Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
122 Cards in this Set
- Front
- Back
|
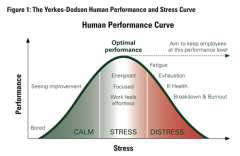
What is stress?
|
Negative emotional state in response to events seen as taxing or exceeding a person's ability to meet demands
|
|
|
Stressors
|
any type of event that triggers a stress response
|
|
|
Sources of Stress
|

Early stress research: any change that required you to adjust your behavior/lifestyle would cause stress
* Social Readjustment Rating Scale (SRRS)* |
|
|
Problems with the SRRS
|
-Link between SRRS and physical and psychological problems is weak
-Assumes life events have same impact on everyone -Assumes that change, whether good or bad, produces stress |
|
|
Sources of Stress: Daily Hassles
|
-Everyday minor events that annoy/upset people
-# of daily hassles is a better predictor of physical illness than number of major life events * Cumulative effect * Everything begins to pile on top of each other |
|
|
Daily Hassles - Gender Differences
|
-Women more likely to report daily stress associated with friends/family
-Men more likely to report school/work related stressors -Stress at work/school spills over into home l life * Women: spills into partner interactions * Men: more likely to withdraw |
|
|
Sources of Stress: Burnout
|
Condition caused by chronic, prolonged work stress
* Exhaustion: used up all of their emotional and physical resources * Cynicism: negative or overly detached attitudes * Failure/inadequacy: have a reduced sense of accomplishment or productivity |
|
|
Conditions that commonly produce burnout
|
-Overload: demands of job exceed ability to meet them
-Lack of control: the more control you have, the less stress you feel *Can be prevented when there is a sense of community in the workplace |
|
|
Sources of Stress: Traumatic Events
|
- Events/situations that are negative, severe and far beyond our normal expectations for life
-85% of people report experiencing traumatic events - When traumas are intense or repeated, some people may develop PTSD, though most are resilient |
|
|
Social Sources of Stress
|
-People who live under difficult or unpleasant conditions experience chronic stress
* People living under the poverty line, homeless * SES (Economic Status) is negatively correlated with chronic stress * Less privileged group - fewer resources to cope * Racism and discrimination |
|
|
Cognitive Appraisal
|
Personal interpretation of a situation
|
|
|
Primary appraisal
|
-quick assessment of what a situation means to us
* Ex: I only need a D on this test to pass it, not too stressed |
|
|
Secondary appraisal
|
-self assessment of the resources required to deal with the stressor
* Ex: Do I have the time to study for the test? Am I confident in it? |
|
|
Personal control
|
-People that feel some control over a stress-producing event often show no more distress than people who don't experience that event
* Must be realistic to be adaptive |
|
|
Langer (1977): Nursing home study
|
-One nursing home was provided with higher control over their environment - healthy, more active and alert
* The other nursing home - low amount of control over their environment, twice as many people died in the time the experiment with conducted |
|
|
Optimistic Explanatory Style (Explanatory Style)
|
-Use external, unstable and specific explanations of negative events
-Able see that it might not be just our fault, but on other factors -Willing to turn the negative around and do better |
|
|
Pessimistic Explanatory Style (Explanatory Style)
|
-Use internal, stable and global explanations for negative events
- "My fault" - Not willing to turn the negative around |
|
|
Optimistic Explanatory Style (Event Rejection)
|
- What's his problem? (External)
- I must not be his type. (Unstable, temporary) - Maybe he's waiting for his girlfriend to arrive (Specific) |
|
|
Pessimistic Explanatory Style (Event Rejection)
|
- I must have said the wrong thing (internal, blames self)
- I'm a pretty boring guy and really not very good looking (stable, permanent) - No one is ever going to like me (global, pervasive) |
|
|
Chronic Negative Emotions
|
More likely to develop a chronic diseases (heart disease, cancers…)
|
|
|
Positive emotions
|
Associated with increased resistance to infection, decreased illnesses, less pain and increased longevity
|
|
|
Heath Psychology
|
How biology, behaviors and social factors influence health, illness and medical treatment
|
|
|
Psychosomatic Theory
|
Idea that emotional factors (ex: stress) can lead to/worsen the source of illness
|
|
|
Indirectly (Physical Effects of Stress)
|
-affects health by leading to behaviors that jeopardize physical well-being
* Stressed out- likely to eat poorly, sleep less… |
|
|
Directly (Physical Effects of Stress)
|
affects health by altering body functions
|
|
|
Adrenal glands (The Endocrine System)
|
primarily responsible for releasing hormones in response to stress
|
|
|
Stress hormones (Catecholamines)
|
fight-or-flight
* Epinephrine (AKA adrenaline) * Diminishes quickly |
|
|
The Endocrine System (Corticosteroids)
|
maintain actuation of the physiological systems during emergencies
* Cortisol: helpful in the short term |
|
|
Cortisol in acute stress (Short term)
|
* Reduce inflammation
* Enhance muscles * Help immune cells combat infection |
|
|
If the secretion is not turned off (Cortisol in acute stress)
|
* Hypertension
* High cholesterol * Immunosuppression * Reduced neurogenesis/neuroplasticity |
|
|
Selye (1950s)
|
Effects of exposure to extreme stress in rats
* Adrenal glands became enlarged * Stomach ulcers * Impaired immune system |
|
|
The Immune System
|
* White blood cells release antibodies
* Cortisol suppresses white blood cells * Reduced # of antibodies: reduced ability to fight antigens * Impair immune cell functioning |
|
|
Telomeres (Aging and chronic stress)
|
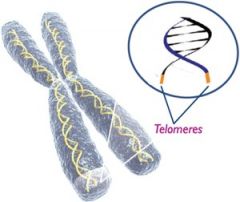
tips of chromosomes that protect genetic data - shorten as we age
|
|
|
Telomerase (Aging and chronic stress)
|
adds DNA/lengthens
* Short telomeres links with aging/disease/morality * Chronic stress: less telomerase activity which means shorter telomeres |
|
|
Type A Behavior and Hostility
|
* Exaggerated sense of time urgency
* Intense ambition and competitiveness * Greater hostility (anger and irritation) increase risk of heart disease |
|
|
Type B Behavior and Hostility
|
* More easygoing, relaxed, laid back
* Low hostility, not associated with heart disease |
|
|
Panic Attack
|
sudden episode of extreme anxiety that rapidly escalates in intensity
|
|
|
Effects of Panic Attack
|
* Pounding Heart
* Rapid Breathing * Breathlessness * Choking * Sweating * Trembling * Light-headed * Feelings of terror * Belief that one is going to die * Losing control/going crazy |
|
|
Agoraphobia
|
-Anxiety disorder involving the extreme/irrational fear of experiencing a panic attack in public place and not being able to escape / get help
* 1/3 panic disorder patients * Avoid: * Elevators * Crowds * Cars * Etc… * Many don’t leave their homes |
|
|
Triple Vulnerability Model (Explaining Panic Disorder)
|
1. Biological predisposition
2. Low sense of control over potentially life-threatening events 3. Hypersensitive to signs of physical arousal |
|
|
Catastrophic Cognition's Theory (Explaining Panic Disorder)
|
Not only are they more sensitive to physical aspects
* Also catastrophize meaning of experiences * ex. climbing stairs |
|
|
Phobias
|
Persistent and Irrational fear of a specific object, situation, or activity
* Its common to have fears * Only a phobia if it interferes with your functions |
|
|
Specific Phobias
|
Excessive, intense, irrational fear of specific object, situation, or activity that is actively avoided or educed with high anxiety
* Can provoke panic attack * Person knows fear is excessive / irrational * 13% experience in their lives * Women outnumber men 2:1 |
|
|
5 Categories (Specific Phobias)
|
* Fear of particular situations
* Fear of features of the natural environment * Fear of injury or blood * Fear of animals and insects * Other (e.g. vomiting) |
|
|
Social Phobia
|
Extreme and irrational fear of being embarrassed, judged, or scrutinized by others in social situations
* Interferes with functioning * Situations avoided or endured with high anxiety * Specific or generalized * 12.1% of population * Slightly more Females * Most Common: fear of public speaking |
|
|
Learning Theories
|
neutral stimulus + Traumatic experience -> fear response
* What type of conditioning is this? * Classical * People usually generalize everything in this (e.g. dogs) * Avoidance is negatively reinforced * Reduces anxiety/fear * What type of condition is this? * Operant |
|
|
Observational Learning
|
* Some become phobic by watching fearful reactions of others
* Or by hearing/seeing traumatic experiences of others |
|
|
Post Traumatic Stress Disorder (PTSD)
|
* Chronic and persistent symptoms of anxiety in response to an extreme physical or psychological trauma
* Re-experiencing (e.g. memories, nightmares, flashbacks) - intrusive * Emotional numbing and interpersonal problems * Increased physical arousal * Only diagnosed after one-month post trauma * Acute stress disorder |
|
|
Obsessive-Complusive Disorder (OCD)
|
* Symptoms of anxiety are triggered by intrusive, repetitive thoughts and urges to perform certain actions
|
|
|
Obsessions
|
repeated / intrusive / uncontrollable / irrational thoughts or images causing extreme distress
* Far-fetched w/ little basis in reality |
|
|
Compulsions
|
repetitive behavior or mental acts performed to prevent / reduce anxiety
* 2% population * 3/4 OCD patients have multiple obsessions * 1/2 have more than one compulsion |
|
|
Irrational Belief
|
Failure to perform ritual will lead to catastrophic or disastrous outcome
* Prone to superstitious / “magical” thinking * Most know this is irrational * Can have obsessions, compulsions, or both |
|
|
Mood Disorders
|
significant and persistent disruptions in mood or emotions that cause impairment in cognitive, behavior and/or physical functioning
|
|
|
Emotions violate “normal” moods in:
|
* Quality
* Duration * Intensity |
|
|
Major Depressive Disorder
|
- Characterized by having at least 1 major depressive episode
- Causes impaired emotional cognitive, behavior and physical functioning * Lifetime prevalence: 8-19% * Most common psychological disorder * 2:1 female to male ratio * Course = episodic * Possible to have only one major depressive episode, but not common |
|
|
Qualification for Major Depressive Disorder
|
Symptoms present for at least two consecutive weeks
* Low Mood * Anhedonia (low interest) * Lack of motivation * Feelings of worthlessness * Excessive guilt * Sleep disturbance * Suicidal thoughts * Weight loss/ weight gain * Difficulty concentrating |
|
|
Dysthymic Disorder
|
* Milder but longer lasting depression
* Subjective discomfort * No serious functional impairment * At least 2 years * No more than 2 months w/o symptoms |
|
|
Double Depression
|
dysthymia + major depression
|
|
|
Bipolar Disorder
|
Involving periods of incapacitating depression alternating with periods of extreme euphoria / excitement
* Prevalence: * Lifetime prevalence .4-1.6% * Males=Females * Episodic Course: cycle between (hypo)mania |
|
|
Manic Episode
|
sudden, rapidly escalating emotional state with extreme euphoria, excitement, physical energy, rapid thoughts, and speech
|
|
|
Effects of Manic Episodes
|
* Inflated self-esteem
* Require little sleep * Grandiose ideas * Rapid speech * Flight of Ideas * Inappropriate / Uncharacteristic Impulsive behavior |
|
|
Hypomania
|
Abnormally elevated mood at least 4 days (less severe than Manic Episode)
|
|
|
Affects of Hypomania
|
* High productivity
* Need little sleep * Bipolar 2 |
|
|
Cyclothymic Disorder
|
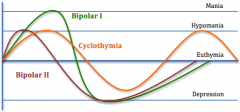
Moderate but frequent mood swings that are not severe enough to qualify as bipolar/depression
|
|
|
Antidepressants increase availability of
|
* Norepinephrine
* Serotonin |
|
|
Bipolar (treated with)
|
Glutamate (treated with lithium)
|
|
|
Eating Disorders
|
* Anorexia Nervosa
* Bulimia Nervosa * Binge Eating Disorder |
|
|
Anorexia Nervosa (symptoms)
|
* Intense fear of gaining weight
* Disturbed body image * Refusal to maintain body weight at or above minimal normal weight (15% or below) * Amenorrhea (loss of menstrual cycle) * Denies seriousness of weight loss |
|
|
Anorexia Nervosa (2 Subtypes)
|
* Restricting type
* Bingeing / Purging type * 1-2% lifetime prevalence * resistant to treatment * Often times linked with a need for control * Often begins with dieting * Life threatening |
|
|
Bulimia Nervosa (symptoms)
|
* Periods of objective bingeing (eating more than normal) with a sense of loss of control
* Inappropriate compensatory behaviors * Self-evauation unduly influenced by body weight/shape * Binges occur at lease twice a week for 3 months |
|
|
Bulimia Nervosa (2 Types)
|
* Purging type: Vomiting
* Non-purging type * Exercise (many hours) * Laxatives * Metabolism pills, other medications |
|
|
Bulimia Nervosa (facts)
|
* 1.2% Lifetime prevalence
* 90% female * Most within 10% of their normal body weight * Non conducive to weight loss * More likely to seek treatment than anorexic patients * Feeling of loss of control |
|
|
Psychotherapy
|
use of psychological techniques to treat emotional, behavior, and interpersonal problems.
|
|
|
Biomedical Therapies
|
use of medication to treat the symptoms of psychological disorders
|
|
|
Who provides Therapy?
|
- Doctoral Degree (Ph.D., Psy.D., or E.D.)
- Medical Degree (M.D.) - Masters Degree |
|
|
Doctoral Degree (Ph.D., Psy.D., or E.D.)
|
Clinical and counseling psychologists
|
|
|
Medical Degree (M.D.)
|
* Psychiatrists
* Can prescribe medications |
|
|
Masters Degree
|
* Social Workers
* Counselors |
|
|
Psychoanalysis
|
* The origin of “talk therapy”
* Developed by Freud * Cause of mental illness is unconscious conflict * Defense mechanisms protect against anxiety * Repression = keeping out of consciousness * Goal of therapy is to help clients achieve insight. |
|
|
Repression
|
keeping out of consciousness
|
|
|
How does the therapist help the client gain insight? (psychoanalysis)
|
* Therapist helps interprets and analyze information
* Free association * Dream interpretation * Transference: client projects feelings about someone else (e.g., a parent) onto the therapist * Therapist stays neutral so the client can project * Work through themes from old relationships |
|
|
Transference
|
client projects feelings about someone else (e.g., a parent) onto the therapist
|
|
|
Psychoanalysis Today
|
* Originally 3-6 times a week for years
* Now, briefer form exist |
|
|
Psychodynamic therapy
|
* Unconscious
* Early/Childhood experiences |
|
|
Interpersonal therapy
|
* Focus on current rather than past relationships
* Interpersonal deficits and patterns * Giving direct feedback to client |
|
|
Mental Illness
|
personal growth is being blocked
|
|
|
Humanistic Psychotherapies
|
* Mental Illness: personal growth is being blocked
* Person-centered approach * Move away from “client is sick, therapist will fix” * Focus on the clients perception * Active listening: echo, restate, clarify * Empathy, genuineness, unconditional positive regard * Goal is to help clients reach self-actualization * Create environment so they can help themselves |
|
|
Humanistic: Positive Psychotherapy
|
* Increasing a persons happiness, well-being, and positive emotions
* Gratitude training * 3 good things * (write down why it happened) * Gratitude letter * Character strengths * (authentichappiness.com) |
|
|
Motivational Interviewing
|
* Help clients overcome reluctance to change
* Skills * Open ended questions * Providing affirmation * Reflective listening * Summary statements * Explore pros and cons of future with and without change * Especially useful for substance abuse disorders, eating disorders |
|
|
Behavioral Therapies
|
* Maladaptive behaviors are the problem, not a symptom
* Goal: modify problematic behavior * Unlearn certain behaviors * Operant and classical conditioning * Modeling |
|
|
Exposure Therapy
|
* Anxiety disorders
* Expose to feared stimulus until fear response is extinguished |
|
|
Behavior Modification
|
Childhood disorders, autism spectrum disorders, health psychology, etc.
|
|
|
Exposure Therapy: Flooding
|
Extreme exposure to a phobic object/stimulation
|
|
|
Exposure Therapy: Systematic Desensitization
|
* Pairs relaxation with gradual exposure to a phobic object
* Hierarchy of aversive stimuli * Exposure can be imagined, virtual, or real |
|
|
Behavior Modification
|
* Use operant conditioning to reinforce behaviors
* Token economies |
|
|
Cognitive Therapies
|
* Cause of mental illness = maladaptive thoughts
* Automatic * Goal = identify and change maladaptive thoughts * Role of therapist * Challenge maladaptive beliefs * Search for evidence to support/refute thoughts * Identify and help change distorted perceptions |
|
|
Patterns of problematic thinking
|
* Catastrophizing
* All-or-nothing thinking * Etc… |
|
|
ABC Model
|
* Activating Event
* Beliefs * Consequences |
|
|
Cognitive Behavioral Therapy (CBT)
|
* Integration of cognitive and behavior therapies
* Most commonly used therapy * Interaction between thoughts and behavior * Behavioral Activation |
|
|
Groups therapy
|
1+ therapists working with a group of clients
* More cost efficient * Can provide microcosm of social environment * Help clients feel less alone |
|
|
Family Therapy
|
* Focus on family as a unit (more than the sum of the parts)
* Focus on “rules” of communication/interaction * Couples therapy |
|
|
Antipsychotic Drugs
|
* Helps positive psychotic symtooms
* Little effect on negative symptoms * Block dopamine activity in brain * Side Effect: Tardive Dyskinesia * Problems with Parkinson’s like motor symptoms * Side effects: “Revolving door” * Hospitalized, stabilized, go off meds, rehospitalized * Atypical antipsychotics -> no motor side effects * targets different dopamine receptors * Side Effects = weight gain, diabetes, reduction in white blood cells |
|
|
Tardive Dyskinesia
|
Problems with Parkinson’s like motor symptoms
|
|
|
Side effects: “Revolving door”
|
Hospitalized, stabilized, go off meds, rehospitalized
|
|
|
Atypical antipsychotics
|
no motor side effects
* targets different dopamine receptors * Side Effects = weight gain, diabetes, reduction in white blood cells |
|
|
Benzodiazepines (Benzos)
|
* Valium, Xanax
* Suppress the stress response, slow brain activity * Immediate effect |
|
|
Buspar
|
* Not sure how it works
* serotonin, dopamine? * Longer term-effective after 2-3 weeks * No risk of addiction |
|
|
Antidepressants - Tricyclics & MAO Inhibitors
|
Increase activity of excitatory neurotransmitters, norepinephrine and serotonin
|
|
|
Tricyclics
|
* Prevent reuptake
* Side effect: weight gain, irritability, confusion, hypertension |
|
|
MAO Inhibitors
|
* Reduce activity of enzyme MAO
* Side effects: * May have negative interaction with many foods and antihistamines |
|
|
Antidepressants - SSRIs
|
* Selective Serotonin Reuptake Inhibitors
* Most common * Increase activity of serotonin by preventing reuptake * Milder side effect than other antidepressants * Agitation, insomnia, nausea, sexual dysfunction * Reduce depressive symptoms more rapidly |
|
|
SSRIs
|
Selective Serotonin Reuptake Inhibitors
|
|
|
Electroconvulsive Therapy (ECT)
|
* Passing electrical current through brain in order to induce localized seizures
* Patients given an anesthetic and muscle relaxant * Side effect: memory loss * Currently used for severe depression * often after other things (therapy, drugs) haven’t worked * Especially among actively suicidal patients * Don’t really understand why this treatment relieves symptoms * Brain reboot? * Controversial |
|
|
`Medications may not be as effective as we think
|
* “File drawer effect”
* 1/3 of FDA studies (most with negative results) not published * Antidepressants may not be more effective than placebos |
|
|
Atypical antipsychotics
|
best at treating positive symptoms
|
|
|
Issue
|
medication compliance
|
|
|
ECT
|
* treatment of last resort
* Improvements in mood are not long lasting |
|
|
Dodo Bird verdict
|
psychotherapy tends to work, but which kind of therapy doest not appear to matter much
|
|
|
Therapist characteristics
|
* Caring, genuinely concerned, empathetic
* Warm, sensitive, responsive, sincere * Explanation for clients symptoms seem plausible * Culturally sensitive |
|
|
Client Characteristics
|
* Committed, motivated, engaged in process
* External circumstances * Client belief in therapist s abilities * Optimistic that treatment will work |
|
|
Electric Therapists
|
Choose strategies depending on clients presenting problem
|
|
|
Integrative therapists
|
Blend multiple approaches together
|