![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
30 Cards in this Set
- Front
- Back
|
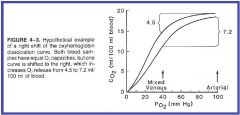
What is P50? |
The index of hemoglobin's affinity for oxygen. or the PO2 required to produce a saturation if 50%. For conditions of normal systemic arterial blood (37 C, PCO2 40 mmHg, pH 7.4) the P50 is about 27mmHg. |
|
|
What is a left or right shift in the Oxyhemoglobin Dissociation Curve? |
A right shift indicates a decreased affinity of hemoglobin to oxygen requiring a higher PO2 to achieve P50. (Normal at the tissues) A left shift indicates an increased affinity of hemoglobin to oxygen requiring a lower PO2 to achieve P50. (Normal in the Lungs) |
|

|
|
|
|
What is the Bohr Effect? |
When elevated CO2 and or H+ decreases Oxy-Hemoglobin Affinity. |
|
|
What conditions can cause a left shift? |
Decreased PCO2 Decreased H+ Decreased Temperature Increased pH Carbon Monoxide |
|
|
What conditions can cause a Right Shift? |
Increased PCO2 Increased H+ Increased Temperature Increased 2,3 Diphosphorgycerate (2,3DPG) |
|
|
What factors can lead to an increase in 2,3 Diphosphoglycerate? |
Increase in Epinephrine, Growth Hormone, & Thyroid Hormone
Alkalosis
Chronic Tissue Hypoxia
Blood stored in a blood bank for as little as 1 Wk has a decrease in 2,3 DPG |
|
|
How is Hb F different than Hb A? |
Molecular difference in structure between Hb Fetal & Hb Adult causes a change in the Oxy-hemoglobin dissociation curve shifting it to the Left (Higher affinity). |
|
|
What is formed when Carbon Monoxide binds with Hemoglobin? What affect does it have on PO2? Does it have an effect on respiration rate? |
It forms carboxyhemoglobin (has 240 times affinity).
It has no effect on PO2 as that is determine by O2 dissolved in the blood.
No, Chemoreceptors in the blood monitor PO2 not total O2 concentrations. |
|
|
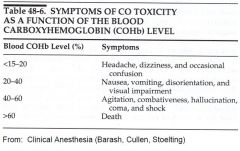
What are the symptoms of Carbon Monoxide poisoning and the corresponding levels? |
|
|
|
How is CO2 transported in the plasma at the tissues? (4 ways and percentages) |
10% is dissolve in the plasma as CO2. 70% In Hb metabolized with H2O to into HCO3 and H+ then diffuses out of Hb into plasma Cl- shifts into Hb cell. 20% reversibly bound to Hb as Carbaminohemoglobin. Small amt dissolve in Plasma converts to HCO3 |
|
|
What happens to the CO2 when Blood reaches Pulmonary Capillaries? |
All processes are reversed caused by PCO2 gradients. |
|
|
How is the CO2 disassociation curve different than the O2 disassociation curve? |
CO2 disassociation curve is almost linear.
|
|
|
What is the Haldane Effect? |
The more desaturated the hemoglobin is of oxygen the better able is that blood to carry CO2. |
|
|
What is a normal V/Q ratio |
4:5 or 0.8 |
|
|
How are PO2 and PCO2 related through alveolar ventilation? |
Inversely |
|
|
How is Hyperventilation defined? How is Hypoventilation defined? |
PACO2< 40 mmHg Increasing V/Q ratio produces Higher PAO2 and lower PACO2 PACO2>40 mmHg Decreasing V/Q ratio produces Lower PAO2 and Higher PACO2 |
|
|
What happens with High V/Q? |
Over-ventilation relative to the level of perfusion. PO2 increases (not sign-flat portion of curve) PCO2 decreases (sign-linear curve) pH increased |
|
|
What is physiologic dead space? |
Alveolar dead space+Anatomic dead space |
|
|
What happens with low V/Q? |
Area of the lung is under-ventilated relative to the amount of blood passing through the pulmonary capillaries. Decreased PO2 (potentially lg, curve dependent) Increased PCO2 (Large increase linear curve) Decreased pH Pulmonary Shunt (one type of) |
|
|
What are the two types of Pulmonary shunts? |
Anatomic-Portion of CO returns to heart without passing through pulmonary capillaries Intrapulmonary-Blood that passes through pulmonary capillaries without obtaining normal PO2 or PCO2. |
|
|
What are normal and abnormal sources of anatomic shunts? |
Normal-Veins in the heart that drain straight into the ventricles and some veins in the lungs. Abnormal-congenital defects Will not be corrected by increasing FIO2 |
|
|
What are the two types of intrapulmonary shunts? |
Shunt like-Low V/Q, alveoli with diffusion defect (increased diffusion distance)-unable to reach equilibrium due to not enough time(Increasing FIO2 would improve diffusion) Absolute-Blood passes around alveoli that have are not ventilated (absolutely no gas exchange) like fluid filled or atelectasis(increasing FIO2 would not help) |
|
|
|
|
|
Are the lungs dependent on nerves and hormones to optimize the V/Q ratio? |
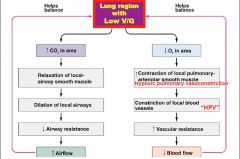
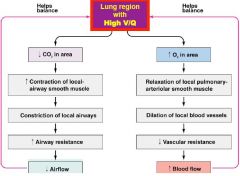
No-PCO2 and PO2 affect brochial and Vascular smooth muscles to affect V/Q ratio. |
|
|
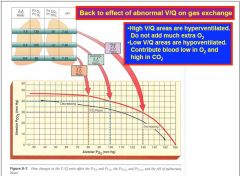
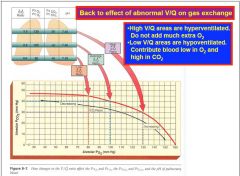
What happens in a lung region with Low V/Q? |
|
|
|
What happens in lung region with High V/Q? |
|
|
|
What causes regional differences in V/Q ratio in healthy upright adults at resting Cardiac Output, and how does it happen? |
Gravity Ventilation- Base better ventilated, Apex worse due to the effects of the compliance curve. Perfusion-Bases best perfused, Apex least perfused related to gravity effect on low pressure/low resistance circuit. Some of apex may not be perfused at all at rest. |
|
|
Does gravity have a greater effect on ventilation or perfusion? |
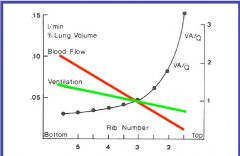
Affects Blood Flow Most |
|
|
Can regions of High V/Q compensate for regions of Low V/Q with respect to defending arterial O2 levels, what about CO2 levels? |
No- Not much extra O2 is picked up in High V/Q area related to the shape of disassociation curve. Maybe-If relatively equal volumes of blood from low and high V/Q areas & if the difference in PCO2 levels were equal. |