Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
30 Cards in this Set
- Front
- Back
|
What are the quantity and composition of body fluids dependent on?
|
- Input (food, fluids, etc)
- Metabolism - Output (urine) |
|
|
How much fluid is filtered through the glomeruli every day?
|
180 L
|
|
|
How much fluid flows through the kidneys every day?
|
1728 L
|
|
|
All but how much of the glomerular filtrate (180L) is reabsorbed per day?
|
1.2 L (excreted)
|
|
|
What is contained within the 1.2 L of daily excreted urine?
|
By-products of metabolism as well as excess electrolytes
|
|
|
What range of pH can the kidneys adjust the pH of urine within? Why?
|
pH: 4.5 - 8.0
Allows it to excrete either base or acid to maintain constant plasma pH in vicinity of 7.4 |
|
|
How can urine be used to determine disease states?
|
- Abnormal metabolism will lead to abnormal end products of metabolism in urine (eg, porphyria)
- Presence of glucose indicates blood glucose level exceeds threshold value for total reabsorption (indicates diabetes mellitus) - Protein in urine indicates glomerular disease |
|
|
What does the volume and osmolarity of urine tell us about a person?
|
Body's state of hydration
|
|
|
How does a severely restricted fluid intake affect the volume and osmolarity of urine?
|
- Very little urine output
- Concentration of electrolytes (Na+ and K+), and solutes will be relatively high |
|
|
What is the best index of dietary intake of Na+ and K+?
|
24 hour excretion of Na+ and K+, respectively
|
|
|
What happened in the renal experiment / dry lab?
|
- Each subject ingested 1.5% body weight of specific fluid in 30 min or they have been given a drug to increase urine output
- Subjects provided urine samples at hourly intervals for 3 consecutive hours |
|
|
How do you calculate Cosm (osmolar clearance)
|
Cosm = (urine flow rate * Uosm) / Posm
|
|
|
How do you calculate C_H2O?
|
C_H2O = urine flow rate - Cosm
Cosm = (urine flow rate * Uosm) / Posm |
|
|
What were the 7 treatment groups?
|
- Ingestion of 1L of water
- Ingestion of 1L of water + ADH administration - Ingestion of 300 mL beef broth - Ingestion of 1L of kool-aid made up in a 30 mM sodium bicarb sol'n - Ingestion of 1L of beer - Injection of 10 mg/kg furosemide (inhibits Na+ reabsorption in thick ascending loop) - Injection of Acetazolamide (carbonic acid inhibitor that inhibits Na+ reabsorption in PT) |
|
|
How do you calculate Urine Flow Rate?
|
UF = (Urine Volume) / (Time of Collection)
|
|
|
How do you calculate Clearance?
|
Cx = [Ux] * UF / [Px]
Cx = clearance of substance X [Ux] = urine concentration of substance X UF = urine flow rate = urine volume / time [Px] = plasma concentration of substance X |
|
|
How do you calculate the excretion rate of X?
|
Excretion Rate of X = [Ux] * UF
[Ux] = urine concentration of substance X UF = urine flow rate = urine volume / time |
|
|
What were the 7 treatment groups?
|
- Ingestion of 1L of water
- Ingestion of 1L of water + ADH administration - Ingestion of 300 mL beef broth - Ingestion of 1L of kool-aid made up in a 30 mM sodium bicarb sol'n - Ingestion of 1L of beer - Injection of 10 mg/kg furosemide (inhibits Na+ reabsorption in thick ascending loop) - Injection of Acetazolamide (carbonic acid inhibitor that inhibits Na+ reabsorption in PT) |
|
|
Which of the treatment groups can be distinguished based on having the highest pHs? Why?
|
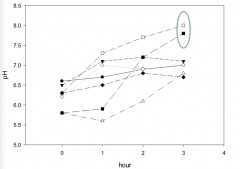
- Injection of Acetazolamide (carbonic acid inhibitor that inhibits Na+ reabsorption in PT)
- Ingestion of 1L of kool-aid made up in a 30 mM sodium bicarb sol'n (Both will have high pH) |
|
|
How are bicarb solution and Acetazolamide similar? How can you distinguish them?
|
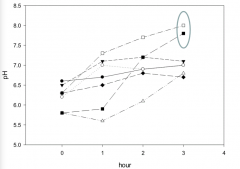
- Both have high pH by hour 3
- Distinguish based on free water clearance - Bicarb (open squares) will excrete more free water |
|
|
Which of the treatment groups will be the most different (very high urine flow, very high osmotic clearance, very high Na+ and K+ excretion)?
|

Furosemide (inhibits Na+ reabsorption in thick ascending loop) = black diamonds
|
|
|
Which of the treatment groups will have no changes for first couple of hours but then changes at 3rd time point? What kind of changes?
|

- Ingestion of 1L of water + ADH administration (open triangles)
- No urine flow, osmotic clearance, or free water clearance until hour 3 - ADH and H2O cancel each other out until ADH wears off between hours 2 and 3, then H2O has its effect - ADH has no effect on Na+ or K+ |
|
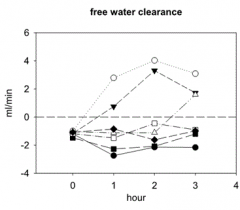
Which treatment groups stick out for having high free water clearance?
|
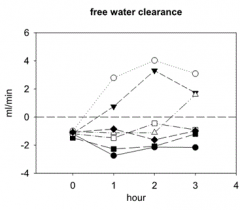
- 1 L water (free water)
- 1 L beer (basically free water + alcohol) |
|
|
How are 1L water and 1L beer similar? How can you distinguish them?
|

- Both have high free water clearance
- Beer will cause more excretion of urine and free water clearance d/t alcohol (open circle) - 1L water is by default the other high free water clearer (dark triangle) |
|
|
What treatment group remains and is determined by default
|

Beef Broth (dark circles)
|
|
|
A patient's plasma concentration of Na+ is 150 mM, GFR is 100 ml/min, urinary conc. of Na+ is 200 mM, and urine flow rate is 1.5 ml/min. Patient's fractional excretion of Na+ is what? What equation do you use?
|
Fractional excretion of Na+ = ([Una] * UF) / (GFR * [Pna])
= (200 mM * 1.5 ml/min) / (100 ml/min * 150 mM) 2% |
|
|
Adding a hypertonic solution to the systemic circulation cause what change in volume / osmolarity?
|
- ↑ Extracellular Fluid Volume
- ↓ Intracellular Fluid Volume - ↑ Extracellular and Intracellular Fluid Osmolarity |
|
|
As the tubular fluid moves from the beginning to the end of proximal tubule, how does the creatinine concentration change?
|
Increased conc.:
- Not reabsorbed - As fluid is reabsorbed along PT, creatinine conc. is concentrated |
|
|
Which mechanism most importantly contributes to the auto-regulation of GFR?
|
Tubularglomerular Feedback (senses changes in Na+ delivery to distal tubule (often d/t change in GFR) and sends signals to glomerulus to bring GFR back to normal
|
|
|
Stimulation of renal sympathetic nerves will do what?
|
Constricts renal vessels → ↓ GFR & stimulates tubular reabsorption of Na+ and H2O by increasing renin release (AngII, Aldosterone)
|