Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
73 Cards in this Set
- Front
- Back
|
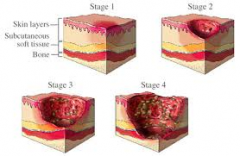
four stages of a decubitus ulcer
|
|
|
NANDA diagnoses related to wounds
|
Impaired skin integrity
Acute pain Fear Imbalanced Nutrition |
|
|
barrier to protect the body from potentially harmful external environment
|
the skin
|
|
|
any abnormal break in the skin
|
wound
|
|
|
inspect the client's skin carefully upon admission to a facility, and frequently thereafter...
|
for any signs of pressure or skin breakdown
|
|
|
It is important to prevent skin breakdown
|
and if it occurs, notify PCP
|
|
|
* a physical injury causing a break in the skin or mucous membrane
|
wound
|
|
|
* rubbing off of the skin's surface, i.e. skinned knee
|
abrasion
|
|
|
* stab wound
|
puncture
|
|
|
* wound with torn edges, i.e. an accidental or self-inflicted cut
|
laceration
|
|
|
intentional, non-self inflicted wound
|
surgical incision
|
|
|
other types of abnormal skin conditions
|
infections, rashes, lesions, and burns
|
|
|
skin inspection includes both
|
visual and palpation, with emphasis on bony prominences
|
|
|
do not massage any discolored or reddened pressure points
|
this can add to the irritation and accelerate skin breakdown
|
|
|
Inspection sites include
|
head, ears, heels, coccyx, shoulder blades, elbows, etc. as well as IV sites, NG tubes, tracheostomy tubes
|
|
|
vascular ulcers may be evaluated with
|
angiograms or laser Doppler, lab testing (biopsy, and wound culture)
|
|
|
clear, thin, watery drainage
|
serous
|
|
|
composed of some serum and some blood
|
serosanguineous
|
|
|
contains pus
|
purulent
|
|
|
green, tan, yellow, red
|
puss colors
|
|
|
malodorous, no odor, sweet smelling
|
puss odors
|
|
|
drainage containing a great deal of protein and cellular debris
|
exudate
|
|
|
25% of dressing
|
small
|
|
|
30-60% of dressing
|
moderate
|
|
|
60-75% of dressing
|
large/copious
|
|
|
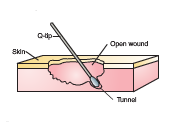
tunneling
|
|
|
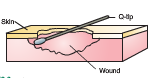
undermining
|
|
|
can be rolled under, macerated, calloused, open
|
wound edges
|
|
|
intact, pink, erythema (redness), excoriated (scratch or abrasion), blistered, ecchymotic (hemorrhage spot), denuded (skin stripped away), macerated (moistened) etc.
|
periwound area
|
|
|
a ruler is used to measure the length and width of a wound
|
linear measurement
|
|
|
graph paper is used to duplicate the shape of a wound, include scale
|
planimetry
|
|
|
special video camera downloads to a computer, provides color images and some indication of depth
|
stereophotogrammerty
|
|
|
photos of the wound
|
wound photography
|
|
|
transparent paper may be laid over the wound and edges lightly traced
|
wound tracing
|
|
|
causes of skin breakdown
|
immobility, inadequate nutrition, hydration levels, external moisture, mental status, sensory loss, fever, low bp, infancy
|
|
|
moisture, meticulous skin care, located anywhere on the body, diffuse pattern, limited to dermis/epidermis
|
Incontinence associated dermatitis
|
|
|
pressure, turn often, bony prominances, surrounding bony areas only, may extend to muscle or bone
|
pressure ulcer
|
|
|
the rubbing of one surface against another
|
friction
|
|
|
the interaction of friction and gravity when tissue is moved across material
|
shear
|
|
|
develop most often in lower extremities as a result of local hypoxia
|
venous stasis ulcer
|
|
|
may occur in people who have diabetes mellitus
|
diabetic ulcer
|
|
|
pressure ulcers can also be complicated by
|
yeast infections
|
|
|
how to document pressure ulcers on a person at the time of admittacne
|
"present on admission"
|
|
|
primary factors of pressure ulcer development
|
intensity and duration of pressure...and tissue tolerance of pressure
|
|
|
these factors are considered in pressure ulcer development
|
sensory perception, moisture level, activity, mobility, nutrition, friction/shear
|
|
|
If the outside of a would is sealed before the before the area underneath has healed
|
an abscess often forms, which may be sterile or infected
|
|
|
new tissue that forms when old destroyed tissue is sloughed off
|
granulation tissue
|
|
|
if a client is transferring, with a wound...
|
alert department and take steps to protect wound and prevent infection
|
|
|
if an area is already reddened, do not
|
rub or massage it
|
|
|
to promote wound healing, a client should eat
|
a high calorie, high protein diet with extra vitamin C
|
|
|
many immobile clients can be aided by what devices to help prevent skin breakdown
|
special beds or mattresses
|
|
|
wounds with minimal tissue loss, such as surgical incision
|
first intention (primary intention)
|
|
|
occurs with tissue loss, the wound edges are widely separated, deep lacerations , burns and pressure ulcers
|
second intention (secondary intention)
|
|
|
there is a delay between the injury and the closure of the wound
|
third intention (tertiary intention)
|
|
|
Telfa pads, ABD pads and Surgi-pads function
|
to collect drainage and protect the wound
|
|
|
dressing intended to protect a wound from contamination
|
dry, sterile dressing (dry-to-dry)
|
|
|
debridement or cleansing or a wound by saturating a sterile dressing with normal saline or sterile solution, placing it on or into the wound, allow it to dry.
|
wet-to-dry dressings, commonly used for infected wounds by secondary intention
|
|
|
done most often with a puncture wound that has a sinus tract
|
wound packing, which may be dry or impregnated with petrolatum or medication, special gel-foam or sponge material may also be used for this purpose.
|
|
|
used on clean, open wounds or on wound that are granulating in
|
wet-to-wet dressing
|
|
|
When using duo-derm, be sure to get adequate coverage of the wound
|
at least a 1 inch margin
|
|

|
Penrose drain
|
|

|
A. Jackson-Pratt B. Hemovac
|
|
|
negative pressure device
|
Vacuum Assisted Closure
|
|
|
Infected wounds are still irrigated with sterile fluid because
|
this helps prevent the introduction of additional pathogens
|
|
|
suture staple removal after
|
7-10 days
|
|
|
When removing staples or interrupted sutures, remove
|
every other one and inspect for dehissance
|
|
|
antiseptic is applied to the skin prior to placement of steri strips
|
because the antiseptic cleans the wounds and dries to help steri strips stick better
|
|
|
clients with steristrips are encouraged to shower instead of baths
|
to allow the steristrips to fall off naturally
|
|
|
intact skin, firm/boggy/mushy skin, persistent redness ( blue/purple in darker skinned people)
|
Stage I
|
|
|
loss of epidermis, damaged dermis, partial thickness loss, shallow crater, blister-like appearance
|
Stage II
|
|
|
full thickness loss, subcutaneous tissue involved, fat may be visible, not painful, possible odor, may show undermining/tunneling
|
Stage III
|
|
|
full thickness loss, exposed bone, muscle, tendons, often extensive tunneling
|
Stage IV
|
|
|
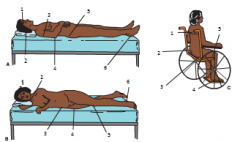
(A) Occiput, rim of ear, dorsal thoracis area, elbow, sacrum/coccyx, heel
(B) side of head, shoulder, ischium, trochanter, anterior knee, malleolus, (C) shoulder blade, sacrum coccyx, ischial tuberosity, foot, posterior knee |