Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
36 Cards in this Set
- Front
- Back
|
dyspnea during pregnancy is common however
|
pregnant women with acute or unexlained sob deserve eval for a PE
|
|
|
pregnant women imaging
|
CXR while shielding abdomen, V/Q scan as opposed to CT also a half dose perfusion scan without ventilation can be done
|
|
|
functional test that can provide tremendous info about the patients resp status
|
ambulation
|
|
|
a patient fails a breif trial of NIPPV...
|
the physician should be prepared for intubation
|
|
|
in severe asthma or status what else is given
|
mag epi or heliox can also be tried
|
|
|
high doses of CS are used initially for
|
moderate to severe asthma exacerbations
|
|
|
in the setting of acute pulmonary edema...
|
100% O2 must be provided often under positive pressure the patient is maintained in the upright position with legs dangling if possible to assist fluid redistribution from the lungs
|
|
|
IV loop dieuretics are used in acute pulmonary edema because
|
not only diurese but cause increased venous capacitance with the usual starting dose of furosemide being 20-80mg IV...sublingual NG also causes redistribution and can be administered
|
|
|
patients requiring nitrodrip because of high BP require what
|
art line
|
|
|
may be of limited benefit in patients presenting with acute pulmonary edema
|
refers to Beta blockers as there is often mild to moderate bronchospasm
|
|
|
no definitive role in acute management of CHF
|
dig
|
|
|
if absolutely needed in the setting of CHF what beta blocker should be used
|
often reserved for Diastolic dysfxn choose esmolol (short acting)
|
|
|
usually the only therapy for patients on dialysis and chronic renal failure
|
emergent dialysis
|
|
|
standard anticoagulation therpy for PE
|
heparin and warfarin
|
|
|
If anaphyulaxis or allergic rxn suspected give
|
(aerosolized, SC or IV) epi, IV benadryl, IV CS and IV H2 blockers
|
|
|
dyspnea occurs in 75% of pregnant women by when
|
30th week 2/2 higher diaphragm, blood redistribution and progesterone causing increased CO2 sensitivity...the physiologic dyspnea of pregnany rarely increases in severity in the final weeks
|
|
|
life threatening causes of dyspnea in the pregnant patient are
|
preeclampsia and PE
|
|
|
which dyspnea patients need to be admitted
|
patients requiring supplemental O2 to maintain Oxygenation and those with distress...also recommended in in someone with unstable angina having dyspnea even if they respond to therapy in the ED
|
|
|
normal A-a gradient
|
2-10 but this increases with age and may be as high as 30 in elderly
|
|
|
A-a gradient calculated by
|
(713)FiO2- PaCO2/0.8
|
|
|
causes of an A-a gradient
|
1. V/Q Mismatch (ex: PNA, CHF, ARDS, atelectasis, etc)
2. Shunt (ex: PFO, ASD, PE, pulmonary AVMs) 3. Alveolar Hypoventilation (ex: interstitial lung dz, environmental lung dz, PCP PNA) |
|
|
best CXR for dyspnic
|
PA and Lateral however a portable AP is often necessary at bedside
|
|
|
CXR worrisome for PE
|
a normal one in the setting of Hypoxemia
|
|
|
incongruity
|
lack of harmony; absurdity; incompatible; inconsistent
|
|
|
incidence of a silent MI is approximately
|
20%
|
|
|
calssic PE finding on ECG
|
S1Q3T3
|
|
|
dirge
|
to lament with music; a slow, solemn, and mournful piece of music
|
|
|
ECG of PE
|
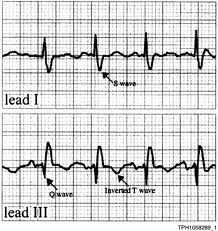
S1Q3T3
|
|
|
the VQ scan is reserved for what patients
|
renal insufficiency
contrast allergies and pregnant patients |
|
|
chemoreseptors for respiration
|
aortic and carotid bodies
|
|
|
one of the earliest findings in people with diaphragmatic weakness from neuromuscular D/Os
|
orthopnea
|
|
|
dyspnea associated with unilateral recumbant position may opccur in patients with unilateral dz, ball-valve airway obstruction diaphragmatic paralysis or COPD
|
trpopnea
|
|
|
diaphragmatic paralysis from injury to what levels
|
C3-5
|
|
|
a patient that can speak in few words has
|
moderate RD
|
|
|
suggstive of hypercarbnia
|
somnolence
|
|
|
jugular venous distention on inspiration is referred to as
|
cussmall's sign
|