINA BIFIDA? |
Meninges and neural elements |
|
|
WHERE ALONG VERTEBRAL COLUMN DOES SPINA BIFIDA MOST COMMONLY OCCURS? |
Lumbar and sacral regions |
|
|
WHAT VARYING DEGREES OF NEUROLOGIC IMPAIRMENT IS SPINA BIFIDA ASSOCIATED WITH? |
minoranesthesia, paraparesis,death |
|
|
FETUSES WITH MYELOMENINGOCELE OFTEN PRESENTS WITH CRANIAL DEFECTS ASSOCIATED WITH...? |
Arnold-Chiari(type II) malformation |
|
|
IF YOU SEE A FETUS W/ SPINA BIFIDA... WHAT SHOULD YOU DO? |
Scan the brain and if you see enlarge ventricles and if there is ventriculomegaly it means that fetus has Arnold Chiari Type II malformation and you will not call it spina bifida |
|
|
WHEN YOU HAVE ARNOLD-CHIARI, SONOGRAPHIC FINDINGS INCLUDE...? |
Banana shape of the cerebellum |
|
|
TRUE OR FALSE: ARNOLD CHIARI LEADS TO OBLITERATION OF CISTERNA MAGNA. |
True |
|
|
WHAT DO CAUDAL DISPLACEMENT OF CRANIAL STRUCTURES IN ARNOLD CHIARI CAUSE? |
Scalloping of frontal bones of skull making fetal head resemble a lemon |
|
|
WHY WOULD FETUSES BE DELIVERED EARLY W/ SPINA BIFIDA? |
Ventricular shunting is usually by c section to preserve motor function |
|
|
WHAT ARE THE RISKS OF SURGICAL REPAIR OF DEFECTS IN UTERO? |
premature delivery, maternalmorbidity, fetal mortality |
|
|
WHAT DOES THE PROGNOSIS OF SPINA BIFIDA DEPENDING ON? |
Type, size, and location of defect |
|
|
WHAT MATERNAL FACTORS ARE ASSOCIATED WITH SPINA BIFIDA? |
Maternal diabetes, maternal obesity, hyperthermia, folic acid deficiency have been associated with spina bifida |
|
|
IF THERE IS A FAMILY HISTORY OF SPINA BIFIDA OR ANENCEPHALY, IS THAT A SIGNIFICANT RISK FACTOR FOR OCCURENCE OF SPINA BIFIDA? |
Hell yes |
|
|
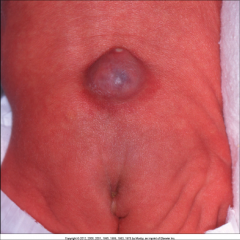
Aneonate with a lumbar myelomeningocele |
|
|
WHAT DOES DANDY-WALKER MALFORMATION MANIFESTS WITH? |
a genesis or hypoplasia of cerebellar vermis withresulting dilation on fourth ventricle and enlargement of posterior fossa. |
|
|
ALWAYS THINK OF THE POSTERIOR PART OF THE BRAIN WITH WHAT DEFECT? |
Dandy-Walker Malformation |
|
|
DIAGNOSIS OF DANDY-WALKER SHOULD NOT BE DONE BEFORE WHAT WEEK? |
18 |
|
|
WHAT ARE CHROMOSOMAL ANOMALIES ASSOCIATED W/ DANDY-WALKER? |
Trisomies 13, 18, 21, triploidy |
|
|
WHAT OTHER SYNDROME IS DANDY-WALKER ASSOCIATED WITH? |
Meckel-Gruber and Walker-Warburg |
|
|
IF MOMMY HAS CONGENITAL INFECTION OR DIABETES, IS RISK HIGHER FOR DANDY- WALKER? |
Yes |
|
|
WHAT DOES THE PROGNOSIS OF DANDY-WALKER DEPEND ON? |
Presenceor absence of associated anomalies and on degree of hypoplasia of cerebellar vermis, ascorrelates with severity of mental retardation |
|
|
MANY INFANTS WITH ISOLATED DWM HAS WHAT KIND OF IQ? |
Some may have subnormal IQ and some may have normal function |
|
|
WHAT WILL YOU SEE ON US W/ DWM? |
Posteriorfossa cyst Splayingof cerebellar hemispheres as result of complete or partial agenesis ofcerebellar vermis Enlargedcisterna magna caused by cerebellar vermisanomaly and posterior fossa cyst Ventriculomegaly |
|
|
WHAT IS THE CAUSE OF HYDROENCEPHALY? |
Obstruction of internal carotid |
|
|
IF OBSTRUCTION IS INSIDE BRAIN VENTRICLE, WHAT KIND OF HYDROENCEPHALY IS THAT? |
Non communicating |
|
|
PRESENCE OF SUBARACHNOID CYST MAY CAUSE WHAT? |
Non communicating hydroencephaly |
|
|
WHAT THREE TYPES OF SPINA BIFIDA ARE THERE? |
1. Occult spina bifida 2. Meningocele spina bifida 3. Meningomyelocele spina bifida |
|
|
WHAT TYPE OF SPINA BIFIDA HAS OPENING IN SPINE BUT NOTHING HAS BEEN PROTRUDED... THE OPENING IS COVERED BY SKIN AND HAIR AND CANNOT BE DETECTED ON US AND MOMMY'S AFP IS NORMAL? |
Occult spina bifida |
|
|
CAN OCCULT SPINA BIFIDA BE SURGICALLY SOLED? |
Yes because the hole is small with everything else normal in the baby |
|
|
WHAT TYPE OF SPINA BIFIDA INVOLVES ONLY PROTRUSION OF THE MENINGES? |
Meningocele |
|
|
WHAT SPINA BIFIDA IS MORE COMMON AND BOTH MENINGES AND NEURAL ELEMENTS PROTRUDE THRU DEFECT? |
Meningomyelocele |
|
|
WHAT IS TERMED FOR A SPINA BIFIDA DEFECT THAT IS VERY LARGE AND SEVERE AND INVARIABLY LETHAL? |
Rachischisis |
|
|
IN ARNOLD CHIARI II, WHAT WILL MAKE FETAL HEAD RESEMBLE A LEMON? |
Caudal displacement of cranial structures which causes scalloping of frontal bones of skull |
|

|
Splayingof the posterior ossification centers with a V or U configuration. |
|

|
Alarge spinal defect at the thoracic level is seen in the fetus. The prognosiswas expected to be extremely poor |
|

|
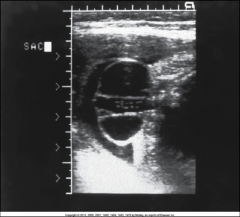
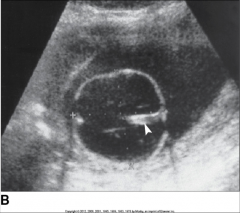
FIGURE 59-14A Sagittal(A) and transverse (B)views of the fetal spine (arrows)demonstrate this defect in the lumbar region consistent with a myelomeningocele |
|
|
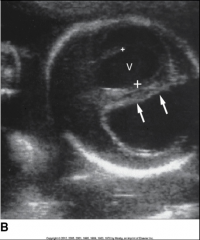
Meningomyelocele infetus with mild ventriculomegaly.Note the neural elements protruding into the sac. Protrusionof a saclike structure that may be anechoic (meningocele) orcontain neural elements (myelomeningocele). |
|

|
Spina Bifida open cleft in the skin |
|
|
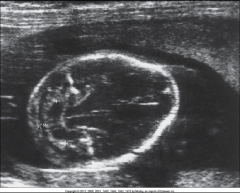
“Bananasign” in21-week fetus with lumbosacral meningomyelocele.Note lemon-shaped frontal bones consistent with frontal bossing. Flatteningof frontal bones, head “lemon”shape Obliterationof cisterna magnaInferiordisplacement of cerebellar vermis,giving cerebellum rounded, “banana”shapeVentriculomegaly |
|
|
Lumbosacralmeningomyelocele (arrows)shownin a 21-week fetus, detected on a basic fetal scan. A,Abdomen;S, spine. |
|
|
Lumbosacralmeningomyelocelemeasuring 6 cm (calipers) observed in a 33-week fetus during a basic fetalscan. |
|

|
Dandy-Walkercyst. Note the splayed cerebellar hemispheres. |
|

|
ThisDandy-Walker malformation was not associated with ventriculomegaly;amniocentesis revealed normal chromosomes. |
|

|
DWM with ventriculomegaly |
|
|
WHAT RESULTS FROM ABNORMAL CLEAVAGE OF PROSENCEPHALON (FOREBRAIN) AND ALSO FAILURE FOR IT TO DEVELOP INTO 2 HEMISPHERES? |
Holoprosencephaly |
|
|
TRUE OR FALSE: HOLOPROSENCEPHALY IS ASSOCIATED WITH SYNDROMES, GENETIC FACTORS, OR TERATOGENS AND MAY ALSO BE A SPORADIC EVENT. |
True
|
|
|
WHAT IS A TERATOGEN? |
Anything that exposes mom to have birth malformation such as radiation |
|
|
WHAT ARE THE THREE FORMS OF HOLOPROSENCEPHALY? |
Alobar - most severe Semilobar - intermediate form Lobar - mildest form |
|
|
THE THREE FORMS ARE DEPENDENT ON WHAT? |
The degree of failed hemispheric division |
|
|
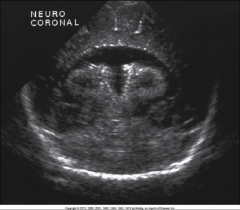
WHAT TYPE OF HOLOPROSENCEPHALY DO YOU GET WITH: •Singularmonoventriclebrain tissue that is small •Cup,ball, pancake configuration •Fusionof thalamus •Absenceof interhemisphericfissure •Absenceof cavumseptum pellucidum •Absenceof corpus callosum •Absenceof optic tracts •Absenceof olfactory bulbs |
Alobar holoprosencephaly |
|
|
WHAT ARE THE THREE MORPHOLOGIC TYPES OR CONFIGUARTION OF ALOBAR HOLOPROSENCEPHALY? |
Pancake Cup Ball |
|

|
3 types of alobar holoprosencephaly |
|
|
WHAT TYPE OF HOLOPROSENCEPHALY DO YOU GET WITH: Singularventricular cavity with partial formation of occipital horns Partialor complete fusion of thalamus Rudimentaryfalx and interhemisphericfissure Absentcorpus callosum Absentcavumseptum pellucidum Absentolfactory bulbs |
Semilobar |
|
|
FIGURE 59-27 Aneonatal ultrasound in a newborn revealed semilobar holoprosencephaly.There was no history of a prenatal ultrasound because of the normal course ofthe pregnancy. The infant lived for only a few weeks. |
|
|
WHAT TYPE OF HOLOPROSENCEPHALY WILL YOU GET WITH: •Almostcomplete division of ventricles with corpus callosum that may be normal, hypoplastic, orabsent •Cavumseptum pellucidum willstill be absent. |
Lobar |
|
|
WHY IN MOST SEVERE FORMS OF HOLOPROSENCEPHALY, FETUS DIES AT BIRTH OR SHORTLY THEREAFTER? |
Prognosis is considered uniformly poor |
|
|
IS SURVIVAL POSSIBLE FOR LEAST SEVERE LOBAR HOLOPROSENCEPHALY? |
Yes, but with severe mental retardation |
|
|
WHAT ARE FACIAL ANOMALIES THAT COME WITH HOLOPROSENCEPHALY? |
•Thefacial anomalies include cyclopia,hypotelorism, anabsent nose, a flattened nose with a single nostril, and a proboscis. |
|
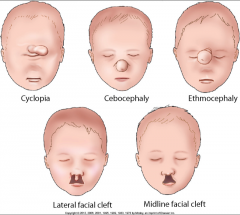
HOLPROSENCEPHALY FACIAL ANOMALIES |
Cyclopia = one eye Cebocephaly = monkey-like head, with a defective small, flattened nose with a single nostril or absent nose and closely set eyes Ethmocephaly = absent nose |
|
|
HOLOPROSENCEPHALY C-shaped monoventricle |
|

|
HOLOPROSENCEPHALY with a proboscis which is a long nose think of an elephant |
|

|
Holoprosencephaly |
|

|
HOLOPROSENCEPHALY:Polydactyly wasalso identified on all four extremities, suggesting the possibility of trisomy13. |
|
|
Fetuswith trisomy 13. Small eyes with hypotelorism. Probiscus seenabove the orbits. |
|
|
What do you get when there is a complete or partial absence of the corpus callosum? |
Agenesis of the corpus callosum |
|
|
WHEN DOES AGENESIS OF CORPUS CALLOSUM OCCUR? |
It occurs when the corpus callosum, the band of white matter connecting the two hemispheres in the brain, fails to develop normally |
|
|
WHY IS THE NORMAL DEVELOPMENT OF THE CORPUS CALLOSUM SO IMPORTANT? |
It aids in learning and memory |
|
|
DYSGENESIS OF THE CORPUS CALLOSUM DESCRIBES WHAT? |
Complete to partial absence of callosal fibers that cross the midline |
|
|
WHAT ARE THE CHROMOSOMAL ANMALIES THAT MAY ACCOMPANY ACC? |
Trisomies 21, 13, 18, and triploidy |
|
|
WHAT ARE SYNDROMES THAT HAVE BEEN ASSOCIATED WITH ACC? |
Aicardi, Apert, Opitz, Joubertsyndromes |
|
|
WHAT ARE THE MATERNAL DISEASES THAT CONTRIBUTE TO ACC? |
Diabetes Infections Alcohol abuse |
|
|
IS EXTRACRANIAL OR INTRACRANIALS THAT ARE ASSOCIATED WITH ACC? |
Extracranial |
|
|
WHAT DOES THE PROGNOSIS OF ACC DEPEND ON? |
High incidence of associated anomalies but many carry poor prognosis |
|
|
ACC MAY BE AYMPTOMATIC OR ASSOCIATED WITH MENTAL RETARDATION AND OR SEIZURES. TRUE OR FALSE? |
True |
|
|
WHAT SONOGRAPHIC FEATURES DO THESE BELONG TO? •Absenceof corpus callosum•Elevationand dilation of third ventricle•Widelyseparated lateral ventricular frontal horns with medial indentation of medialwalls•Dilatedoccipital horns (colpocephaly),giving lateral ventricles teardrop shape•Absenceof cavumseptum pellucidum |
ACC |
|

|
A,Agenesis of the corpus callosum is diagnosed in this fetus with an absent cavumseptum pellucidum |
|

|
ACC: The occipital horn of the lateral ventricle also appears dilated |
|
|
WHAT IS THE RESULT OF OBSTRUCTION, ATRESIA, OR STENOSIS OF AQUEDUCT OF SYLVIUS WHICH CAUSES VENTRICULOMEGALY? |
Aqueductal stenosis |
|
|
WHAT DOES THE AQUEDUCT OF SYLVIUS DO? |
Connect the third and fourth ventricles and it also explains the enlargementof lateral ventricles and third ventricle in presence of normal fourthventricle |
|
|
WHAT KIND OF INFECTION MAY RESULT FROM AQUEDUCTAL STENOSIS? |
Intrauterine infections |
|
|
WHAT KIND OF MASS AND HEMORRHAGE ARE ALSO CONTRIBUTING FACTORS OF ACQUIRED OBSTRUCTION? |
Cranial masses and ventricular hemorrhage |
|
|
Primary aqueductal stenosis is usually __-linked and has _______-__________ inheritance. |
X-linked Auto-somal recessive (both parents) |
|
|
AQUEDUCTAL STENOSIS HAS A _______ PROGNOSIS AND VARIES WITH ASSOCIATED _____________. |
Poor Anomalies |
|
|
APPROX 90% OF SURVIVORS OF AQUEDUCTAL STENOSIS HAVE AN IQ OF WHAT? |
BELOW 70 |
|
|
INFANTS WITH X-LINKED AQUEDUCTAL STENOSIS ARE PROFOUNDLY WHAT? |
Mentally retarded |
|
|
WITH AQUEDUCTAL STENOSIS, US FEATURES OF THE LATERAL VENTRICLES ARE...? |
Enlarged! And may be a sign of severe aqueductal stenosis |
|
|
TRUE OR FALSE: WITH AQUEDUCTAL STENOSIS, THE FOURTH VENTRICLE IS DILATED. |
False, you get third ventricular dilation |
|
|
IN X-LINKED FORM OF AQUEDUCTAL STENOSIS, YOU GET WHAT OF THE THUMB? |
Flexion and adduction |
|

|
Ventricularview in a fetus with acquired aqueductalstenosis caused by parvovirus infection. Dilatation of the ventricular system (v)resultedfrom inflammation, causing obstruction to the flow of cerebrospinal fluid. Thefetus was severely hydropic.Note the significant scalp edema (E |
|

|
Inthe same fetus, third ventricle (3v) dilatation is demonstrated. Cordocentesis wasperformed to find a cause for the severe nonimmune hydrops, andparvovirus was detected within the fetal blood. The fetus died shortly afterbirth. E, Scalp edema. |
|

|
Asagittal image of a fetus with severe hydrocephaly that was thought to resultfrom aqueductalstenosis. |
|
|
WHAT IS THE CONDITION WHERE THERE IS DESTRUCTION OF CEREBRAL HEMISPHERES BY OCCLUSION OF INTERNAL CAROTID ARTERIES? |
Hydranencephaly |
|
|
WHAT IS DESTROYED AND REPLACED BY CSF IN HYDRAENCEPHALY? |
Brain parenchyma |
|
|
WHAT IS STILL PRESENT IN HYDRANENCEPHALY? |
Midbrain and cerebellum |
|
|
TRUE OR FALSE: THERE IS COEXISTING STRUCTURAL OR CHROMOSOMAL ANOMALIES ASSOCIATED. |
False, there is no coexisting structural or chromosomal anomalies are associated |
|
|
WHAT IS THE PROGNOSIS OF HYDRANENCEPHALY? |
Grave with death occurring at birth or shortly thereafter |
|
|
ARE THERE POSSIBLE SURVIVORS OF HYDRANENCEPHALY? |
Some long-term survivors have been reported |
|
|
WHAT DO THE FOLLOWING DESCRIBE? •Absenceof normal brain tissue with almost complete replacement by cerebrospinal fluid •Absentor partially absent falx•Presenceof midbrain, basal ganglia, cerebellum•Choroidplexus may be identified.•Macrocephalymay occur. |
US features of hydranencephaly |
|
|
WHAT MAY HYDRANENCEPHALY BE CONFUSED WITH? |
Hydrocephaly |
|
|
WHAT MAY HELP IN DIFFERENTIATING HYDRANENCEPHALY FROM HYDROCEPHALY? |
Presence of intact falx and surrounding rim of brain parenchyma may |
|
|
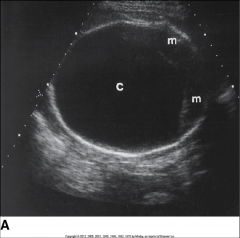
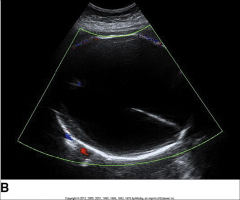
Hydranencephaly (c) in afetus at 33 weeks’gestation showing a massive collection of cerebrospinal fluid. Note the braintissue in the occipital region (m) |
|
|
Ina different fetus at 37 weeks’gestation, hydranencephaly isidentified. The head measurements were greater than the 95th percentile, so theinfant was delivered by cesarean section |
|
|
WHAT REFERS TO DILATION OF VENTRICLES WITHIN BRAIN |
Ventriculomegaly |
|
|
WHAT OCCURS WHEN VENTRICULOMEGALY IS COUPLED WITH ENLARGEMENT OF FETAL HEAD? |
Hydrocephalus |
|
|
WHAT IS THE OCCURENCE OF HYDROCEPHALUS? |
0.3 to 1.5 per 1000 live births |
|
|
WITH VENTRICULOMEGALY (HYDROCEPHALUS), ENLARGEMENT/DILATION OF VENTRICLES OCCURS WITH OBSTRUCTION OF....? |
CSF flow |
|
|
WHEN IS A VENTRICLE CONSIDERED TO BE DILATED? |
When its diameter exceeds 10 mm |
|
|
WHEN HYDROCEPHALUS OCCURS WITH OBSTRUCTION THAT MAY BE CAUSED BY VENTRICULAR DEFECT LIKE AQUEDUCTAL STENOSIS, WHAT IS THIS REFERRED TO AS? |
Non communicating hydrocephalus |
|
|
WHEN OBSTRUCTION IS OUTSIDE OF VENTRICULAR SYSTEM SUCH AS WITH ARACHNOID CYST, WHAT KIND OF HYDROCEPHALUS IS THIS? |
Communicating hydrocephalus |
|
|
VENTRICULOMEGALY (HYDROCEPHALUS) COMMUNICATING TYPE withMultiplearachnoid cysts. |
|
|
WHY IS IT CALLED NONCOMMUNICATING HYDROCEPHALUS? |
Because the obstruction occurs within the ventricular system, the ventricles and subarachnoid space do not communicate |
|
|
WHY IS IT CALLED COMMUNICATING HYDROCEPHALUS? |
The obstruction occurs outside the ventricular system so the ventricles and the subarachnoid space communicate. |
|
|
WHAT WILL CAUSE VENTRICULAR EXPANSION WITH VENTRICULOMEGALY (HYDROCEPHALUS)? |
The increase in pressure within the ventricular system |
|
|
WHY DOES IRREVERSIBLE BRAIN DAMAGE OCCUR WITH VENTRICULOMEGALY/HYDROCEPHALUS? |
The enlarged ventricles may exert pressure on brain tissue |
|
|
Periventricularcalcifications (arrows) and ventriculomegaly (v)ina 20-week fetus. An infectious cause was suspected. All testing had provednegative. |
|
|
Inthe same fetus at 30 weeks’gestation, persistent periventricular calcifications (arrows)withventriculomegaly (v)wereobserved. No other anomalies or complications were present. |
|
|
WHAT IS VENTRICULOMEGALY/HYDROCEPHALUS A MANIFESTATION OF? |
Syndrome or chromosomal abnormality |
|
|
WHAT ARE COMMON CAUSES OF VENTRICULOMEGALY? |
Spina bifida and encephaloceles |
|
|
VENTRICULAR ENLARGEMENT HAS BEEN LINKED TO WHAT? |
Congenital infections such as toxoplasmosis and cytomegalovirus |
|
|
SONOGRAPHIC FEATURES OF VENTRICULOMEGALY/HYDROCEPHALUS INCLUDE: 1. Lateral ventricular enlargement > ____ mm 2. "______ ______ _____," as gravity-dependent choroid plexus falls into increased ventricular space 3. Possible dilation of _____ and ____ ventricles 4. Fetal head enlargement when biparietal and HC mrasurements __________ those for established ga. |
1. 10 2. Dangling choroid sign 3. 3rd and 4th 4. exceed |
|
|
Proximalventricle measured 28 mm in diameter. Note the asymmetry between theventricles. Topone more than 8 mm is considered to be dilated (v)Downstream needs to be more than 10 mm to be dilated |
|

|
Theanterior choroid plexus “dangles” intothe posterior ventricle. |
|
|
WHAT IS TERMED AN ABNORMALLY SMALL HEAD THAT FALLS TWO STANDARD DEVIATIONS BELOW THE MEAN? |
Microcephaly |
|
|
WHY DOES MICROCEPHALY OCCUR? |
Brain is reduced in size |
|
|
TRUE OR FALSE: Isolatedmicrocephaly occurs in 1 per 1000 births; more commonly caused by associatedanomaly |
True |
|
|
IS MICROCEPHALY A RESULT FROM INHERITANCE OF AUTOSOMAL-DOMINANT OR AUTOSOMAL-RECESSIVE PATTERN? |
Could be both! |
|
|
WHAT TERATOGENS ARE LINKED WITH MICROCEPHALY? |
congenitalinfections (rubella, toxoplasmosis, cytomegalovirus), maternal alcohol abuse,heroin addiction, mercury poisoning, maternal phenylketonuria, radiation, andhypoxia. |
|
|
WHAT PERCENTAGE OF MICROCEPHALY ARE MENTALLY RETARDED? |
85% |
|
|
WHAT ARE SONOGRAPHIC FEATURES OF MICROCEPHALY? |
•Small biparietaldiameter •Smallhead circumference •Abnormalhead circumference/abdomen circumference and head circumference–to–femurlength ratios |
|

|
Microcephalyis demonstrated in this fetus with semilobar holoprosencephaly. |
|

|
Inthe same fetus, the profile shows the small head; the fetus also had abilateral cleft lip.(shadowing from the nose/mouth is cleft palette) |