![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
109 Cards in this Set
- Front
- Back
|
What is the highly vascular structure that provides nutrition to the fetus? |
Placenta |
|
|
Approx. thickness of placenta |
2-4cm |
|
|
Aprrox. weight of placenta @ term |
600g |
|
|
What is the major functional unit of the placenta? |
chorionic villus |
|
|
Where are the intervillous spaces found? |
chorionic villus of placenta |
|
|
What happens in the intervillous spaces? |
transfer of gases and nutrients between maternal & fetal |
|
|
Know how to label diagram of placenta & decidual layers * see image on flip side |
|
|
|
Where is the fetal portion of placenta formed from? |
Chorion frondosum |
|
|
Chorionic villi that atrophy are now called what? |
chorionic laeve |
|
|
What covers the placental surface? |
amniotic membrane |
|
|
Know how to label intervillous spaces *see picture on flip side |

|
|
|
What forms the maternal portion of the placenta? |
Basalis |
|
|
Irregular grooves divide the Maternal portion into spaces called...? |
cotyledons |
|
|
Maternal blood flow is not established until when? |
~12 weeks gestation |
|
|
What is the entire purpose of the placenta? |
help the fetus survive |
|
|
What will the placenta do when the maternal environment is less than satisfactory? |
overcompensate for inadequacies |
|
|
Where does deoxygenated blood go after it leaves the fetus? |
through umbilical artery to placenta |
|
|
What does the umbilical artery divide into? |
multiple vessels that branch into chorionic plate |
|
|
What does the placental membrane prevent? |
intermixing of fetal & maternal blood |
|
|
2 Main functions of the Placenta |
1. exchange gas & nutrients 2. produce hormones to maintain pregnancy |
|
|
What hormone does the placenta secrete during early pregnancy? |
chorionic gonadotropin to maintain CL |
|
|
What hormones does the placenta produce in later pregnancy? |
estrogen & progesterone |
|
|
Sonographic appearance of Fetal surface of placenta |
- echogenic - represents chorionic plate - surrounded by amniotic fluid |
|
|
Sonographic appearance of Maternal surface of placenta |
basal plate - against myometrium w/ vessels crossing |
|
|
How should the placenta look on ultrasound? |
homogeneous - thickness varies |
|
|
What should the placental thickness be after the 6th month of pregnancy? |
~15mm |
|
|
What can occur in placenta secondary to Rh sensitization, diabetes, and congenital anomalies? |
Placentomegaly |
|
|
The placenta should NOT exceed what measurement? |
50mm |
|
|
Explain what you do when measuring the placenta |
- take perpendicular mmt from myometrium to fetal layer of placental tissue (thickest part) - avoid Braxton-Hicks contractions |
|
|
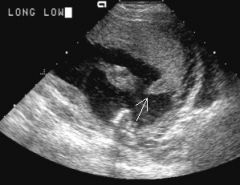
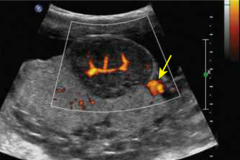
Name the 3 different Cystic Areas that may be visualized within the Placenta *also know Doppler of the 3 |
1. Large fetal vessels (flow)
2. Fibrin deposit (NO flow) 3. Placental lakes / venous lakes / maternal lakes (slow flow) |
|
|
Where can the placenta develop? |
anywhere along uterine endo lining |
|
|
What 2 things need to be specified when talking about placental position? |
1. location 2. relationship to cervix |
|
|
Placental Migration |
the apparent change in position of the placenta during serial ultrasounds during same pregnancy *placenta does NOT move - internal os of cervix does! |
|
|
What is required to see internal os & cervical length on ultrasound? |
FULL bladder |
|
|
How to measure placental position |
from end of placenta to internal os |
|
|
At what mmt is the placenta considered low-lying with increased risk of placenta previa? |
< 2cm |
|
|
When should low-lying placenta NOT be diagnosed prior to? Why? |
24 weeks - uterus still growing |
|
|
What can cause false diagnosis of previa? |
overfilling of bladder |
|
|
What is placental grading used for? |
assessing growth and stability of placenta throughtout pregnancy |
|
|
Maternal health plays a large factor in.... |
maturation of placenta |
|
|
Placental Grading - what weeks should they occur? |
Grade 0 < 28 weeks Grade 1 ~31 weeks Grade 2 ~36 weeks Grade 3 ~38 weeks |
|
|
Grade 0 < 28 weeks |

chorionic plate - smooth, well-defined placental tissue - homogenous basal plate - regular |
|
|
Grade 1 ~ 31 weeks |

chorionic plate - indentations placental tissue - calcium deposits basal plate - regular |
|
|
Grade 2 ~ 36 weeks |

chorionic plate - indentations linear densities extending from chorionic plate into placenta but NOT reaching basal plate |
|
|
Grade 3 ~ 38 weeks |

- linear densities extend to basal plate - placental septae w/ calcium deposits - complete circles of calcium |
|
|
What is evaluated on the post-partum placenta? |
- size - texture - membranes - meconium exposure?? |
|
|
What should the post-partum placenta measure and weigh? |
15-20cm diameter < 4cm thick 400-600 grams |
|
|
Placentomegaly |
when placenta weighs more than 600g |
|
|
Placentomegaly on U/S |
> 5cm thick |
|
|
Where do pathologies of the placenta typically arise from? |
maternal source |
|
|
Name 3 placental pathologies |
1. infection 2. decreased blood flow from mom to placenta 3. immunologic attack |
|
|
What is a real danger with abnormalities of placenta? |
IUGR |
|
|
Fibrin Deposit |
- found throughout placenta but prominent in placental floor or villi - increases throughout pregnancy |
|
|
Fibrin is a.... |
protein |
|
|
U/S of Fibrin deposit |

- hypoechoic area beneath chorionic plate (subchorionic) |
|
|
D/D for Fibrin deposit |
- venous lake (slow flow) - hematoma |
|
|
Placenta Previa |
when placenta implants OVER or NEAR internal os of cervix |
|
|
5 types of Placenta Previa |
1. Complete/Total 2. Partial 3. Marginal 4. Low-lying 5. Vasa Previa |
|
|
Complete / Total Previa |

completely covers internal os of cervix |
|
|
Partial Previa |
partially covers internal os |
|
|
Marginal Previa |
does not cover; placental edge touches os |
|
|
Low-lying Previa |
placental edge within 2cm of os |
|
|
Vasa Previa |
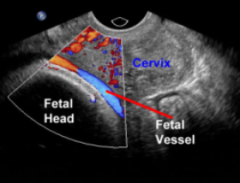
umbilical cord vessels precede presenting fetal part and overlie cervix |
|
|
Placenta Previa increases risk of what? |
Hemorrhage during labor |
|
|
As LUS thins & elongates in prep for delivery, what may happen to placenta? |
become loosened & bleed |
|
|
What can be disrupted as cervical dilation occurs? |
attachment of placenta |
|
|
Why is Previa not diagnosed until late 2nd trimester? (24 weeks) |
LUS is continuing to grow |
|
|
3 risk factors for Placenta Previa |
1. Multiparity 2. Prior c-sections 3. AMA |
|
|
Possible complications of Previa |
**premature delivery - life-threatening maternal hemorrhage - placenta accreta - postpartum hemorrhage - IUGR |
|
|
Signs / Symptoms of Placenta Previa |
PAINLESS bright red bleeding |
|
|
What is the most common cause of painless 2nd and 3rd trimester bleeding? |
Placenta Previa |
|
|
Delivery with Complete Previa |
will have to deliver c-section |
|
|
Delivery with Partial/Marginal Previa |
can attempt vaginal delivery |
|
|
U/S Complications with Previa |
- overly distended bladder can mimic previa (mmts should be taken before and after voiding) - Braxton-Hicks contractions (should resolve in 20 min) |
|
|
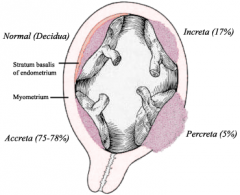
Placenta Accreta |

abnormal adherence of all/part of placenta with ABSENCE of all/part of decidua basalis - chorionic villi grow into myometrium |
|
|
In Placenta Accreta, where does the placenta anchor instead of decidua? |
myometrial tissue |
|
|
Placenta Accreta occurs in how many deliveries? |
1:2500 |
|
|
Placenta Increta |
placenta extends into myometrium |
|
|
Placenta Percreta |
placenta penetrates uterine serosa (outside) |
|
|
Know how to differentiate Placenta Accreta / Increta / Percreta *see image |
|
|
|
2 Risk Factors for Placenta Accreta |
- placenta previa - Hx of prior uterine surgery |
|
|
What percent of women with 1 prior c-section will develop Placenta Accreta? |
25% |
|
|
What percent of women with more than 2 uterine surgeries will develop Placenta Accreta? |
45% |
|
|
U/S Evaluation of Placenta Accreta |
- absence of hypoechoic subplacenta venous channels - myometrium below placenta |
|
|
What might you see on U/S with Placenta Percreta? |

placental vessels extending into maternal urinary bladder |
|
|
Succenturiate Placenta |

presence of more than 1 accessory lobes - connected by blood vessels to placenta |
|
|
With Succenturiate Placenta, what do the additional lobes have a tendency to develop? |
- infarcts & necrosis - 50% - previa |
|
|
With Succenturiate Placenta, what may happen during delivery? |
additional lobes may get 'left behind' - can cause hemorrhage & infection |
|
|
U/S of Succenturiate Placenta |

*discrete lobe w/ placental appearance - Doppler to see vessels connection lobe to placenta |
|
|
Circumvallate Placenta - what does it result in? |
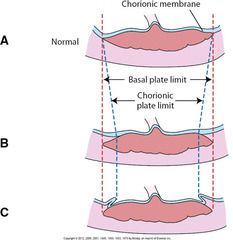
attachment of placental membranes towards center (fetal portion) rather than to the placental margin **RESULTS in villi that are NOT covered by chorionic plate |
|
|
U/S of Circumvallate Placenta |
placental margin appears... - folded - thickened - elevated - fibrin & hemorrhage underneath |
|
|
Circummarginate Placenta |
same as Circumvallate but placental edges are NOT affected |
|
|
Bi-Lobate Placenta |
placenta has 2 equal lobes connected by placental tissue |
|
|
Subchorionic Hemorrhage AKA Implantation Bleeds AKA Submembranous Hematomas |
accumulation of blood beneath chorion |
|
|
U/S of Subchorionic Hemorrhage |

depends on age of bleed... |
|
|
What should be seen on a follow-up exam for a Subchorionic Hemorrhage? |
should have decreased in size |
|
|
When can Subchorionic Hemorrhage be seen? |
early as 9 weeks |
|
|
Why is Subchorionic Hemorrhage referred to as 'Implantation Bleed' ? |
as GS grows and pushes on the hematoma, blood is slowly pushed out - noted as brownish/red spotting in 1st tri |
|
|
Chorioangioma |
blood vessel (angiomatous) tumor that grows from placenta |
|
|
U/S of Chorioangioma |
- hypoechoic, well-circumscribed placental mass - possib near cord insertion site |
|
|
If Chorioangioma is seen, what should fetus be scanned for evidence of? |
high-output heart failure - distension of umbilical vein or R atrium |
|
|
Advanced U/S fetal finding with Chorioangioma |
fetal hydrops - pleural - pericardial - intraperitoneal - subcutaneous |
|
|
Abruptio Placenta |
premature seperation of placenta from uterine wall |
|
|
What occurs in ALL cases of Placental Abruption? |
BLEEDING |
|
|
2 Types of Placental Abruption |
1. Concealed 2. External |
|
|
Concealed Placental Abruption - 20% of cases |

hemorrhage is confined to uterine cavity - detachment may be complete - SEVERE consequences - able to dx via U/S |
|
|
External Placental Abruption |
detachment not usually as severe - PAINFUL vaginal bleeding - if no blood remains in retroplacental space - NOT able to dx via U/S |
|
|
Signs / Symptoms of Placental Abruption |
*** PAIN - Spastic uterus - Fetal distress - Hypovolemic Shock - Trauma - Disseminated Intravascular Coagulopathy (DIC) - formation of small blood clots throughout vessels of body |
|
|
U/S of Placental Abruption |

- elevation of placenta from uterine wall - retroplacental anechoic / complex mass without blood flow - may appear normal or thickened |