![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
149 Cards in this Set
- Front
- Back
|
Dalton's Law Calculation, Use |
Dalton's law determines the pressure of a mixed gas, which is the combination of the partial pressures of the individual mixed gases. PB = PN2 + PO2 + PH2O + PCO2 Mainly The partial pressures of these 2 gases make up the dominant portions of atmospheric pressure PN2 = (.79)( 760 - 47) = 563 mm Hg PO2 = (.21)(760 - .47) = 150 mm hg PN2 + PO2 = 713 (57 mm Hg rest) PCO2 = (0.004) (760-47) = |
|
|
What is PN2? |
PN2 = (.79)(760 - 47) |
|
|
What is PO2? |
PO2 = (.21) (760-47) |
|
|
What is PCO2? |
PCO2 = (.0004)(760-47) |
|
|
Percent composition gases |
N2 = 79% O2 = 21% CO2 = 0.04% |
|
|
Partial pressures at different altitudes, important values at each |
Sealevel to highest: Sealevel, Denver, Andes, Mt. Everest Pressure values (mm Hg) All same FIO2 = 0.21 Sealevel: PB = 760 PO2 = 160 Denver: PB = 640 mm Hg PO2 = 134 Andes: PB = 380 PO2 = 80 Mt. Everest: PB = 253 PO2 = 53 |
|
|
Diffusion of gas formula |
Use Fick's law: J = PAC/(thickness) V gas (flow) = (A)(D (solubility/ molecular weight))(delta P)/(T x MW ) Vgas = volume of gas diffusing per minute A = surface area D = Diffusion coefficient (incorporates solubility, molecular weight) : D = (solubility) / (MW^0.5) delta P = change pressure T = membrane thickness |
|
|
Difference in diffusion between CO2, O2. Significance. |
Diffusion coefficient CO2 20 X > than that of O2 Thus, far more soluble |
|
|
Partial pressure of gas in ambient air calculation PP O2 in ambient air |
Pgas = (Fgas) (P atm) P gas = partial pressure gas Fgas = concentration gas Patm = atmospheric pressure = 760 mm hg P gas = (0.21) (760 mm hg) = |
|
|
Partial pressure of gas in inspired gas |
PIg = (F gas) (P atm - P H2O (47)) PIg = partial pressure of inspired air F = f gas (O2 = .21, N2 = .79, CO2 = 0.004) Patm = 760 PH2O = partial pressure water vapor = 47 (not used in ambient air, only inspired air calculation) |
|
|
Gas values (venous and arterial blood, alveolus), significance |
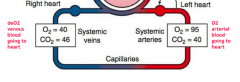
Arterial blood (o2 blood going to heart): PO2 = 95 mm hg PCO2 = 40 mm hg Alveolus: PO2 = 100 mm hg PCO2 = 40 mm hg Venous blood (de o2 blood going to heart):PO2 = 40 mm hg PCO2 = 46 mm hg |
|
|
Compositions CO2 in blood |
CO2 concentrations: CO2 dissolved plasma = 10% HCO3 in plasma and RBC = 60% carbamino protein: 30% |
|
|
What is the best to measure gas diffusion in lungs? |
Carbon monoxide |
|
|
What does the pulmonary wedge measure? a. RA pressure b. RV pressure c. LA pressure d. LV pressure |
LA pressure (choice c). Pulmonary wedge pressure is an indirect measurement of Left atrial pressure. |
|
|
What is an indirect measure of left atrium pressure. |
Pulmonary wedge pressure |
|
|
Where is o2 on (percents, locations) |
Dissolve in plasm (0.03%), producing 100 mm Hg Attached to HB as Hb-O2 (99.7%) |
|
|
Normal PaO2 VALUES |
85-95 mm Hg |
|
|
Normal PaCO2 values |
35-48 mm Hg |
|
|
Why does blood not go through the body equally? |
Gravity |
|
|
Normal V/Q |
0.8 (perfect) V = 4 L /min Normal Q = 5 L / min V/Q = 4L/MIN/5L/MIN = |
|
|
Low 0.8, significance, situations |
V/Q, Low ventilation high perfusion Reason: Obstruction Situations: (i.e: chronic bronchitis, asthma, acute pulmonary edema) |
|
|
High 0.8, significance, situations |
V/Q, High ventilation, low perfusion Reason: Unable to oxygenate blood: Situations:COPD |
|
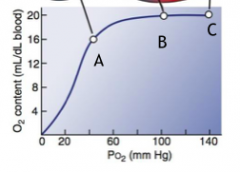
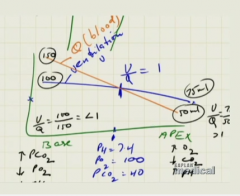
What does A, B, C represent? What are the certain values attributes to them and examples of each? |
A = V/Q : 1/10 explanation: Low ventilation, high perfusion Situations: Obstructions in ventilation (i.e: Chronic bronchitis, asthma ) B = V/Q : 10/10 Explanation: Normal C = V/Q : 10/1 Explanation: High ventialtion, low perfusion Situations: Obstruction in perfusion (i.e: COPD) |
|
|
Impact of in increased CO on pulmonary resistance. a. increased b. decreased c. no change |
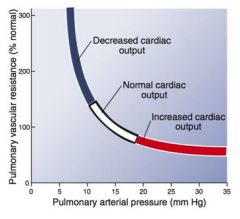
b. Decreased pulmonary resistance |
|
|
Impact of decreased CO on pulmonary resistance a. increased b. decreased c. no change |
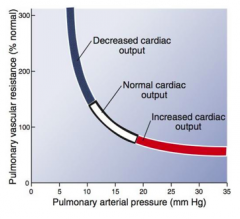
a. increased pulmonary resistance |
|
|
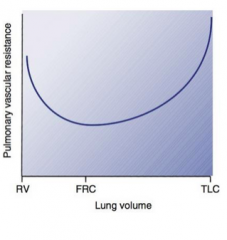
At what point do you have the optimal resistance related to lung volume? a. RV b. fRC c. TLC |
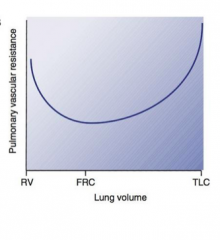
b. FRC is when you have optimal resistance related to lung volume |
|
|
Effect generalized hypoxia. Result, mechanism |
Pulmonary hypertension (eventually right ventricular hypertrophy due to RV having to pump harder due to persistent pulmonary hypertension) Reason: Persistant vasoconstriction and vascular smooth muscle remodeling. Mechanism: More hypoxia > more hypoxia > more.. viscous cycle But with generalized hypoxia. not good. |
|
|
Structure and function right ventricle emphasis. |
Right ventricle pumps same amount of blood at LV but right ventricle has lower systolic pressure (15-25 mm Hg) vs left ventricle systolic pressure (100-140), because not pumping to entire system Result: lower pressure, lower ventricle |
|
|
Properties contributing to high diffusion between capillaries |
Thin sheet (Fick's) High surface area CO2, O2 (hydrophobic) |
|
|
What proteins produces osmotic force due to plasma protein ? |
Albumin |
|
|
What pressure changes (starling) |
Hydrostatic pressure (13 > 6 from arterial to venous) P out on arteriole = 2-4 mm hg P in arteriole = -3 - 5 mm hg |
|
|
What pressure remains the same (starling) |
Interstitial colloid osmotic at 17
|
|
|
What does pulmonary wedge pressure? |
Indirect measure of left atrial pressure |
|
|
What is the indirect measure of left atrial pressure |
Pulmonary wedge pressure |
|
|
Change in blood flow lungs with gravity |
Highest blood flow at base Lowest blood flow at apex |
|
|
What point is there optimal ventilation perfusion on the lungs |
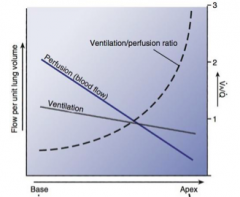
Somewhere in the middle, V/Q = 1, where the ventilation perfusion ratio = 1. |
|
|
Local low VA/Q meaning (values) |
PA O2 < Normal (102 mm hg) PA CO2 > Normal (40 mm hg) |
|
|
Local high VA/Q |
PA O2 > Normal (102 mm Hg) PA CO2 < Normal (40 mm Hg) |
|
|
62 year out female exhausted. Can not catch breath. BP = 90/60 HR = 110. RR = 25 b/min. Explanation. |
|
|
|
What happens when O2 decreases to bv? Result mechanism. |
Result: When O2 < 70% normal (< 73 mm Hg PO2), adjacent bv constrict. Mechanism: Blood diverted away from poorly ventilated regions, pulmonary circulation maximizes ventilation and perfusion |
|
|
Effect of generalized hypoxia. |
Pulmonary hypertension Persistent vasoconstriction > vascular smooth muscle remodeling. |
|
|
What does generalized hypoxia result? |
Pulmonary hypertension Persistent vasoconstriction, vascular smooth muscle remodeling. Right ventricular hypertrophy |
|
|
In the lungs, what is the changes in starling forces? Same force Different force |
Arteriole side: 2-4 mm hg towards interstitial fluid Pc = 13 Pi i = 17 Venous side: -3 - -5 mm hg towards capillaries Pc = 6 Pi i = 17 Same: Pi i = 17 mm hg Cahnge: Arterial Pc = 13, Venous Pc = 6 mm hg |
|
|
Hydrostatic capillary pressure = 10. What happening, possible effects? |
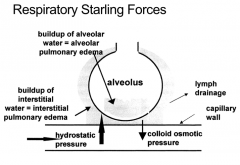
Pc > normal (2-4 mm hg) Resulting in more pressure: > More fluid going from capillaries to interstitial water (interstitial pulmonary edema) > More fluid going from capillaries to edema (alveolar pulmonary edema) |
|
|
Situation |
Heart: Lungs: Possibilities: obstruction, reducing blood flow Left ventricular heart failure Left side heart failure (resulting in pulmonary edema) |
|
|
Effect of let ventricular heart failure |
Pulmonary edema S&S: tired (no o2 coming in) S O2 : Very low |
|
|
1. What is the pulmonary CO? a. 1L/MIN b. 2l/min c. 3l/min d. 4/lmin e. 5/l min f. 6l/min 2. Is the pulmonary CO a. greater than b. less than c. equal to Systemic CO? |
1. Pulmonary CO = 5 L /min 2. Pulmonary CO = Systemic CO = 5 L / min |
|
|
1. A certain vessel oscillations from 4-25 mm hg during systole. What is it? 2. Oscillations from 8-25 3. Oscillations from 75-120 a. Aorta b. RA c. RV d. pulmonary artery e. pulmonary vein |
1. Right ventricle: 4-25 2. Pulmonary artery: 8-25 3. Aorta: 75-120 |
|
|
60 year old male patient |
Sleep apnea |
|
|
What creates pulmonary arterial pressure? |
Right ventricle. |
|
|
Diff. RV, LV |
RV has lower vascular resistance |
|
|
Hypoxia result |
Shunt blood away fom damaged alveolir sacs. Cause pulmonary hypertension as a result of general hypoxia |
|
|
Effect of gravity on blood flow to lungs |
Creates zones of perfusion. |
|
|
V/Q matching leading to areas to different levels of perfusion and ventilation |
. |
|
|
Result low resistance |
Low pressure in pulmonary capillaries retaining low pressures to avoid pulmonary |
|
|
Gravity |
Good perfusion base lungs Low perfusion apex lungs |
|
|
Result obstructive sleep apnea |
Long bouts of apnea, this can cause intermittent hypoxia in the lungs, which cause vasoconstriction, pulmonary hypertension > right ventricular hypertrophy (edema) |
|
|
What does increase non CO2 producing gas stimulate? |
Only peripheral chemoreceptors stimulated since no CO2 stimulated |
|
|
What does increasing CO2 producing gas stimulate? Result, mechanism |
CO2 stimulates central and peripheral chemoreceptors > stimulation o medullary inspiratory neurons > increased ventilation |
|
|
Deep sea diving. what contributes blackout? |
Hyperventilation that you drop CO2 And when swimming drop O2 quickly that you black out before CO2 can increase |
|
|
What changes during breathing? |
Oscillation arterial O2 saturation (87-80) Tidal air movement not oscillation all the time, oscillation except during apnea |
|
|
What happens with CO2? Result mechanism |
CO2 goes to capillaries Diffuse into CSF and stimulate chemoreceptors to stimulate ventilation. |
|
|
What is the more powerful driver of respiration? |
CO2 |
|
|
Phases respiraiton |
2 phases: Slow, fast |
|
|
How does inspiration result? |
Turn of inhibitory isinglass allowing diaphragm contraction |
|
|
Sleep what is it |
erratic breathing |
|
|
What stimulates breathing: |
Alveolar PO2: < 60 Slight change CO2 |
|
|
What is the unloading phase of oxyhemoglobin equilibrium curve? |
in the venous blood system when PaO2 drops < 60 |
|
|
What is the loading phase of oxyhemoglobin equilibrium curve |
in the arterial blood when Po2 around 100-60 |
|
|
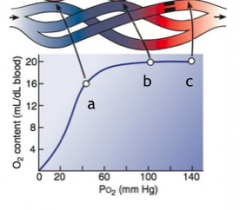
What are the main points of the oxyhemoglobin equilibrium curve? |
Arterial: 100% o2 sat (100 mm Hg) Venous: 75% O2 sat (40 mm Hg) |
|
|
When is there shifts in the Hb - o2 dissociation curve? |

Left shift (higher O2 affinity with Hb): Right shift (lower O2 affinity with Hb): Increase CO2, H+ (decreased pH), temperature, 2,3BPG Exercise. |
|
|
Person exercise. What happens to o2 dissociation curve? |
right shift (b/c increase CO2, H+, 2,3BPG) |
|
|
How can the lung's ability to transfer gases be measured? |
Diffusing capacity = V gas (gas flow)/ (P1-P2) Diffusion via conventional flux's formula not commonly used, b/c SA, membrane thickness, and diffusion coefficients are difficult to accurately measure in the lungs |
|
|
What partial pressure of what gas stays constant throughout the alveolar air, systemic arterial blood, and mixed venous blood? a. O2 b. CO2 c. H2O vapor d. N2 |
N2 (It stays constant at 571 mm Hg) throughout |
|
|
Use following choices to answer questions. a. Andes b. Mt. Everest c. Denver d. Sea level 1. Exclusing sea level, which of the following has the greatest PO2? 2. Which has the lowest PO2? 3. Exclusing sea level, what is the middle PO2? |
1. Denver at 134 mm Hg 2. Mt Everest at 53 mm Hg 3. Andes at 80 mm Hg |
|
|
What is the respiratory exchange ratio. |
The volume of o2 transferred to pulmonary circulation / the volume of co2 removed |
|
|
Which gas diffuses the fastest. Reason |
CO2 diffuses ~ 2 x faster Properties CO2: 20 x greater diffusion coefficient (solubility / (sq root MW)), Properties O2: 10 x greater partial pressure greater. |
|
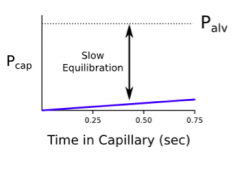
This is evidence of what? Reason? mechanism. |
Diffusion limited gas perfusion. Since molecule reaches equilibrium in solution slowly, diffusion is the limiting factor of transport across the membrane. |
|
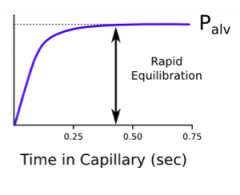
What is evidence of what? Reason? mechanism. |
Perfusion limited gas exchange The transfer of molecule into capillary can only be increased by increasing blood flow. |
|
|
By what percent is O2 carried in body? |
98% via Oxyhemoglobin > process: O2 + Hb > HbO2 2% dissolved in blood |
|
|
O2 saturation formula. Normal, significance. |
O2 saturation (SO2) = HbO2 content / (HbO2 capacity) x 100 Typically normal ~ 98% This is the ratio of oxygen actually bound to hb vs quantity that could be bound. |
|
|
What is the oxygen carrying capacity? Normal. What is it based on. |
The oxygen carrying capacity is the maximum amount of oxygen that can be carried by hemoglobin Value = 20 mL O2/dL Based on normal hb concentration of 15g hb/dL |
|
|
What is the o2 carrying capacity? a. 5 mL o2/dL b. 15 mL o2/dL c. 20 mL o2/dL d. 25 mL o2/Dl Significance |
O2 carrying capacity = 20 ml o2/dL (c) O2 carrying capacity is the max. amount of O2 that can be carried by Hg Based on a normal Hb concentration of 15 g Hb/dL blood |
|
|
Changes in P50. What are the changes and effect. |
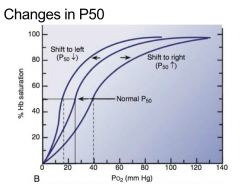
Left shift, P50 decrease Right shift, P50 increases |
|
|
What is the haldane effect? Diagram. |
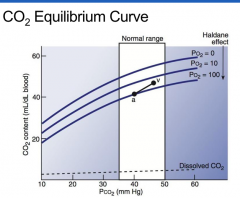
Haldane effect describes changes in CO2 content with increases in PO2. When PO2 increases, the CO2 content decreases (inverse relationship). But the normal range remains around 34-50 mm Hg |
|
|
There is a V = 0. Meaning? Examples? |
V = 0 ('Shunt') No air enters alveoli, unoxygenated blood continues in circulation Exampels: Pneumonia, atelectasis |
|
|
There is a Q = O. Meaning? examples? |
Q = O ('Dead space') No blood supply for lungs Ex: Pulmonary embolus |
|
|
High V/Q. Meaning, Labs , examples |
Ventilation exceeds perfusion. Labs: PAO2 > Normal, PA CO2 < Normal Unable to oxygenate blood (wasted ventilation Ex: COPD |
|
|
Low V/Q. Meaning, labs, examples |
Poor ventilation, lack O2 supply Labs: PAO2 < Normal, PA CO2 > Normal Ex: Chronic bronchiti, asthma, acute pulmonary edema (obstructions) |
|
What does a, b, c represent? Examples?. Also include d. V = 0, e. Q = 0 |
a: V/Q = 1/10 Perfusion exceeds ventilation Ex: Obstructions (asthma, chronic bronchitis, pulmonary edema) b: V/Q = 10/10 Normal c: V/Q = 10/1 Ventilation exceeds perfusion (wasted ventilation) Ex: COPD D: Shunt. No ventilation at all. Ex: Atelectasis, Pneumonia E: Dead space Ex: Pulmonary embolism |
|
|
Inspired gas, expired O2, CO2 values |
Inspired gas: O2 = 160 CO2 = 0.3 Expired gas: O2 = 116 CO2 = 32 |
|
|
What pumps Cl- into RBC and HCO3 out into plasma? |
Chloride shift |
|
|
Normal CO2 levels: hypo, hypercapnia |
35-48 Hypocapnia: < 35 Hypercapnia: 48 |
|
|
Hypoxemia |
PaO2 < 85 |
|
|
Normal pH, acidosis, alkalosis |
7.35-7.45 Acidosis: < 7.35 Alkalosis: > 7.45 |
|
|
What does pulmonary embolus cause? |
Dead space Q= 0 |
|
|
wHAT DOES PNEUMONIA, ATelctasis cause? |
V = O Shunt |
|
|
What does COPD cause? |
Ventialtion exceeds perfusion. V/P = 10/1 |
|
|
What does chronic bronchitis, asthma cause? |
Perfusion > ventilation V/P = 1/10 |
|
|
Difference between pulmonary and systemic blood flow |
Pulmonary bf = systemic bf = 5 L |
|
|
Differences pressures? (oscillation graph) Pulmonary artery pressure |
Right ventricular pressure oscillation: 3-25 mm Hg Pulmonary artery pressure oscillations: 8-25 Pulmonary capillaries = 8 Left atrium = 4 Aortic pressure oscillations: 75-120 Pulmonary artery pressure: 8-25 Pulmonary capillaries = 8 Left atrium 2 |
|
|
A certain vessel alternates between 3 and 25 mm Hg. What is it? |
Right ventricle |
|
|
A certain vessel alternates between 8 and 25 mm Hg. What is it? |
Pulmonary artery |
|
|
A certain vessel alternates between 75 and 120 mm Hg. What is it? |
Aorta |
|
|
Changes of CO on resistance of lungs? |
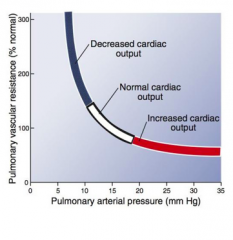
As CO increases, resistance decreases by opening more capillaries (branching/RECRUITMENT ) |
|
|
How does the higher region of lungs compare to lower? |
Low perfusion pressure Capillaries usually closed |
|
|
What does the pulmonary wedge pressure for? |
Indirect measurement of left atrial pressure. |
|
|
What is used for left atrial pressure measurement? |
Pulmonary wedge pressure
|
|
|
Pulmonary pressures. What are they. |
Pulmonary artery: 8-25 Pulmonary capillaries: 8 Left atrium: 3 |
|
|
Which of the following best corresponds to the pulmonary wedge pressure? |
The left atrial pressure at 3 mm Hg |
|
|
When is the pulmonary vascular resistance the lowest? a. At RV b. At FRC d. At TLC |
At the FRC |
|
|
What does the lung volume vs resistance graph look like? |
|
|
|
Effect of hypoxia Physiological. Pathological Result, mechanism |
Physiological: Below 70% normal o2 (below 73 mm hg PO20, adjacent blood vessels. Reason: Divert blood away from Poorly ventilated regions and pulmonary circulation can maximize ventilation and person. Pathological (Generalized hypoxia): Result: Pulmonary hypertension Reason: Persistent vasoconstriction and vascular smooth muscle remodeling. Eventually the pulmonary hypertension ill cause right ventricular hypertrophy. |
|
|
Effect high filtration (high Pc, low Pi c) |
Edema
2 types: interstitial pulmonary edema (buildup interstitial water) alveolar pulmonary edema (buildup alveolar water) |
|
|
Arterial and venous pressures and net pressures. in pulmonary capillaries |
Arterial end: Pc = 13 Pi i = 17 net = 2-4 mm hg Venous end: Pc = 6 Pi i = 17 net = -3 - -5 |
|
|
What pressure remains constant in pulmonary capillairies? |
Colloid osmotic interstitial pressure at 17 |
|
|
Pulmonary arterial pressure is created by what? What is the pressure? |
Right ventricle PA pressure = 3-25 mm hg |
|
|
Respiratory groups of medulla, their innervations What stimulates them? |
Dorsal respiratory group (DRG): inspiratory muscles = External intercostals, diaphragm Ventral respiratory group (VRG): expiratory muscles = Internal intercostals, accessory respiratory muscles Stimulation of DRG, VRG: Pontine respiratory group (PRG): Pneumotaxic center Apneustic center |
|
|
Expiratory phases |
2nd phase: Essentially silent and caused by changes in passive recoil of lung |
|
|
Below questions will use these choices: a. Pulmonary stretch receptors b.Irritant receptors c. J receptors 1. What receptor is rapidly adapting? 2. What receptor is slowly adapting 3. What receptor results in rapid shallow breathing and cardiovascular depression? |
1. Irritant receptors These irritant receptors are rapid adapting receptors in the sensory terminals of myelinated afferent fibers that respond to noxious stimuli such as dust, smoke or touch. 2. Pulmonary stretch receptors These are slowly adapting stretch receptors that lead to excitation of the inspiration blocking switch. 3. J receptors (juxtapulmonary capillary receptors) Stimulated by lung injury, large inflation, acute pulmonary vascular congestion, chemicals. Stimulate rapid shallow breathing, bronchoconstriction, cardiovascular depression . |
|
|
Effects of gases on driving respiration. |
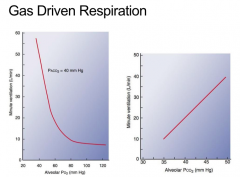
O2: Increase when start decline below 80 and greatest drive when below 60 CO2: Change to slight changes. |
|
|
How would one compare and contrast the O2 and CO2 dissociation curves. |
The concentrations released are similar but pressure differences different Change gas concentration ~ 5 Pressure change O2: 95 > 40 mm Hg Pressure change CO2: 40 > 47 mm Hg |
|
|
What happens to PO2 of blood as it travels away from pulmonary capillaries towards the systemic circulation. Result, mechanism. |
O2: Drops 100 mm Hg to 95 mm Hg Rationale: O2 rich blood mixed with venous blood that was distributed to the conducting passageways rather than to the alveoli. CO2: Constant 40 mm hg |
|
|
Sensing receptors respiratory, function, method, locations |
Central chemoreceptors: CO2 monitor (main) Location: Brain medulla Mechanism: Only CO2(not H+) from Systemic arterial blood diffuse across blood brain barrier, H+ produced and stimulate H+. Peripheral chemoreceptors: Via: O2 monitor (main), CO2 (assistant role) Location: Carotid, Aortic arches |
|
|
Patient given 21% O2 air. Result, what receptors controlling ventilation |
No change ventilation and central receptors, b/c same O2. |
|
|
Patient given 100% O2 air. Result, what receptors controlling ventilation. |
No change respiration and central receptors sense , b/c central chemoreceptors respond only to changes in CO2. Thus no change in ventilation. |
|
|
Patient transferred to a room providing 5% CO2 10% O2. Result, rationale. |
Ventilation increased, controlled by peripheral receptors Rationale: Peripheral chemoreceptors take over despite CO2 via chemoreceptors with excessive fall O2 (21% > 10% O2) |
|
|
What are the response of ventilation to controlled changes of PO2 and PCO2? Significance. |
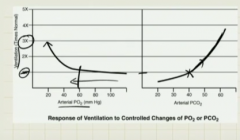
PCO2, increase 10 mm Hg from 40 > 50 (Ventilation 2X) PO2, decrease below 60 mm Hg, (Ventilation 2X) Significance: A slight increase in PCO2 (40 normal > 50 mm hg) vs large decline PO2 (100-80 normal, below 60 (very low)) will drive ventilation. Thus, PCO2 changes are more prone to cause ventilation increase (CO2 change via central chemoreceptor are the prime drivers ventilation) |
|
|
Under normal circumstances, what is the driver for ventilation. |
Central chemoreceptors (PaCO2, H+) |
|
|
Patient has following lab values, PaCO2 = 70 mm Hg, PaO2 = 55 mm Hg. What is true? |
PaO2 is the driving force for ventilation (via peripheral chemoreceptors) |
|
|
What is the site for inherent rhythm for respiration. Result site. |
Medulla oblongata Result: 12-20 RR Expiration > inspiration |
|
|
Components total OT in body |
Dissolve O2 (PaO2: 80-100): Patm fO2 (normally: .21 = 21%) Hb: Hb concentration (12-15 g/dL) Hb saturation (97%+, less 92% dangerous) |
|
|
Going to Denver, Ansen, Mt. Everest. Result, mechanism |
Going to high altitude areas with Lower Patm O2 = Patm, FO2 (fO2) Result lower Patm (Vmin = Patm x FiO2) Reduced Vmin, reduced Valv, reduced O2. Process Peripheral chemoreceptors take over ventilation the reduced O2 and hyperventilation occurs (Hyperventilation driven by peripheral chemoreceptors) Result: PaO2 decreases, PaCO2 decreases (via ventilation) pH increases (respiratory alkalosis), Hb saturation (decreases), Hb same, Overall O2 decreases (via PaO2 decrease, Hb saturation decreases) |
|
|
Acclimatization to Denver, Ansen, Mt. Everest. |
Process: Patm decreased > PO2 decreased Continued PO2 still low, thus peripheral chemoreceptors take over However, Hg saturation decrease remains as Hg releases O2 in response to low PaO2 Result: Continued hyperventilation driven by peripheral receptors and kidneys reduce HCO3- reabsorption from DCT, PCT to balance pH Hb: Increase Hb concentration (physiological polycythemia) : via erythropoetin secreted by kidneys Continued low O2 saturation Labs: Normal pH, Low PaO2, Low PaCO2 (via hyperventilation), Increased Hb + Rbcs (Physiological Polycythemia), Low O2 saturation |
|
|
Patient is in denver. Labs are shown: PaO2 (55 mm Hg), RBC elevated, hyperventilation. What to do? a. Administer O2 b. Administer erythropoetin c. Encourage patient to breathe deeply d. Continue monitoring patient. |
Patient is in an elevated altitude with low O2. Normally body's peripheral chemoreceptors will take over to manage the low O2, resulting in hyperventilation to acquire more O2. This hyperventilation will cause respiratory alkalosis, however body compensates to remove HCO3- to restore pH. Also, RBC will increase over time (physiological polycythemia) to compensate lower O2. Thus, patient is in a naturally acclimatized position and nothing should be done. Choice c. continue monitoring patient. |
|
|
Change in acclimization |
Total O2 same (B/c although low PaO2, Hb increased) Continued low PaO2, low PaCO2, low O2 saturation Change increased: Hb (polycythemia) |
|
|
Rank gases in order of solubility.
Significance. |
CO >> CO2 >>> O2 As a result, CO is the best indicated to measure diffusing capacity of lungs. |
|
|
Which of the following gases is best indicated to measure the diffusing capacity of the lungs? a. CO b. CO2 c. O2 d. N2 e. H2O f. He |
CO > CO2 > O2 Since CO highest soubility, this is best indicated to measure diffusing capacity of the lung. |
|
|
Effect of Hb on O2 content at different PO2. |
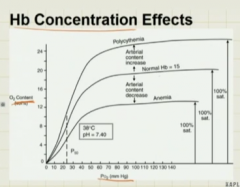
Left shift: increase rbc (hg) (increase arterial O2, no change Hb saturation) Right shift: decrease rbc (hg) (decreased arterial O2, no change hb saturation) |
|
|
Effect change # hb (RBC). |
Increase O2, no change Hb saturation at different PO2 b/c carrying more O2 in more Hb (rBC) |
|
|
Effect CO on carrying capacity O2. |
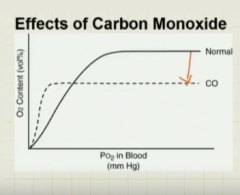
Mechanism: Since CO >> solubility than O2, diffuses to and attaches faster to hb (displacing O2). Result: Decreased as CO displaces O2 from hb resulting. Lab: Normal Hb saturation (not sensitive for what, but no O2 saturation), but Total O2 decreased (bc less O2 containing hb) PaO2 normal |
|
|
Effect RBC disorders |
Anemia: PO2: normal Hb: reduced (b/c reduced RBC) Total O2: reduced Polycychemia: PO2: normal Hb: increased (b/c increased RBC) Total O2: increased CO poisoning: PO2: normal Hb: normal but saturated with CO (Pulse ox will show normal saturation, but less O2) Total O2: Decreased (b/c Hb less O2) |
|
|
Gas transport forms. |
O2: 99% Hb, 1% dissolved CO2: 70% HCO3- (Transported via HCO3-Cl- antiport, Cl- in, HCO3- out and vice versa) 10% Dissolved 20% Bound to Hb as Hb-CO2 (Carboxyhemoglobin) |
|
|
What are the 4 causes hypoxemia. |
1. V/Q mismatch 2. Diffusion impairment 3. Shunt 4. Hypoventilation |
|
|
What part lung gets more vent/perfu. |
Via gravity, base of lungs get more ventilation and perfusion |
|
|
Relatinoship between apex, base |
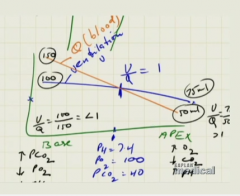
Apex is to O2 as base is to CO2 Base: High CO2 (Low pH) Low O2 V/Q < 1 Apex: High O2 Low CO2 (High pH) V/Q > 1 |
|
|
V and Q diagram of lungs. |
Q starts higher than V, but greater slope and drops below V after midpoint V starts lower, but smaller slope and above Q after midpoint |
|
|
Patient inhales peanut. What happens to lungs. Values, mechanism,rationale. |
Decreased ventilation (airway obstructed) V/Q < 1, towards base Values in base: PaO2 decreases (peripheral vasoconstriction, Q then decreases) PaCO2 decreases (ph decreases) V decreases, Q increases (V/Q < 1) |
|
|
Patient has pulmonary embolism. What happens to lungs. Values, mechanism, rationale. |
Decreased perfusion V/Q > 1 towards apex Values in apex: PaO2 increases (peripheal vasodilation, Q then increases) PaCO2 decreases (pH increases) Q low, V high (V/Q > 1) |