![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
13 Cards in this Set
- Front
- Back
|
Describe the entire renal physiology |

|
|
|
Describe countercurrent mechanism |

|
|
|
1) Where do angiotensin work on? 2) Where do aldosterone work on? 3) Where do ADH work on? |
1) - Afferent arteriole constriction < Efferent arteriole constriction, thus reducing but maintaining GFR - Increased sodium and water reabsorption in proximal tubule, and increased potassium secretion too - Trigger systemic vasoconstriction - Trigger release of ADH and aldosterone 2) - Act on DT's principal cells, by activating Na-K exchanger, thus increased sodium reabsorption - Upregulation of epithelial sodium channels (ENaCs) in the collecting duct and colon - Upregulation of H-K exchanger in DT's intercalated cells - Upregulation of NCC in DCT 3) - Upregulate aquaporins-2 channels in DCT and collecting tubules - Systemic vasoconstriction |
|
|
1) Where do thiazides work on 2) Where do loop diuretics work on 3) Where do osmotic diuretics work on 4) Where do potassium sparing diuretics work on? 5) Where do ACE-I work on? |
1) inhibit Na-Cl Co-transporter (NCC) in DCT 2) inhibit Na-K-Cl Co-transporter in LoH 3) throughout the renal tubule 4) inhibit K-H exchangers in the alpha intercalated cells of DCT 5) blocks angiotensin converter enzyme, produced by the lungs (*** ARB blocks angiotensin II receptors in the body) |
|
|
What are the causes of hyponatremia? |
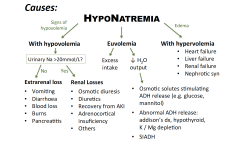
- Check serum osmolality - Check urine osmolality - Check creatinine/urea/potassium - Check volume status |
|
|
What are the causes of hypernatremia? |
1) Concentrated urine, low urine output: Consider loss of water/dehydration - burns/sweat - GI losses 2) Water loss into cells: - severe exercise - seizures 3) High urine output, dilute urine: - Central or Nephrogenic DI - Diuresis (hyperglycaemia, post AKI diuresis, post obstructive diuresis) |
|
|
What are the causes of hypokalemia? |
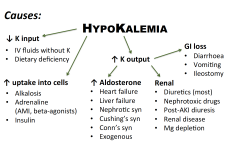
1. assess volume status 2. tro GI losses 3. tro urinary losses 4. increased entry into cells bloods to order: - renal panel, Ca, Mg, FBC, ABG |
|
|
What are the causes of hyperkalemia? |
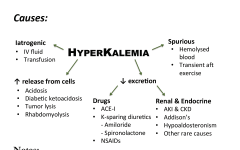
bloods to order: -Renal panel, Ca, Mg, Glucose, ABG, FBC, creatinine kinase (if myolysis suspected) |
|
|
How to differentiate between central and nephrogenic DI? |
Water deprivation test: 1) test urine osmolality after water deprivation for 4-18 hrs (normal >800) 2) test urine osmolality again after injection of desmopressin (central > 800, nephrogenic < 500) |
|
|
What is addison's disease |
Addison disease (or Addison's disease) is adrenocortical insufficiency due to the destruction or dysfunction of the entire adrenal cortex. It affects glucocorticoid and mineralocorticoid function. The onset of disease usually occurs when 90% or more of both adrenal cortices are dysfunctional or destroyed. |
|
|
What is conn's syndrome |
Primary hyperaldosteronism |
|
|
Differentials of high potassium, low sodium |
1) intracellular shift (low Na-K pump function) - Beta blockers - Low insulin levels 2) Endocrine - low aldosterone (Addison's, Panhypopituitarism) - low angiotensin |
|
|
Differentials of low potassium, high sodium |
1) Intracellular shift (high Na K pump function) - Beta agonists - High insulin levels 2) Endocrine - High aldosterone (RAA activation, paraneoplastic secretion, CAH, Conn's) - High angiotensin |