![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
33 Cards in this Set
- Front
- Back
|
Why would someone with lower extremity conditions (Ex: total hip joint replacement) need to be checked for shoulder problems? |
People with LE conditions use their arms more to lift things (such as lifting themselves off a chair), which lead to UE shoulder issues. |
|
|
What bones make up the shoulder girdle?. |
Humerus, clavicle and scapula |
|
|
Describe scapular movement with shoulder flexion, through various degrees of movement with the motion |
- GH movement (0-60 degrees) - Scapulothoracic movement (60-140 degrees): "middle/critical phase) - GH movement (140-180 degrees) |
|

- What is this called? - What muscle is likely weak |
- Scapular winging - Serratus Anterior |
|
|
- When is immobilization a good recommendation for someone suffering from shoulder pain? WHY? |
- ONLY with humeral fracture, or post-surgical, otherwise immobilization will increase shoulder stiffness. (SLINGS ARE NORMALLY BAD) |
|
|
Posture and the Shoulder - What does rounded shoulders cause? How is this corrected? - What does a forward head posture cause? How is this corrected? |

- Weakness in rotator cuff over time/Cuff must be strengthened - Cervical and shoulder dysfunction/Strengthen cervical retractors and extensors |
|
|
- What happens if the shoulder becomes too flexible? - What happens if the shoulder becomes too stable? - If a shoulder is too flexible, what should an OT consider? |
- Becomes unstable (can lead to soft tissue tears) - Frozen shoulder |
|
|
What types of diagnostic imaging is available for the shoulder? What are the benefits/drawbacks? |
1.) X-ray: Can show misalignment of bones and arthritis, but does not show soft tissue abnormalities 2.) MRI: Best test/expensive, insurance will only order if surgery is likely (typically try therapy before ordering one) 3.) Arthrogram- dye is injected/can show bones and soft tissue 4.) Ultrasound |
|
|
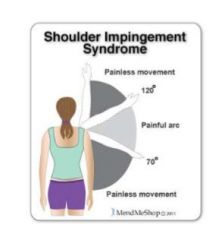
Etiology/Symptoms/Diagnosis Shoulder Impingement |
Etiology: Rotator cuff weakness, causing head of humerus to elevate into joint space and impinge tendons and nerves Symptoms: Anterior-Superior shoulder pain, limited ROM and strength, possible numbless going distally to elbow Diagnosis: Painful arc test & Hawkins-Kennedy Sign |
|
Which test? Desceribe |
Painful arc test |
|

Which test? Describe |
- Hawkins Kennedy - Examiner passively moves patient into shoulder flexion of 90 degrees with internal rotation; anterior/superior pain indicates shoulder impingement |
|
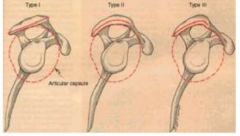
- Which is the worst of the acromion morphology types |
- Type 3 - it is hooked down so it can impinge structures and scrape bones |
|
|
Etiology/Symptoms/Diagnosis Shoulder Arthritis |

Etiology: Genetic (ex: type 3 acromion), or related to UE overuse Symptoms: Pain in various locations of shoulder, limited ROM and strength, crepitus (crunching sound) during shoulder movement, can include impingement Diagnosis: X-ray can confirm: Can see misalignment of GH, or bone spur under acromion, which can deteriorate cartilage/tendons (appearance of string cheese) |
|
|
Etiology/Symptoms/Diagnosis Rotator Cuff Tendonitis |
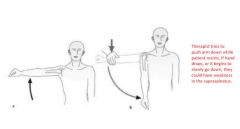
Etiology: Overuse of rotator cuff, usually from repetitive lifting (especially overhead). Can also occur as a result of other shoulder injuries. Most often supraspinatus is affected. Diagnosis: Drop arm test and palpation of other tendons Symptoms: Pain over tendon site, limited ROM and strength when muscle is used. |
|
|
Etiology/Symptoms/Diagnosis Rotator Cuff Tear |
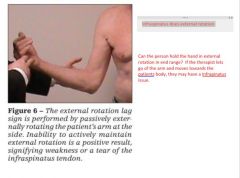
Etiology: Trauma and/or bone spur under acromion from arthritis Symptoms: Mid-deltoid pain, edema, limited ROM and strength Diagnosis: Can be identified by external rotation lag sign (infraspinatus) and internal rotation lag sign (subscapularis) - can be hard to identify |
|
|
Describe a external rotation lag sign
|
|
|
|
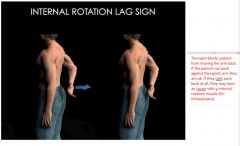
Describe internal rotation lag sign
|
|
|
|
Etiology/Symptoms/Diagnosis Labral Pathology |

Etiology: trauma/dislocation to GH Symptoms: Weakness, limited ROM, sharp momentary pain somewhere in arc of motion, pain in circle around GH, instability of joint Diagnosis: Crank test |
|
|
Etiology/Symptoms/Diagnosis GH Dislocation |
Etiology: Trauma, normally anterior (most common) or posterior. Symptoms: "My shoulder popped out", weakness, edema, limited ROM, tendency to dislocate at 90 degrees abduction and full external rotation Diagnosis: Apprehension (patient is afraid to move shoulder), than relation tests NO DEMO |
|

Etiology/Symptoms/Diagnosis Acromioclavicular (AC) Dysfunction (pic is a grade III AC separation) |

Etiology: Usually trauma, AC can be dislocated, separated or has poor alignment Symptoms: Pain with horizontal adduction, edema, limited ROM, tenderness w/ active compression of AC Diagnosis: Cross arm test + painful palpation |
|
|
Etiology/ Symptoms/Diagnosis
Biceps Tendonitis |
Etiology: RC dysfunction, overuse and/or excessive lifting. Also occurs as a consequence of supraspinatus tendonitis, RC weakness/dysfynction.
Symptoms: Weakness and EXTREAME pain over the tendon located in bicipital groove. Pain during limited shoulder AROM. Diagnosis: Speed's Test & Palpation of bicepts tendon to identify |
|
|
- What is the Speeds Test? - What does it check for? |

- Biceps tendonitis |
|
|
Etiology/Symptoms/Diagnosis Adhesive Capsulitis |
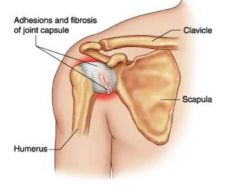
Etiology: "Frozen Shoulder"-scar tissue tigthens shoulder capsule- Painful injury of shoulder followed by voluntary immobilization and/or non-use, Symptoms: Shoulder pain and poor AROM and PROM (AROM = PROM), edema Diagnosis: |
|
|
- What occupational performance areas will a OT likely assess with shoulder dysfunction? (7) |
1 ADL/IADL Independence and History 2 Work/leisure history (Ex: repetitive lifting) 3 Health history and diagnostic imaging 4 PROM/AROM
5 Strength (MMT) 6 Posture 7 Sensation (especially numbness and pain) |
|
|
- What is the key concept of OT shoulder rehab - Provide example |
- Treatment is dictated by patients deficits. Understand underlying problems to resolve symptoms. - Ex: If patient has difficulty with shoulder internal rotation. Is subscapularis weak? Is pec minor too short? |
|
|
- What is staging? - How do you stage? |
- Treat inflammation before you begin strengthening - Staging
|
|
|
Common features of:
|
|
|
|
- How is cervical nerve impingement related to shoulder dysfunction - How do the two present themselves differently? |
- Many patients develop cervical nerve impingement as a result of shoulder dysfunction (or vice-versa). - Patterns of pain are different. UE Numbness is more common when cervical spine is involved |
|
|
- Which frame of reference is most often used to treat and assess shoulder dysfunction |
- biomechanical frame of reference - approach is consistent with deficits and precautions are followed to prevent further injury |
|
|
- What is a general rule of shoulder treatment |
- Exercise and ROM should be limited to 90 degrees and below, due to likelyhood of shoulder impingement and cervical compensatory patterns (UT) - Above the shoulder exercises should only be used towards the end of treatment when pain is minimal and patient isint waking up during the night as a result of pain |
|
|
OT Interventions: Shoulder Dysfunction Manual Therapy Types (4) |
|
|
|
OT Interventions: Shoulder Dysfunction 1. Neuro-Reducation -Types (4) 2. Therapeutic exercise - Types (3) 3. Therapeutic Activity - describe/example 4. Self care retraining - describe 5. Physical agent modalities (7) 6. Adaptive equipment - NONE 7. Kinesiotaping - none |
1. Nerve glides, postural re-education, coordination exercises, nerve mobilization 2. Stretching (for decreased ROM), active range of motion and strengthening 3. Functional activity with multiple parameters (Ex: throwing a ball) 4. ADL activities to increase independence 5. Ultrasound, iontophoresis, electrical stimulation, fluidotherapy, paraffin bath, cold laser, vasocompression |
|
|
- How to know when patient is progressing in treament (4) - What do you do if patient is not improving |
- Demonstrates greater ROM and MMT - States pain score is lower than previously - No longer requires relieving modailities - Meets functional goals set initially - Patient may need referral to orthopedic surgeon |