![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
25 Cards in this Set
- Front
- Back
|
Bipolar Disorder |
- Manic-depression disorder; fluctuation between episodes of mania, depression and normalcy Manic episode: - emotional euphoria - Cognitive hyperactivity: increased productivity and creativity - Motor hyperactivity Prevalence and onset: - Peak vulnerability between 20 and 29 years - 1 to 2.5% of population: no sex difference Cyclothymic disorder: less severe symptoms |
|
|
Schizophrenia Symptoms |
Disorganized thought: - Delusions: persistent and unrealistic false beliefs - Broadcast thoughts, imposed thoughts and thought control - Delusions of grandeur - Thought processes become chaotic Disorganized perception: - Hallucinations: perceptions that occur in the absence of a physical stimulus, or that are distorted Disorganized behaviour: - Deterioration of routine functioning (work, social, personal care) Disturbed emotion: - Blunted or inappropriate affect; volatility(0-100 real quick) |
|
|
Schizophrenia Specifiers |
Paranoid (common): - Delusions of persecution and grandeur - Become suspicious of social network, institutions, unknown persons/entities Catatonic (uncommon): - Motor disturbances (rigidity, random activity) - Catatonic stupor (withdrawal) - Catatonic excitement (hyperactivity) Disorganized: - severe deterioration of adaptive behaviour - Emotional blunting, social withdrawal |
|
|
Positive and Negative symptoms |
Negative symptoms: - behavioural deficits: blunted affect, social withdrawal, impaired attention, poverty of speech Positive symptoms: - behavioural excesses or peculiarities: delusions, hallucinations, bizarre behaviour, chaotic thoughts - better adjustment before onset - better response to treatment Most patients exhibit both; differ in degree only |
|
|
Course and outcome |
- usually emerges (sudden or gradual) during adolescence or early adulthood Disorder severity: - Mild: full recovery - Moderate: partial recovery and frequently relapse -Chronic: permanent hospitalization -Male patients: earlier onset; more severe; higher relapse rate Favourable prognosis when: - Onset is sudden and at later age - Adjustment before onset was good - fewer negative symptoms - social support |
|
|
Etiology of Schizophrenia |
- genetic vulnerability Neurochemical Factors: - excessive dopamine activity - Serotonin and glutamate Brain abnormalities - enlarged brain ventricles - increased activity in temporal lobe - increased dopamine production (positive symptoms) - decreased dopamine activity in prefrontal lobe (negative symptoms) |
|
|
Neurodevelopmental hypothesis |
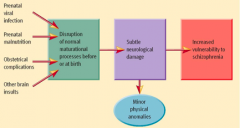
- disruptions during maturation of brain before or at birth increase vulnerability to schizophrenia later in life |
|
|
Schizophrenia progression |
-factors that exacerbate illness after onset. One factor is Expressed Emotion - degree to which relatives express negative emotions towards patient: overly critical; overly protective - social stress; not social support - relapse rate is 3 times higher in high EE families Marijuana use? no evidence that marijuana causes schizophrenia but higher in the rate of using marijuana - stress can trigger schizophrenic episodes in those with increased vulnerability (genes); trigger relapses. |
|
|
Somatoform Disorders |
Physical ailments with no organic explanation; largely expression of psychological factors - not psychosomatic: genuine ailments caused by psychological factors such as stress (asthma, high blood pressure) - not malingering (faking illness) Somatization Disorder: history of diverse minor physical complaints that appear psychological in origin - gastrointestinal problems: aches and pains, headaches - wax and wane with stress - more common in women - often coexist with anxiety and mood disorders. |
|
|
Somatoform disorder: conversion disorder and hypochondriasis |
Conversion disorder: loss of physical function with no organic basis - symptoms not consistent with medical knowledge - single system: partial or complete loss of sensations (vision, hearing, glove anesthesia), paralysis and laryngitis Hypochondriasis: preoccupation with health and concerned with developing physical illness - dont experience phantom disease -Over interpret physical symptoms -drain on medical system coexists with anxiety and mood disorders |
|
|
Dissociative Disorders |
- Individual loses contact with portions of consciousness or memory; disrupting identity. Dissociative amnesia: loss of memory for an event or information that cannot be accounted for by mere forgetting. (single episode that is missing) - Precipitated by a traumatic event (ex. disaster, accident, death, abuse or rape) Dissociative fugue: loss of memory for one's identity. - episodic memory impaired - procedural and semantic memory remain intact |
|
|
Dissociative Identity Disorder (DID) |
Multiple Personality Disorder: coexistence of two or more complete and independent personalities (very rare) - Large disparities between personalities (different personalities could be a different age etc) - Personalities unaware of each other - Not the same thing as different roles - Appears with anxiety, mood and personality disorders Diagnosis of DID began to increase in 1970s. - before 1970: 79 documented cases(under diagnosis?) - Next 30 years: 40,000 cases (over diagnosis?) - Modestin: surveyed 655 swiss psychiatrists -- 90% never diagnosed DID -- 3 psychiatrists diagnosed 20+ cases each - 6 psychiatrists accounted for 2/3 of all diagnosis. |
|
|
Cause of Dissociative Identity Disorder |
Cause of DID unknown. Spanos(1994;1996): DID reflects intentional role playing - symptoms changed with schema of DID - sybil published in 1973: girl with lots of personalities. (after published people diagnosed had lots of personalities) - Michelle remembers published 1980 - cases manufactured by minority of clinicians DID precipitated by childhood trauma (rejection, abuse): - cases of abuse are unverified. Impossible to identify if they actually happened or not. - Not unique to DID |
|
|
Personality disorders |
Extreme, inflexible personality traits that cause subjective distress or impaired social functioning - imaginary line between disorder and normalcy(everyone has personality traits but ppl with disorder are really high in certain traits) - Emerge during late childhood/ early adolescence - Very common - Some are mild versions of Axis 1 disorders Anxious/fearful disorders: maladaptive efforts to master anxiety or fear of rejection Odd/eccentric disorders: distrustful & aloof; exhibit mild symptoms consistent with schizophrenia Dramatic/impulsive disorders |
|
|
Cluster B: impulsive personality disorders - antisocial personality |
Antisocial Personality: disregard for rights of others. - lack of respect for social norms and rules - Criminal activity - Deceitfulness (cheating and conning) - Impulsive & reckless (sex and drugs) - irresponsible (unemployment) but not all are unemployed - Lack of remorse Most problematic personality disorder -Male/female ration: 82/18 |
|
|
Cluster B: impulsive personality disorders - Borderline personality |
Borderline personality: unstable relationships, self-image, affect. - frantic efforts to avoid real or imagined abandonment - intense but unstable relationships (idealization and devaluation) - identity disturbances - impulsivity - Suicidal behaviour or threats; self-mutilation - emotional volatility (change in emotion) - inappropriate and intense anger - paranoia Male/female ratio: 38/62 |
|
|
Cluster B: dramatic personality disorders - histrionic personality |
Histrionic personality: excessive emotionality and attention seeking - Need to be centre of attention - Rapid shifting of emotion; exaggerated expression of emotion -Conspicuous(standing out) appearance to attract attention - exaggerated expression of speech - highly suggestible - overestimates intimacy levels in relationship Male/female ratio: 15/85 |
|
|
dramatic personality disorders - narcissistic personality |
Narcissistic personality: grandiosity, need for admiration, lack of empathy - self importance (exaggerates achievements) - sense of entitlement (expect favourable treatment) - belief that they are special or unique - preoccupation with fantasies of success, genius, beauty, etc. - exploitative, arrogant, envious Male/female ratio: 70/30 |
|
|
Anxious/fearful personality disorders 1 of 3 Avoidant personality disorder |
Excessively sensitive to potential rejection, humiliation, or shame; socially withdrawn in spite of desire for acceptance from others - 50/50 |
|
|
Dependent personality disorder |
Excessively lacking in self-reliance and self-esteem; passively allowing others to make all decisions; constantly subordinating own needs to others' needs. - 31/69 |
|
|
Obsessive-compulsive personality disorder |
Preoccupied with organization, rules, schedules, lists, trivial details; extremely conventional, serious, and formal; unable to express warm emotions - 50/50 |
|
|
odd/eccentric personality disorders 1 of 3(reflect lighter forms of schizophrenia) - schizoid personality disorder |
Defective in capacity for forming social relationships; showing absence of warm, tender feelings for others - 78/22 |
|
|
Schizotypal personality disorder |
showing social deficits and oddities of thinking, perception, and communication that resemble schizophrenia - 55/45 |
|
|
Paranoid personality disorder |
Showing pervasive and unwarranted suspiciousness and mistrust of people; overly sensitive; prone to jealousy |
|
|
Diagnostic problems |
- categories overlap too much More(1988): 291 patients who received a specific personality disorder; many qualified for other disorders: - histrionic(dramatic): - 56% qualified for borderline - 54% for narcissistic - 32% for avoidant - 30% for dependent - makes it difficult to research cause and prognosis - Dimensional approach: score along several continuous dimensions; similar to personality assessment |