Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
46 Cards in this Set
- Front
- Back
|
Tetraplegic & Paraplegic Levels
|
T1/C8 above and below
|
|
|
SCI Epidemiology
|
• Incidence of Traumatic SCI in Australia (>15
y.o.) : 15-17 cases per million per year • Peaks at 15-24 & 65-74 • 82% male • 52% paraplegic and 47% quadriplegic. • Average age of spinal cord injured person is 31. |
|
|
Causes of SCI
|
Cause (04-05) %
Motor Vehicle 25 Motorcyclists, cyclists, pedestrians 24 Low Falls (< 1 m) 10 High Falls (> 1m) 29 diving or surfing 9 Hit / Struck by an object 10 Other Causes 3 |
|
|
Aetiology of Non-traumatic SCI
|
• Spinal Stenosis, Intervertebral disc herniation,
RA • Vascular • Inflammatory – infectious (viral, bacterial, fungal, parasitic) – Non-infectious (transverse myelitis, MS, polio) • Tumor • Iatrogenic: Radiation, Contrast arachnoiditis • Others: Syringomyelia, MND, vitamin B-12, Friedreich ataxia. |
|
|
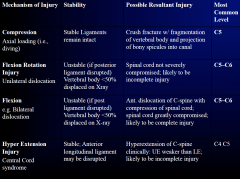
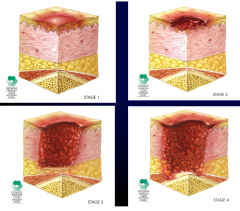
Mechanical Injuries
|
|
|
|
Compression Fractures
|
axial forces
- can also cause a burst fracture, and most are pretty stable if they dont affect the ligaments EXCEPT the jefferson fracture |
|
|
Flexion Rotation Injuries
|
rotatory component involved
- shallow and slopy facets joints - flat cevival CERVICAL joints can therefore jump ontop of each other, thus locks ontop of each other (need surgical to unlock) can also affect the ligaments as well as the verterbral aa. thus causing clots or stuff... |
|
|
Flexion Injuries
|
BILATERAL DISLOCATION: one part of the spinal column moves anteriorly the other moves posteriorly thus the cord is dramatically affected
TEARDROP FRACTURE: osteoarthritic spurs also can affect the spinal cord (compressions) |
|
|
Most Spinal Cord Injury occurs at:
|
C4,5,6 (the most flexible part of the spinal column)
|
|
|
Standard Neurological Classification of SCI
|
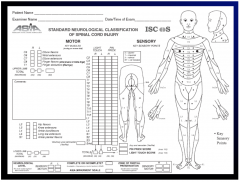
- classify the last level with some preservation still on each side
AIS-A complete injury AIS-B incomplete injury |
|
|
Syndrome of Spinal Cord Injury
|
Central Cord Syndrome
Brown Sequard Syndrome Anterior Cord Syndrome |
|
|
Central Cord Syndrome
|
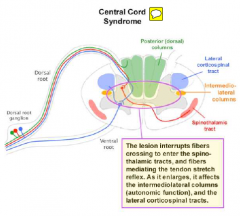
greater weakness in upper limb, rather than lower lims
|
|
|
Anterior Cord Syndrome
|
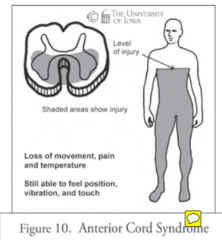
anterior spinal aa. comes form the aorta, thus hypertension here can cause the syndrome (affects motor power)
|
|
|
Brown-Sequard Syndrome
|
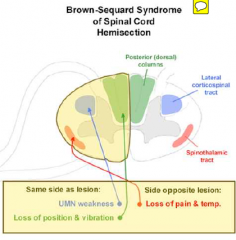
contralateral loss of pain and temp, and ipisilateral of touch, power...
|
|
|
Crossection of spinal cord with main tracts
|
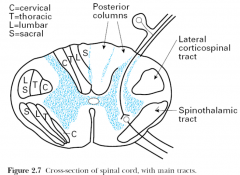
central cord syndrome because the cervical tracts are laminated nearer to the tracts-
thus the upper tracts are more affected |
|
|
Consequences of SCI
|

• Impairment of control of movement
& sensation • Defective/absent bladder & bowel function • Impaired fertility and sexuality • Defective control of autonomic function • Blood pressure (Autonomic dysreflexia) • Sweating • Temperature • Inadequate respiratory function • Uncontrolled activity of the isolated spinal cord • Spasticity • Pain • Musculoskeletal complications • Psychosocial impact |
|
|
Autonomic Dysreflexia (AD)
|
• Sudden onset of severe hypertension
– At or above T6 – Isolation of Sympathetic Nervous System (SNS) from vasomotor centres of brain • Potentially life threatening condition – requires immediate attention. – Can lead to: - Hypertensive encephalopathy - Intracerebral haemorrhage - Seizures - Cardiac Arrhythmias |
|
|
Pathophysiology of AD
|
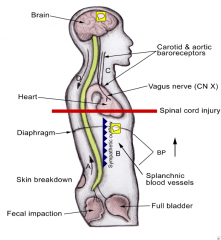
SYMPATHETIC OUTFLOW: can recieve input for strong spina reflexes below and causes SNS thjus vasoconstrictors
BRAIN: will try to decreases, the BP, slow HR, and vasodilate only where there is still brain control (since it has no idea of what is going on below the injury) |
|
|
Triggers of AD
|
• Genitourinary - Over distension, UTI, stones, DSD, epididymoorchitis
• Bowel – impaction, hemorrhoids, gastric ulcers, appendicitis, gallstones • Sexual stimulation, labour, menstruation, vaginitis • Skin - Ingrown toe nails, pressure areas, burns, insect bites, tight clothing, shoes, or appliances • MSK: Heterotopic bone, #s • Procedures - Urodynamics, Cystoscopy • Others: DVT, PEs, Temperature fluctuations |
|
|
Presentation of AD
|
- pounding headache
- SoB - Sweating - Goose Bumps - Slow pulse - Flushing or blotching of the skin - Slow pulse - Nasal Congestion - restlessness or anxiety |
|
|
Tx of AD
|
• Sit patient as upright as possible
• Call for help & monitor blood pressure • Remove or loosen all tight clothing (TEDS & abdominal binder) • Check drainage system for kinks/clots/sediment • Empty leg bag • Attempt to identify cause • Refer to AD Treatment Card/Algorithm and RSCIP Fact sheet 1. BLADDER Tx; catheter.. 2. After excluding bladder distention, manually evacuate full rectum with LOTS of lignocaine and watch BP fall 3. If not look for other causes |
|
|
Pharmacological Treatment of AD
|
Medication may be needed if the cause of AD is not
easily remediable / is over 170 mm Hg • Glyceryl Trinitrate as: – sublingual spray or – 1/2 Anginine tablet (repeated every 5-10 min) or – 5mg/24 hr patch. Warning: Do not use GTN spray/tablets if PDE5I or other nitrate containing meds have been used) • Captopril 12.5mg sublingual • Adequate analgesia when appropriate • Patient may require admission to Hospital if AD does not resolve |
|
|
Susceptibility to Autonomic Dysreflexia
|
• Susceptibility to Autonomic Dysreflexia is
increased for 48 hours after an episode has concluded, during that time: – BP should be monitored – Invasive procedures/instrumentation should be minimised • Patient should have: – Education on proper bladder, bowel and skin management techniques – Plan for when AD does occur – AD Medical Emergency Card, Medicalert bracelet – Up to date prescription of GTN THUS pain relief is important even though they cant feel it |
|
|
Micturition Pathways
|

|
|
|
Bladder Goals
|
• Maintain social continence
• Protect upper urinary tracts from sustained high (ie. >40cm H20) pressures • Prevent complications • Choose technique compatible with person’s functional capacity and lifestyle |
|
|
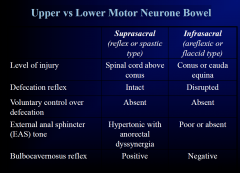
UMN vs LMN Bladder
|
LMN bladder, no hyperreflxic but still can be not soo strecthy, so it wont relax as muxh as normal but u wont have the problems with the spincter in the UMN bladder
- more likely to get inconteince in LMN bladder |
|
|
Genitourinary
Complications |
• Increased intravesical pressures, reduced
compliance, detrusor hyper-reflexia, incomplete emptying • Hydronephrosis, upper tract deterioration & renal failure • Urinary tract infections, epididymoorchitis • Bladder & Renal calculi • Fistulae / stricture of the urethra (CISC) • Increased risk of bladder cancer with long-term IDC/SPC • Do not forget prostate CA |
|
|
Upper vs Lower Motor Neurone Bowel
|
|
|
|
Gastrointestinal Complications
|
• Complications increase with time post injury
– Constipation/incontinence – Abdominal pain & distention (43%) – Haemorrhoids (74%) – AD related GIT (43%) – Difficulty with bowel evacuation (20%) – Severe oesophagitis – Gallstone disease (7x) – Megacolon/ recurrent sigmoid volvulus (poo in the intestines backed up) • ? Colorectal CA |
|
|
Sexual Function Effects
|
• Changes in arousal response
- decreased sensation - decreased lubrication - decreased clitoral engorgement - erectile dysfunction • Changes in orgasm - decreased or absent sensation - few males achieve true ejaculation (4-5% in complete cords) - brief erection with rapid dribbling emission |
|
|
Interventions for erectile dysfunction
|
• Education of patient and partner re:preparation, physical techniques and discuss psychosocial aspects
• Oral - Sildenafil (Viagra), Vardenafil (Levitra), Tadalafil (Cialis) • Nasal, sublingual, intraurethral, transdermal • Intracavernosal Injection of vaso-active substances (e.g. Prostaglandin E1, Papaverine HCl) • Vacuum tumescence device • Newer medications: apomorphine • Sacral stimulation (Brindley) • Penile prosthesis (silicone rods or inflatable) |
|
|
Why do UMN become hyperreflexic?
|
the brain has inhibitory input into the spinal cord thats why when u release its control u become hyper reflexic...
|
|
|
Male Feritility
|
• Impaired due to
– erectile dysfunction – reduced ability to ejaculate – impaired semen quality • Most will require significant medical intervention to achieve pregnancy - normal sperm counts but LOW percent sperm motility |
|
|
Interventions for improving Fertility
|
• Vibroejaculation
• Electroejaculation • Direct Semen Retrieval • Assisted Reproduction: – in-home insemination – intra-uterine insemination – in-vitro fertilsation (IVF) – gamete intrafallopian transfer (GIFT) – Intracytoplasmic sperm injection (ICSI) |
|
|
Integumentary- organ system that protects the body from various kinds of damage, such as loss of water or abrasion from outside. The system comprises the skin and its appendages
|
• 50-80% of persons with SCI develop a pressure ulcer
• Prevalence ~9% at 1yr vs 23-33% at 15-20yrs post-discharge • 2nd most frequent cause for rehospitalisation in USA & occupy 30% of non acute SCI hospital beds in NSW. • Significant morbidity and mortality. • Consider personal costs. |
|
|
Neurological Complications
|
• Pain & spasticity
• Late onset weakness or sensory loss (~20%) • Progressive cystic myelopathy (post-traumatic syringomyelia) • Compressive neuropathy – 2/3 in upper limbs – >50% carpal tunnel – 25% bilateral neuropathy |
|
|
Clinical Relevance of Spasticity
|
• Disabling if interferes with positioning or ADLs (eg. transferring, dressing, bathing, toileting, sitting balance, pushing wheelchair, gait, driving, etc)
• Exacerbated by noxious stimuli below lesion (eg infection, fracture, etc) • May be implicated in falls • May cause contractures, pain or skin breakdown |
|
|
Musculoskeletal Commilcations
|
• Heterotopic ossification
• Upper limb overuse syndromes – rotator cuff tears, tendonitis, subacromial bursitis, capsulitis – shoulder pain – impact on function • Osteoporosis & increased risk of lower limb fractures (6%) • Kyphoscoliosis • Neck & back pain |
|
|
Cardiovascular
|
• Acute phases – inc risk of arrhythmias
• Prone to postural hypotension, pedal oedema • Later phases - Hypertension 2x as common • Increased rate (22% vs 6%) & earlier onset of diabetes mellitus • 2nd leading cause of death (50% deaths >30 yrs post SCI) |
|
|
Pulmonary
|
• Restrictive disease
– muscle paralysis – kyphoscoliosis, spasticity • Obstructive disease – hyperactive airway disease • Recurrent respiratory tract infections • Respiratory failure • DVTs & PEs • OSA (40%) – only 25% are obese |
|
|
Psychosocial Risk Factors for SCI
|
- fewer years of education
- more likely to be unemployed - more likely to be single OUTCOME: younger people are more tolerant and less likely to become depressed |
|
|
Community Reintegration
|
75% return home
However, often face barriers (physical, attitudinal, expertise, systemic) For e.g. attendant care, assistive devices, equipment and financial support, accessible transportation, employment opportunities, and primary health care services Employment rate 40% (70% in the general population) Reduction in involvement in active living Impact on relationships (Postinjury marriages survive better than preinjury marriages) |
|
|
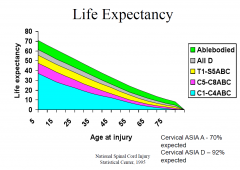
Life Expectancy
|
|
|
|
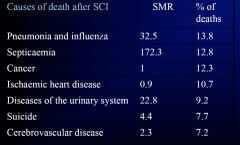
Causes of death after SCI
|
|
|
|
Prevention of SCI
|
• Primary – stopping it from happening
– Seat belts, child safety seats, Safer roads & cars – Random breath testing, legislation – Helmut use, diving education, workplace safety – Falls prevention measures and education • Secondary – reducing severity, managing risk factors – Improved retrieval, specialised care, early decompression • Tertiary – mitigating the effects – Rehabilitation programs – Education and self management re: health maintenance (regular check ups, nutrition, exercise, pressure area care |
|
|
ASIA
-a, b, c, d,e |
A indicates a "complete" spinal cord injury where no motor or sensory function is preserved in the sacral segments S4-S5.
B indicates an "incomplete" spinal cord injury where sensory but not motor function is preserved below the neurological level and includes the sacral segments S4-S5. This is typically a transient phase and if the person recovers any motor function below the neurological level, that person essentially becomes a motor incomplete, i.e. ASIA C or D. C indicates an "incomplete" spinal cord injury where motor function is preserved below the neurological level and more than half of key muscles below the neurological level have a muscle grade of less than 3, which indicates active movement with full range of motion against gravity. D indicates an "incomplete" spinal cord injury where motor function is preserved below the neurological level and at least half of the key muscles below the neurological level have a muscle grade of 3 or more. E indicates "normal" where motor and sensory scores are normal. Note that it is possible to have spinal cord injury and neurological deficits with completely normal motor and sensory scores.[4] |