Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
110 Cards in this Set
- Front
- Back
|
Where should the top of the IR be for a lateral sternum?
|
1 1/2 inches superior to the jugular notch
|
|
|
Whats the level of the sternal angle?
|
T4-T5
|
|
|
The body is turned ___ to ___ degrees for oblique sternum with the ____ side down.
|
15-20 degrees with the right side down (RAO).
|
|
|
true ribs are ___ - ___ because they attach directly to the sternum by it's own costocartilage
|
1 - 7
|
|
|
false ribs are ___ to ___ because they do not attach directly to the sternum.
|
8 - 12
|
|
|
ribs __ and __ only attach to the vertebrae and are called floating ribs.
|
11 and 12
|
|
|
where is the CR for oblique sternum?
|
midsternum, midway between jugular notch and xiphoid tip.
|
|
|
The most inferior portion of the sternum?
|
xiphoid
|
|
|
The longest part of the sternum is the ___
|
body
|
|
|
what is the level of the jug notch?
|
T2-T3
|
|
|
Whats the breathing technique for oblique sternum
|
gentle even breathing during exposure
|
|
|
The heads of ribs articulate with ____ and form ____ joint
|
vertebral body
costovertebral joint |
|
|
Tubercles of the rib articulate with ______ and form _____ joint
|
T-spine transverse processes;
costotransverse |
|
|
Hypersthenic patient type has a ________ diaphragm
|
higher positional
|
|
|
CR for oblique sternum is _____ inch(es) left to the midline.
|
1 inch
|
|
|
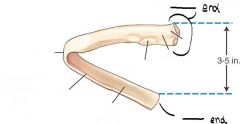
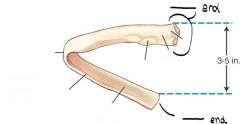
The posterior end of a rib is the _______ end
|
vertebral
|
|
|
The anterior end of a rib is the ________ end
|
sternal
|
|
|
Hyposthenic patient has a ______________
|
lower-positioned diaphragm
|
|
|
how much is the body rotated for RAO/LAO sternoclavicular joints?
|
10-15 degrees from PA
|
|
|
For RAO/LAO sternoclavicular joints, where is the CR
|
level of T2-T3, 3 inches distal to vertebra prominens, 1 to 2 inches lateral to midsagittal plane.
|
|
|
Where is the CR for AP below diaphragm?
|
midway between xiphoid process and lower ribs
|
|
|
breathing technique for above the diaphragm is _______; breathing technique for below the diaphragm is __________
|
inspiration ; expiration
|
|
|
where is the CR for posterior oblique ribs
|
midway between xiphoid process and iliac crest
|
|
|
T/F
hypersthenic patient requires greater rotation of the sternum for RAO projection as compared to a sthenic patient |
False
|
|
|
inside margin of the rib containing the blood vessels and nerves?
|
costal groove
|
|
|
T/F
anterior ends of the ribs do not attach directly to the sternum |
true
attach to costocartilage |
|
|
which position can replace the RAO sternum for the trauma patient who cannot lie prone or stand
|
LPO
|
|
|
T/F
The ideal general position for a study of the ribs below the diaphragm is recumbent |
True
|
|
|
pulmonary injury caused by blunt trauma to two or more ribs
|
flail chest
|
|
|
Anterior protrusion of the lower sternum and xiphiod process
|
Pectus carinatum (pigeon breast)
|
|
|
pectus carinatum is a _________ anomaly
|
congenital
|
|
|
a depressed sternum due to a congenital defect
|
pectus excavatum
|
|
|
destructive lesions with irregular margins
|
Osteolytic
|
|
|
A proliferative bony lesion of increased density
|
osteoblastic
|
|
|
this can be post operative complication of open heart surgery since sternum is split for the surgery
|
Osteomyelitis
|
|
|
Localized infection of bone, and marrow.
|
Osteomyelitis
|
|
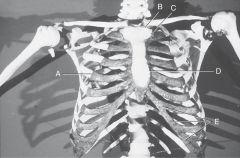
Label the above diagram
|
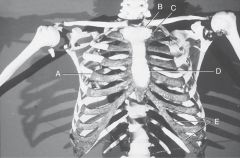
A. costochondral union or junction
B. sternoclavicular joint C. sternocostal joint D. 4th sternocostal joint E. continuous borders of the interchondral joints |
|
|
What kind of mobility type does the 1-10th costochondral unions (btw costocartilage and ribs) have?
|
synarthrodial
|
|
|
What is the mobility, movement, and classification of the sternoclavicular joints?
|
Synovial
diarthrodial plane (gliding) |
|
|
What classification and mobility type are the first sternocostal joints?
|
cartilaginous
synarthrodial |
|
|
What classification, mobility type, and movement is do the 2nd-7th sternocostal joints have
|
synovial
diarthrodial plane (gliding) |
|
|
What classification, mobility type, and movement is do the 6th -10th interchondral joints have
|
synovial
diarthrodial plane (gliding) |
|
|
What classification, movement type, and mobility does the 1st -10th constotransverse joints have?
|
synovial
diathrodial plane (gliding) |
|
|
What classification, movement type, and mobility does the 1st -12th costovertebral joints have?
|
synovial
diarthrodial plane (gliding) |
|
|
A radiograph of an RAO sternum reveals that part of the sternum is superimposed over the Tspine. Which specific posistioning error is visible on this radiograph?
|
underrotation of the PT
|
|
|
A radiograph of an RAO sternum reveals that the sternum is poorly visualized because of excessive lung markings superimposed over the sternum. the following factors were used: 65kV, 200mA, 1 1/4- sec exposure, 40" SID, bucky, and 100 speed screens. which of these factors can be altered to increase the visibility of the sternum?
|
increase the exposure time (and lower the mA) to allow for greater blurring of the lung markings
|
|
|
A radiograph on an RAO sternum reveals that the sternum is difficult to visualize because of excessive density. the following factors were used: 75kV, 25 mA, 3sec exposure, 40" SID, bucky, and 100 speed screens. which one of these factors should be modified during the repeat exposure to produce a more diagnostic image>
|
lower the kV to 65 for higher contrast and to prevent overpenetration of the sternum
|
|
|
What classification, movement type, and mobility does the 1st -10th constotransverse joints have?
|
synovial
diathrodial plane (gliding) |
|
|
What classification, movement type, and mobility does the 1st -12th costovertebral joints have?
|
synovial
diarthrodial plane (gliding) |
|
|
A radiograph of an RAO sternum reveals that part of the sternum is superimposed over the Tspine. Which specific posistioning error is visible on this radiograph?
|
underrotation of the PT
|
|
|
A radiograph of an RAO sternum reveals that the sternum is poorly visualized because of excessive lung markings superimposed over the sternum. the following factors were used: 65kV, 200mA, 1 1/4- sec exposure, 40" SID, bucky, and 100 speed screens. which of these factors can be altered to increase the visibility of the sternum?
|
increase the exposure time (and lower the mA) to allow for greater blurring of the lung markings
|
|
|
A radiograph on an RAO sternum reveals that the sternum is difficult to visualize because of excessive density. the following factors were used: 75kV, 25 mA, 3sec exposure, 40" SID, bucky, and 100 speed screens. which one of these factors should be modified during the repeat exposure to produce a more diagnostic image>
|
lower the kV to 65 for higher contrast and to prevent overpenetration of the sternum
|
|
|
A radiograph of a lateral projection of the sternum reveals that the PTs breasts are obscuring the sternum. what can be done to minimize the breast artifact over the sternum'?
|
have the pt bring the breasts to the side, hold them in position with a wide bandage
|
|
|
repeat PA projections of the Sternoclavicular joints do not clearly demonstrate them. what other imaging modality may produce a more diagnostic image of these joints
|
CT
|
|
|
A pT with trauma to the sternum and the left sternoclavicular joint region enters the ER. in addition to the sternum routine, the ER physician asks for a specific projection to better demonstrate the left sternoclavicular joint. describe the positioning routine, including the breathing instructions that you would use.
|
15-20 deg RAO sternum with breathing techinique
lateral sternum on inspiration 10-15deg LAO of sternoclavicular joint with suspended inspiration |
|
|
A radiograph of the upper ribs demonstrates that the diaphragm is superimposed over the 8th ribs, which is in the area of interest. the following factors were used for the inital exposure: 65kV, 400mA, 1/40th sec, 400 speed screens, grid, suspended respiration on expiration, erect posistion, 40" SID. which one of the factors can be modifies to increase the visibility of the area of interest
|
suspend respiration during inspiration to move the diaphragm below the eigth ribs
|
|
|
a pt enters the ER on a backboard after being involved in a motor vehicle accident. because of the condition of the pt the physician orders a portable study of the sternum in the ER. which two projections of the sternum would be most diagnostic yet minimize movement of the pt
|
LPO and horizontal beam lateral projections.
|
|
|
a pt with trauma to the right upper anterior ribs enters the ER. he is able to sit in an erect position. which positioning routine of the ribs should be performed?
|
erect PA and LAO (or RPO) position with suspended inspiration
|
|
|
a pt with trauma to the left lower anterior ribs enters the ER. which positioning routine of the ribs should be performed?
|
recumbent PA (orAP if the PT can not assume prone position) and RAO (or LPO) positions with suspended expiration
|
|
|
An elderly pt comes to the radiology department for a complete rib series with an emphasis on the posterior ribs.. she has advanced osteoporosis and has difficulty moving and lying down. her physician wants both upper and lower ribs examined. what type of positions should be performed? how would you adjust the technical factors for this patient?
|
bc of pt condition, it is best to perform all positions erect and initiate exposure on full inpiration for upper ribs and full expiration for lower ribs, (RPO and LPO) must be performed, it is recommended that kV (manual technique employed) for all projections be lowered because of the advanced osteoporosis
|
|
|
a pt enters the er with blunt trauma to the chest. he is restricted on a backboard. the ER physician suspects a flail chest. beyond the initial chest projections, what positioning routine would confirm the diagnosis of a flail chest?
|
a limited rib series will indicate which ribs are fractured (and whether this has led to flail chest) since the pt is restricted to a backboard, the oblique positions may not be possible
|
|
|
What is the name of the joint that connects the upper limb to the bony thorax?
|
sternoclavicular joint
|
|
|
What is the name of the section of cartilage that connects the anterior end of the rib to the sternum?
|
costocartilage
|
|
|
Whats the difference between a true and false rib?
|
true ribs connect to the sternum by their own costocartilage. False ribs are connected to the sternum via the costocartilage of the seventh rib.
|
|
|
T/F the anterior end of the rib is called vertebral end
|
False
sternal end |
|
|
List the three structures found within the costal groove of each rib?
|
artery
vein nerve |
|
|
Is the posterior vertebral end or the anterior sternal end most superior?
|
posterior vertebral end is most superior
|
|
|
How much difference in height is there between the posterior and anterior ends?
|
3 to 5 inches
|
|
|
Which ribs articulate with the upper lateral aspect of the manubrium of the sternum?
|
1st anterior sternal end
|
|
|
the bony thorax is widest at the lateral margins of which ribs?
|
8th or 9th
|
|
|
How many posterior ribs are shown above the diaphragm?
|
11
|
|
|
Whats unique about true ribs 1-7
|
each attaches to the sternum by its own costocartilage
|
|
|
Whats unique about floating ribs 11-12
|
they do not attach to anything anteriorly
|
|
|
is it possible to view the sternum with a PA or AP projection?
|
no
|
|
|
An injury to the region of the eighth or ninth rib would require (above/below) diaphragm technique?
|
above
|
|
|
the head, neck, and tubercle are at the ______ end of the rib
|
vertebral
|
|
|
to best demonstrate the ribs below the diaphragm the tech should have the patient in a ______ position.
|
recumbent
|
|
|
for above the diaphragm a _____ kv from ___ to ___ should be used;
for below the diaphragm a ____ kv from ___ to ___ should be used. |
for above the diaphragm a low kv from 65 to 70 should be used;
for below the diaphragm a medium kv from 70 to 80 should be used. |
|
|
A patient has an injury to the right anterior ribs, which obl is best?
|
LAO
|
|
|
A patient has an injury to the left posterior ribs, which obl is best?
|
LPO
|
|
|
For AP ribs the area of interest is _____ to the IR (for a posterior rib injury)
|
closest
|
|
|
physician suspects rib injury caused pneumothorax or hemothorax, which additional projection should be done
|
erect PA and lateral chest
|
|
|
Is a high or low breathing technique required for obl sternum?
|
high 3 to 4 seconds
|
|
|
list the preferred positioning factors for ribs below diaphragm.
body position? breathing ? kv range? |
body: recumbent
breathing:expiration kV range: medium 70 to 80 |
|
|
Osteolytic Metastases of the ribs produce what type of radiographic appearance?
|
irregular bony margins
|
|
|
Why is RAO preferred for a study of the sternum
|
it places the sternum over the heart to provide a uniform background for added visibility of the sternum
|
|
|
What other position can be preformed if patient cannot do RAO sternum prone?
|
LPO supine
|
|
|
Whats the breathing technique for PA SC joints?
|
suspend respiration on inspiration
|
|
|
Which position will best demonstrate the right sternoclavicular joint?
|
RAO
|
|
|
For RAO /LAO SC joints, the CR is at the level of T2 to T3, and 1 to 2 inches lateral to the (upside or downside)
|
upside
|
|
|
Where is the CR for an AP projection of the ribs for an injury located above the diaphragm?
|
3 to 4 inches below jug notch
level of T7 |
|
|
Which obl positions elongate the left axillary portion of the ribs?
|
RAO & LPO
|
|
|
the patient thyroid and breast dose for PA SC joints is ______
|
1 TO 5 mrad
|
|
|
T/F the gonadal dose given for ribs projection is less than 1mrad
|
true
|
|
|
A patient who has a underlying pulmonary injury and suffers a blunt trauma to the chest may have ______ chest
|
flail chest
|
|
label
|
|
|
|
|
|
|
How much obliquity should a large barrel chested person get for RAO sternum
|
15 degrees more is less
|
|
|
How much obliquity should a thin thorax get for RAO sternum ?
|
20 degrees
|
|
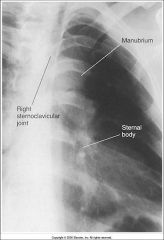
What is the issue with this RAO sternum
|
-under rotation
-right sternoclavicular joint not clear of vertebral column |
|

What is the issue with this RAO sternum
|
-under rotation
-right sternoclavicular joint not clear of vertebral column |
|
|
What is the name of the palpable junction between the upper and midportion of the sternum
|
sternal angle
|
|
|
What distinguishes a floating rib from a false rib?
|
floating ribs dont have cosotcartilage
|
|
|
which part of the sternum do the second ribs articulate ?
|
sternal angle
|
|
|
pathology of the sternum is most likely due to : ______
|
blunt trauma
|
|
|
Whats the average breast dose range for each of the following projections:
posterior obl rib: anterior obl rib: |
posterior obl: 66 mrad
anterior obl: 3mrad |
|
|
which of the following projections will best demonstrate the right axillary ribs?
LAO LPO RAO PA |
LAO
|
|
|
What can normally result when a hypersthenic patient is rotated more than 15 degrees for RAO sternum
|
foreshortening along the width of the sternum and will shift the sternum away excessively from spine.
|
|
|
AEC is generally is generally
(recommended/not recommended) for rib routines due to the need for high contrast, optimum detail exposures. |
not recommended)
|
|
|
T/F A breathing technique is recommended for studies of the sternoclavicular joints.
|
False
suspended upon expiration |