![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
295 Cards in this Set
- Front
- Back
|
is warfarin a prodrug? |
no |
|
|
a combination product that is only used for ischemic stroke prevention? |
aggrenox 25 mg instant release aspirin 200 mg extended release dipyridamole |
|
|
aspirin MOA? |
irreversible acetylation of serine #529 residue of COX |
|
|
constitutive activity, cytoprotective to GI tract, inhibits thromboxane A2 synthesis are characteristics of? |
COX-1 |
|
|
inducible with inflammation describes? |
COX-2 |
|
|
↓ gastric mucosal barrier, ↓ Prostaglandin Synthesis, ↓ Mucus/Bicarbonate Secretion, ↓ Gastric Cellular Energy, ↓ Submucosal Blood Flow, ↓ Mucosal ATP, ↓ Cell Turnover, ↓ Platelet Function (Irreversible via inhibition ofCOX-1) are all examples of? |
GI tract toxicity associated with aspirin use |
|
|
relationship between aspirin dose and admission for ulcer bleeding? |
proportional |
|
|
aspirin loading dose?
|
160-365 mg/day |
|
|
aspirin maintenance dose? |
75-160 mg/day |
|
|
AHA/ACC aspirin recommendations? |
men only, diabetes, intermediate risk (>10%/10 years), no bleeding risk |
|
|
European Society of Cardiology aspirin recommendations? |
no aspirin |
|
|
primary aspirin intervention? |
75-160 mg/day |
|
|
dipyridamole |
oral antiplatelet |
|
|
sulfinpyrazone |
oral antiplatelet |
|
|
secondary aspirin intervention? |
160-365 mg stat. plain, chewed |
|
|
when is secondary aspirin intervention warranted? |
acute MI, ischemic stroke |
|
|
GI tract bleeding is a toxicity commonly related to which antiplatelet medication? |
aspirin |
|
|
two types of aspirin sensitivity? |
immune and non-immune |
|
|
aspirin risk for those 21 yo or less? |
Reye's syndrome |
|
|
aspirin's effect on the kidneys? |
nephropathy |
|
|
kidney issues associated with analgesics? |
papillary necrosis, decreased GFR |
|
|
rhinorrhea, nasal congestion, cough/wheezing, hives/rash/urticaria are all signs of? |
aspirin sensitivity |
|
|
asthmatics, those with nasal polyps (especially multiple), chronic urticariacs, those with angioedema, those who have had previous anaphylaxis due to any medication are all at increased risk for? |
aspirin hypersensitivity |
|
|
T/F: aspirin increases the incidence of CHD in high-risk adults? |
false, decreases |
|
|
T/F: aspirin increases the incidence of GI bleeding? |
true |
|
|
T/F: aspirin may increase the incidence of hemorrhagic strokes? |
true |
|
|
platelet therapy regimen for patients with acute coronary syndrome (unstable angina, NSTEMI, STEMI)? |
aspirin + 1 or more other antiplatelets |
|
|
platelet therapy regimen for patients with stents (bare metal, drug-eluting, biodegradable)? |
aspirin + 1 or more other antiplatelets |
|
|
ticlopidine |
1st gen antiplatelet P2Y12 inhibitor |
|
|
clopidogrel |
2nd gen antiplatelet P2Y12 inhibitor |
|
|
prasugrel |
3rd gen antiplatelet P2Y12 inhibitor |
|
|
which antiplatelet drug is a cyclopentyltriazolopyrimidine? |
ticagrelor P2Y12 inhibitor |
|
|
which antiplatelet drug is FDA approved for treatment of BOTH ACS and prevention of acute CV events following an MI, stroke, or peripheral arterial disease? |
clopidogrel |
|
|
which P2Y12 inhibitor exhibits reversible binding to its receptor target? |
ticagrelor |
|
|
which P2Y12 inhibitor is mostly cleared fecally rather than renally? |
ticagrelor |
|
|
which P2Y12 inhibitor exhibits significant drug interactions or genetic polymorphisms? |
ticlopidine |
|
|
P2Y12 inhibitor MOA? |
irreversible (except ticagrelor) inhibition of ADP activation site on platelets? |
|
|
which is faster onset: clopidogrel or ticlopidine? |
clopidogrel (hours) ticlopidine (days) |
|
|
which antiplatelet medication has a boxed warning regarding neutropenia/agranulocytosis, thrombocytopenia as thrombotic thrombocytopenia purpura, and aplastic anemia? |
ticlopidine |
|
|
which is more potent: clopidogrel or ticlopidine? |
clopidogrel |
|
|
clopidogrel dosing? |
75 mg/day 300-600 mg/day loading dose |
|
|
ticlopidine dosing? |
250 mg BID with meals |
|
|
which drug is an irreversible thienopyridine P2Y12 inhibitor? |
prasugrel |
|
|
prasugrel dosing? |
loading dose (bolus): 40-60 mg maintenance dose: 5-15 mg/day |
|
|
prasugrel indication? |
ACS patients contemplating PCI |
|
|
for which antiplatelet drug are the following claims made: more consistent and thorough platelet inhibition, faster, 32% increase in severe or major bleeding? |
prasugrel |
|
|
how is prasugrel activated? |
via a 1-step metabolism to the active compound (mostly CYP 3A4) |
|
|
prasugrel best responders? |
males, stented patients, diabetics, less than 65 yo, ClCr > 60 ml/min |
|
|
prasugrel not beneficial or detrimental to? |
strokes/transient ischemic attacks, < 65 kg, > 75 yo |
|
|
antiplatelet affected most by polymorphism? |
clopidogrel |
|
|
antiplatelet affected least by polymorphism? |
prasugrel |
|
|
bleeding tendency higher with clopidogrel or prasugrel? |
prasugrel |
|
|
which drug commonly interacts with clopidogrel and reduces its conversion to its active metabolite? |
omeprazole PPI |
|
|
ticagrelor dosing? |
180 mg loading dose 90 mg BID maintenance dose |
|
|
typical of dosing of antiplatelets? |
loading dose followed by maintenance doses |
|
|
ticagrelor vs. clopidogrel: lower death rate? |
ticagrelor |
|
|
how can platelet aggregation be tested in vitro? |
electrical impedence, light (platelet aggregometry) |
|
|
ADP binding to platelets triggers? |
aggregation |
|
|
this drug exhibits efficacy without bleeding, is reversible within 48hours, works faster, has a greater % of inhibition, and is more consistent than clopidogrel? |
ticagrelor |
|
|
dyspnea, asymptomatic ventricular pauses, no use of aspirin at greater than 100 mg/day are all concerns with? |
ticagrelor |
|
|
elinogrel dosing? |
10-60 mg po or iv reversible |
|
|
vorapaxar and atopaxar are both? |
PAR-1 inhibitors |
|
|
which drug is a synthetic analog of himbacine, the Australian magnolia? |
vorapaxar |
|
|
vorapaxar dosing? |
10-40 mg PO loading dose 0.5-2.5 mg/day PO maintenance dose |
|
|
vorapaxar half life? |
really long 159-311 hours |
|
|
vorapaxar MOA? |
inhibition of PAR-1 to prevent platelet activation |
|
|
indicated for intermittent claudication, pain in calf, peripheral arterial disease? |
cilostazol |
|
|
cilostazol dosing? |
100 mg BID separate from meals (30 min before, 2 hours after) |
|
|
cilostazol MOA? |
PDE 3 inhition > increase in cAMP can cause tachycardia |
|
|
cilostazol contraindication? |
chronic heart failure |
|
|
abciximab |
GP IIb/IIIa inhibitor parenteral antiplatelet for ACS with PCI |
|
|
eptifibatide |
GP IIb/IIIa inhibitor parenteral antiplatelet for ACS |
|
|
tirofiban |
GP IIb/IIIa inhibitor parenteral antiplatelet for ACS |
|
|
apcitide |
GP IIb/IIIa inhibitor for acute DVT |
|
|
when are GP IIb\IIIa inhibitors given to people with ACS? |
not with fibrinolytics, before diagnostic angiography, immediately after PCI |
|
|
GP IIb\IIIa inhibitors most effective in those with? |
high troponin, recurrent ischemia, diabetics |
|
|
anticoagulants that can be used concurrently with GP IIb\IIIa inhibitors? |
UFH, enoxaparin, fondaparinux, bivalrudin |
|
|
absolute contraindication to use of GP IIb\IIIa inhibitors? |
current bleeding |
|
|
beraprost |
prostacyclin derivative oral |
|
|
epoprostenol |
prostacyclin derivative |
|
|
treprostinil |
prostacyclin derivative |
|
|
prostacyclin derivative effects? |
vasodilation (pulmonary HTN), prevents platelet aggregation, anti-proliferative to vascular smooth muscle |
|
|
prostacyclin indications? |
early stage primary pulmonary HTN early stage PVD |
|
|
diarrhea, jaw pain, headaches, and flushing are all very common side effects associated with? |
prostacyclin derivatives |
|
|
thrombolytics WITHOUT fibrin specificity? |
streptokinase anistreplase |
|
|
thrombolytics WITH fibrin specificity? |
urokinase, alteplase, reteplase, lanoteplase, tenecteplase |
|
|
responsible for activated plasminogen to plasmin? |
t-PA |
|
|
optimal plasminogen to plasmin conversion time in the event of an ischemic stroke? |
3 hours |
|
|
optimal plasminogen to plasmin conversion time in the event of an MI? |
6 hours |
|
|
optimal plasminogen to plasmin conversion time in the event of a catheter occlusion? |
24 hours |
|
|
which thrombolytic drug exhibits antigenicity? |
streptokinase |
|
|
which thrombolytic drug activates plasmin indirectly? |
streptokinase |
|
|
which thrombolytic drug exhibits resistance to plasminogen activator inhibitor? |
tenecteplase |
|
|
which thrombolytic drugs are indicated for STEMI? |
streptokinase, alteplase, reteplase, tenecteplase |
|
|
which thrombolytic drug is indicated for STEMI, ischemic stroke, pulmonary embolism, and central venous access device? |
alteplase |
|
|
cheaper, more antigenic, higher lytic state describes which type of thrombolytic drugs? |
fibrin non-specific |
|
|
costlier, quicker and more thorough onset, less bleeding tendency describes which type of thrombolytic drugs? |
fibrin specific |
|
|
which antiplatelet medication has weight based dosing? |
tenecteplase |
|
|
fibrinolytic enzyme derived from the venom of agkistrodon contortix? |
fibrolase |
|
|
alfimprase |
direct fibrinolytic derived from snakes |
|
|
direct fibrinolytic, not plasminogen dependent, can lyse large clots in 1-4 hours, lytic activity confined to site of drug delivery, not inactivated by PAI-1, no systemic lytic state at clinically relevant doses, potentially less bleeding? |
alfimeprase |
|
|
epsilon-aminocaproic acid |
thrombolytic antagonist binds to fibrin sites of plasmin |
|
|
tranexamic acid |
thrombolytic antagonist binds to fibrin sites of plasmin |
|
|
aprotinin |
thrombolytic antagonist broad spectrum protease inhibition |
|
|
drug used to treat heavy menstrual periods? |
tranexamic acid |
|
|
which drug was recently found to double the risk of kidney failure and cause other serious adverse events, including stroke and heart attack? |
aprotinin thrombolytic antagonist |
|
|
atherosclerosis or coronary arteries, vasospasm, plaque rupture, platelet activation and aggregation, thrombogenesis, coronary artery occlusion (complete and partial) are all involved in the pathogenesis of? |
acute MI |
|
|
unexplained fatigue, sleep disturbances, shortness of breath are precursor symptoms of? |
acute MI |
|
|
shortness of breath, very tired, unusual fatigue, pain or discomfort centered high in thechest, weakness, shoulder blade/back pain, nausea, hot, flushed, dizziness, pain or discomfort in the left arm,shoulder, and jaw, coldsweat are symptoms of? |
acute MI |
|
|
differential diagnosis: chestpain or pressure may diffuse and radiate to shoulders, neck, jaw, and arms, pain lasts > 20 minutes and is often accompanied by nausea, dyspnea, or diaphoresis, ST elevations >2 mm, ECGchanges and elevated cardiac enzymes? |
acute MI |
|
|
differential diagnosis: chestpressure or heaviness that may radiate, usually induced by activity andrelieved by rest or nitrates, often has cardiac history and may have ECGChanges (Q-waves, ST, T changes)? |
unstable angina |
|
|
differential diagnosis: painis often sharp in nature, involves multiple locations, and is reproduced withpalpation or respiratory movement, heatoften provides relief, consider traumatic causes? |
costochondritis pain |
|
|
differential diagnosis: mayhave mid-chest pressure and often accompanied with coughing, acid taste in throat, or a choking sensation, usually postprandial and relievedwith antacids, H2 blockers, or proton pump inhibitors, be aware that nitratescan also relieve this pain and can makedifferentiation with angina difficult? |
GERD, esophagitis, and esophageal spasm |
|
|
differential diagnosis: sharpchest pain, dyspnea, cough, and sometimes splinting, consider pleural effusionif patient has diminished breath sounds, dullness to percussion, and decreasedtactile fremitus, chest x-ray will assist diagnosis? |
pleurisy and pleural effusion |
|
|
differential diagnosis: chestpain is usually sharp, retrosternal with sudden onset, it can radiate to trapezialridge, there may be a fever, pericardial friction rub, and arrhythmias such asSVT, ECG may have ST elevations or changes in multiple leads? |
pericarditis |
|
|
differential diagnosis: chesttightness or pressure may be accompanied by nervousness, tachycardia,tachypnea, nausea, diaphoresis, dizziness, and restlessness, ECG, CXR, andlaboratory findings should be negative, therefore a diagnosis can be made through ruling out more serious finding? |
anxiety and panic attack |
|
|
LOCATE acronym? |
location, onset and duration, characteristics, associated symptoms, treatment, eliminates/aggravates |
|
|
CHA2DS2-VASc, high homocysteine, high VEGF, high CRP, high TNF are all predictors of? |
stroke |
|
|
CHADS2-VASc meaning? |
congestive heart failure, hypertension (sys > 160 mmHg), age > 75 yo, diabetes, prior transient ischemic attack or stroke (2 points), vascular disease, age 65-74 years, sex category |
|
|
time is tissue when it comes to? |
ischemic strokes |
|
|
AST acronym for responding to acute ischemic strokes? |
assessment, stabilize, transport (3 to 4.5 hours for total, pre-hospital, door to needle 90 minutes max) |
|
|
assessment portion of acute ischemic stroke response? |
history and circumstances, 5 suddens, FAST |
|
|
5 suddens of ischemic stroke? |
weakness, speech impairment, visual changes, dizziness, severe headache |
|
|
FAST acronym for stroke? |
face drooping, arm weakness, speech difficulty, time to call 911 |
|
|
SCAB acronym? |
stabilization, circulation, breathing, airway |
|
|
the Glasgow Coma, NIHSS, Canadian Neurological Scale, and LA or Cincinnati Stroke Scales are all? |
stroke severity scoring systems |
|
|
door-to-needle goals? |
90 minutes max imaging, comprehensive blood work, severity scoring |
|
|
common problems encountered with victims of stroke? |
hyperglycemia, hyperthermia, hypertension |
|
|
when should TPA fibrinolysis NOT be used in stroke patients? |
if BP > 185/110 |
|
|
quick, objective, easy way to to assess CNS function? |
GCS |
|
|
O2 greater than 94%, intravascular TPA, prophylaxis of DVT with anti-thrombotics, endartectomy if TPA contraindicated, stenting in larger cerebral vessels are all treatments for? |
acute ischemic stroke |
|
|
typical patient characteristic when it comes to ACS? |
middle aged male, elderly, diabetic, prior history or family history of CAD, CVA, PVD (angina, TIAs, intermittent claudication, erectile dysfunction) |
|
|
rapid ER verification of MI? |
12-lead ECG |
|
|
delayed ER verification of MI? |
cardiac enzyme profiles |
|
|
can cardiac enzyme/protein profiles tell us whether a heart attack was STEMI or non-STEMI? |
no |
|
|
what is indicated by high troponin? |
recent heart attack |
|
|
how are thrombolytics used in the case of an in-hospital acute MI? |
within 6 hours of onset |
|
|
how are thrombolytics used in the case of an in-hospital ischemic or thrombotic stroke? |
within 3 hours alteplase is the only one that is FDA approved |
|
|
what thrombolytic is used in cases of ischemic or thrombotic strokes that occur in the hospital? |
alteplase |
|
|
what are surgical alternatives to acute MIs that occur in the hospital? |
PCTL angioplasty and CABG |
|
|
shortcomings with balloon angioplasty? |
restenosis, embolization, rupture of blood vessel, infections, can't alleviate blockage |
|
|
type of stent that is used in most coronary arteries? |
balloon expandable stent |
|
|
type of stent that is used in most carotid applications? |
self-expanding stent |
|
|
triggers a healing response that could narrow the vessel after a stent has been placed? |
cracked plaque |
|
|
what sort of stent is used to prevent restenosis due to cracked plaque? |
drug-eluting stent |
|
|
thrombosis 0-24 hours after stent implantation is known as? |
acute stent thrombosis |
|
|
thrombosis 24 hours to 30 days after stent implantation is known as? |
subacute stent thrombosis |
|
|
thrombosis 30 days to one year after stent implantation is known as? |
late stent thrombosis |
|
|
thrombosis one year after stent implantation is known as? |
very late stent thrombosis |
|
|
what are drug eluting stents made of? |
cobalt chromium or stainless steel |
|
|
sirolimus, paclitaxel, everolimus, and zotarolimus are all? |
anti-proliferative agents that are used in drug eluting stents |
|
|
stent characteristics, APT associations, angioplasty-related factors, lesion-related factors, and medical comorbidities are all factors for? |
higher rates of stent thrombosis |
|
|
stent used in BPH? |
Spanner stent |
|
|
oxygen rate for ACS? |
2-4 liters per minute |
|
|
potent analgesics used in treatment of ACS? |
morphine, oxycodone, oxymorphone morphine is vasodilatory |
|
|
potent diuretics used in treatment of ACS? |
furosemide |
|
|
cardiac off-loaders used in treatment of ACS? |
nitroglycerin, nitroprusside also antiplatelet activity |
|
|
stool softener considerations when treating ACS? |
avoid valsalva maneuver and reflexive CV changes |
|
|
low dose beta blockers are used in ACS patients except those with? |
cardiogenic shock, brittle COPD, poorly controlled diabetes |
|
|
fibrinolytics, GP IIb/IIIa inhibitors, and antithrombins are all medications used in acute treatment of? |
acute coronary syndromes |
|
|
antiplatelets, beta blockers, statins, and ACE inhibitors are all medications used in? |
outpatient treatment of acute coronary syndromes |
|
|
cardioselective beta-blockers? |
bisoprolol, metoprolol |
|
|
noncardioselective beta-blockers? |
carvedilol |
|
|
perindopril |
long acting ACE inhibitor (antihypertensive) |
|
|
complex clinical syndrome from any structural/functional cardiac disorder that impairs the ability of the ventricles to fill with or eject blood, other symptoms include: dyspnea, fatigue, and fluid retention? |
heart failure |
|
|
ventricles enlarge but fail in? |
systolic failure |
|
|
ventricles can't relax in? |
diastolic failure |
|
|
factors that contribute to diastolic, systolic, and total heart failure? |
increasing age increasing weight (BMI) increasing A1C/hyperglycemia increasing blood pressure |
|
|
reduced ejection fraction, enlarged heart, neuroendocrine activation, increased ventricular arrhythmias, and shortened life expectancy are all manifestations of? |
congestive heart failure |
|
|
need to add in "deducing strokes" slide from first lecture |
need to add in "deducing strokes" slide from first lecture |
|
|
weakness, easy fatigue, slowed mentation, cardiac cachexia are signs and symptoms of? |
low cardiac output heart failure |
|
|
nocturia, cardiomegaly with tachycardia, cyanosis, and DOT (dyspnea, orthopnea, tachypnea) are signs and symptoms of? |
congestive heart failure |
|
|
who is at risk for HF? |
previous MI survivor, poorly controlled HTN with hypertrophy, DM, abnormal ECG (esp. resting), chronic tachycardia, obesity, heart murmurs, established CAD |
|
|
what are the ABD's of CHF intervention? |
aspirin blockers diet diuretics dilators digoxin or digitalis |
|
|
which drug has a favorable safety profile in elderly heart failure patients? |
nebivolol |
|
|
which drug is indicated for the treatment of stable chronic heart failure (NYHA class II-III) in addition to standard therapy to reduce mortality or cardiovascular hospitalizations? |
nebivolol |
|
|
nebivolol shares pharmacological properties common to which two other drugs? |
metoprolol (beta-1 selectivity) carvedilol (vasodilatory properties) |
|
|
NYHA class I? |
no limitation at ordinary activities |
|
|
NYHA class II? |
slight limitation at ordinary activities |
|
|
NYHA class III? |
marked limitation at ordinary activities |
|
|
NYHA class IV? |
always symptomatic, even at rest |
|
|
what heart failure categorizations replaced the old NYHA categories? |
ACC/AHA |
|
|
ACC/AHA stage A? |
at-risk for HF, no overt damage/symptoms |
|
|
ACC/AHA stage B? |
structural damage w/o symptoms |
|
|
ACC/AHA stage C? |
structural damage with prior/current symptoms |
|
|
ACC/AHA stage D? |
refractory HF with hospitalizations |
|
|
which drug is approved in 71 countries but not yet in the US for treatment of HF? |
nebivolol |
|
|
objectives for CHF patients? |
cure/prolong survival, make pt. asymptomatic and comfortable, increase the NYHA classification (closer to class I?), decrease the # of hospitalizations |
|
|
CHF intervention lifestyle changes? |
limit activity to capacity, reduce weight toward ideal, BMI reduction, control risk factors for atherosclerosis, restrict salt moderately (<3.8 grams, <1.5 grams is better), restrict water (1.5 L/day) |
|
|
which type of diuretic is preferred in CHF if it is effective? |
thiazides |
|
|
GFR for normal renal function? |
120 ml/min |
|
|
GFR for slightly impaired renal function? |
60 ml/min |
|
|
GFR for moderately impaired renal function? |
30 ml/min |
|
|
GFR for severely impaired renal function? |
15 ml/min or less |
|
|
which type of diuretic is wanted for someone with CHF and a GFR of > 30 ml/min? |
thiazide diuretic |
|
|
which type of diuretic is wanted for someone with CHF and a GFR or </= 30 ml/min? |
loop diuretic |
|
|
HCTZ (often in combos), chlorothiazide, bendroflumethazide, methyclothiazide, and polythiazide are all? |
thiazide diuretics |
|
|
chlorthalidone, indapamide, metolazone, quinethazone are all? |
thiazide-like diuretics |
|
|
which drugs are used as add on therapy to improve CHF? |
spironolactone, eplerenone |
|
|
moderately potent, inhibits NaCl (distal convoluted tubule), safe with respect to volume depletion and electrolyte imbalance, HF patients may not respond describes? |
thiazide therapy of CHF |
|
|
what are the potential thiazide toxicities? |
hyperlipidemia hyperglycemia hyperuricemia hypercalcemia hypokalemia (low potassium) hyponatremia hypomagnesiemia hypovolemia photosensitivity in sunlight |
|
|
which thiazide toxicity differentiates it from loop diuretics? |
hypercalcemia |
|
|
furosemide, bumetanide, torsemide, and ethacrynic acid are all? |
loop diuretics |
|
|
which loop diuretic is the poorest choice for treatment of CHF? |
ethacrynic acid |
|
|
what are the peripheral effects of ADH? |
vasoconstriction, fluid retention, ACTH release |
|
|
what are the central effects of ADH? |
learning and memory, social behaviors, autonomic functions |
|
|
ADH is regulated by? |
osmoreceptors and baroreceptors |
|
|
in regards to ADH, which is more potent: volume or osmotic pressure? |
volume |
|
|
conivaptan, tolvaptan, mozavaptan, lixivaptan, and satavaptan are all? |
vasopressin receptor antagonists |
|
|
what effect do the vaptans have? |
decreased platelet aggregation, decreased pressure, improvement/correction of hyponatremia |
|
|
what type of receptor is the vasopressin receptor? |
GPCR |
|
|
V1a receptor activity in cardiomyocytes at low levels of vasopressin? |
+ inotropy or force |
|
|
V1a receptor activity in cardiomyocytes at high levels of vasopressin? |
- inotropy b/c coronary vasoconstriction |
|
|
V1b receptor is responsible for? |
ACTH release from the pituitary is found in the pancreatic Langerhans cells and kidneys |
|
|
adenylyl cyclase with aquaporin-2 to surface as "water pore", free water retention, collecting tubules of nephrons describes which receptor? |
V2 |
|
|
hyponatremia level? |
= 136-138 mEq/L |
|
|
what is euvolemic hyponatremia? |
increase in total body water with constant sodium |
|
|
what is SIADH? |
syndrome of inappropriate ADH secretion |
|
|
causes of SIADH? |
head injuries, stress, drugs |
|
|
hypervolemic hyponatremia? |
same sodium levels, greater total body water |
|
|
causes of hypervolemic hyponatremia? |
cirrhosis, heart failure |
|
|
eplerenone |
mineralocorticoid receptor antagonist |
|
|
pathologic effects of aldosterone? |
inhibits nitric oxide synthesis, increases inflammation and reactive fibrosis, inhibits sympathetic responses, stimulates cardiomyocyte apoptosis |
|
|
increased vascular compliance, re-establishHR variability, increased fibrinolysis, resensitizationof baroreceptors, decreased platelet activation, reduced vascular inflammation, reduced vascular remodeling, reduced ventricular fibrosis, hypertrophy, and remodeling are all benefits of? |
aldosterone inhibitors |
|
|
which MR inhibitor's absorption is increased with food? |
spironolactone |
|
|
which MR inhibitor has a longer half-life: eplerenone or spironolactone? |
eplerenone |
|
|
problems associated with MR inhibitor class of drugs? |
hyperkalemia, gynecomastia, breast pain, drug interactions (inhibition of CYP 3A4) |
|
|
MR receptor antagonist dosing is based on? |
observed concentration of K |
|
|
MR receptor antagonist contraindications? |
SCr > 2.5 mg/dL and/or GFR <30 ml/min |
|
|
drug classes associated with photosensitization? |
anti's, diuretics, hormones, herbs (St. John's Wort) |
|
|
which drug is approved to prevent progression of TIAs to thrombotic strokes? |
ramipril |
|
|
effects of ACE inhibitors? |
decreased central and peripheral vasoconstriction, decreased aldosterone production (systemic), decreased release of ADH, decreased vascular and cardiac growth promotion or remodeling |
|
|
neutropenia, angioedema, proteinuria, fetotoxic and teratogenic are severe toxicities of which drug class? |
ACE inhibitors |
|
|
which two drug classes improve survivability in those with CHF? |
diuretics and ACE inhibitors |
|
|
which ACE inhibitor CANNOT be taken with meals? |
captopril |
|
|
all of the ACE inhibitors are prodrugs except? |
captopril and lisinopril |
|
|
Dr. Smith's favorite ACE inhibitor? |
fosinopril |
|
|
which ACE inhibitor exhibits long action (once daily dosing = increased compliance, lesser reflex changes), and balanced elimination? |
fosinopril |
|
|
what two drugs make up BiDil? |
isosorbide dinitrate and hydralazine |
|
|
how is BiDil used in the treatment of heart failure? |
as an adjunct |
|
|
which ARBs are indicated on-label for heart failure? |
valsartan and candesartan(?) |
|
|
omapatrilat MOA? |
inhibition of ACE, inhibition of neutral endopeptidase (inhibits degradation of ANP which is vasodilatory) |
|
|
omapatrilat uses? |
HTN, CHF |
|
|
side effects of omapatrilat? |
angioedema |
|
|
new dual inhibitor that leads to BP reduction, cardioprotection, nephroprotection and has little associated angioedema as far as we know? |
ilepatril |
|
|
which recently introduced drug is indicated for class II to IV heart failure with reduced ejection fraction? |
sacubitril/valsartan (Entresto) not used in severe renal/hepatic impairment |
|
|
levosimendan |
calcium sensitizer (inotropy) + potassium channel opener (vasodilation) |
|
|
which has a longer half-life: digoxin or digitoxin? |
digitoxin |
|
|
effects of digitalis? |
increased force of contraction delayed conduction through AV node decreased rate of contraction |
|
|
which drug is used for heart failure with atrial tachycardias? |
digitalis |
|
|
anorexia, N/V, diarrhea, visual changes, neurologic changes, and gynecomastia are all symptoms of? |
digitalis intoxication |
|
|
most common cardiotoxicities? |
dysrythmia, heart block |
|
|
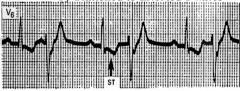
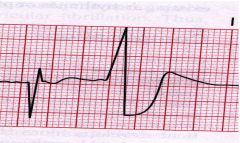
ECG with digitalis |
|
|
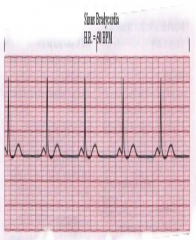
bradycardia due to digitalis toxicity |
|
|
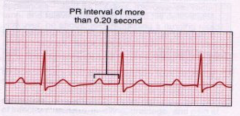
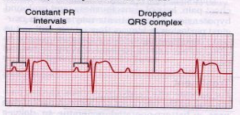
first degree AV block due to digitalis |
|
|
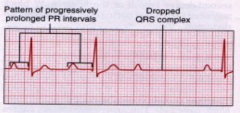
second degree AV block type 1 |
|
|
second degree AV block type 2 |
|
|
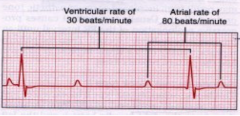
third degree AV block |
|
|
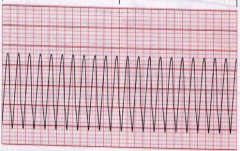
ventricular tachycardia |
|
|
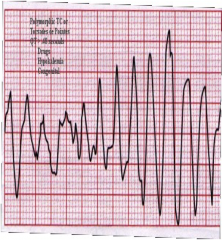
TDP |
|
|
350-440 msec QT interval classification? |
normal |
|
|
450-500 msec QT interval classification? |
potential concern |
|
|
> 500 msec QT interval classification? |
very great risk |
|
|
bigeminy |
|
|
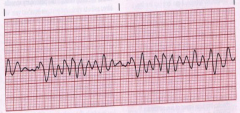
v. fib |
|
|
what to do in cases of mild digitalis intoxication? |
withhold doses until therapeutic/low therapeutic range is achieved, correct electrolytes/pH (low K/Mg, high Ca) |
|
|
digoxin therapeutic range? |
0.5 - 2.0 ng/ml |
|
|
digitoxin therapeutic range? |
10-25 ng/ml |
|
|
what to do in cases of moderate digitalis intoxication? |
same for mild + phenytoin/lidocaine for ventricular dysrhythmias |
|
|
what to do in cases of severe digitalis intoxication? |
DigiBind or DigiFab |
|
|
# vials of DigiBind? |
total digitalis in body (mg) / 0.6 mg/vial |
|
|
# vials of DigiFab? |
total digitalis in body (mg) / 0.5 mg/vial |
|
|
empirical dosing regimen for treating digitalis toxicity? |
10 vials, monitor ECG, repeat after 12-24 hours if symptomatic |
|
|
ancillary medications used to treat digitalis toxicity? |
low dose beta blockers carvedilol, metoprolol, bisoprolol |
|
|
patients with CHF, those who take statins, those who have familial hypercholesterolemia, and >/= 65 years of age need? |
CoQ10 - ubiquinone |
|
|
sources of ubiquinone? |
oily fish, organ meats, whole grains |
|
|
medications used for acute decompensation of CHF (acute worsening)? |
inodilators (amrinone, milrinone) inotropes (dobutamine, dopamine) |
|
|
toxicities associated with inodilators? |
thrombocytopenia, hepatotoxicity, GI tract disturbances |
|
|
problems associated with beta-1 agonists |
proarrhythmic, short-acting, tachyphylaxis, IV admin required |
|
|
novel agent used in the treatment of acute decompensated CHF? |
nesiritide (human, B-type natriuretic peptide) vasodilation natriuresis/diuresis decreased RAAS activation |
|
|
toxicity associated with nesiritide? |
short term, severe hypotension long term renal toxicity with increased mortality |
|
|
used to predict mortality of patients with HF? |
triage BNP test & NT-pro-BNP |
|
|
diagnosis when BNP < 100 pg/ml and NT-proBNP is < 300 pg/ml? |
HF very improbable 2% |
|
|
diagnosis when BNP 100-400 pg/ml and NT-proBNP is > 300 but < 1800 pg/ml? |
ECHO needed to diagnose |
|
|
diagnosis when BNP > 500 pg/ml and NT-proBNP is > 1800 pg/ml? |
HF very probably 95% |
|
|
false positives with BNP tests are common in? |
females, african americans and hispanics, anemiacs, renal diseases |
|
|
false negatives with BNP tests are common in? |
those with obesity |
|
|
which drugs carry a black box warning for causing or exacerbating CHF in some patients? |
thiazolidinediones tioglitazone, rosiglitazone, pioglitazone |
|
|
which diabetes drug is associated with hepatotoxicity? |
tioglitazone |
|
|
which diabetes drug is associated with cardiovascular disease? |
rosiglitazone |
|
|
which diabetes drug is associated with bladder cancer? |
pioglitazone |
|
|
cardiac transplantations, left ventricular assist devices, cardiomyoplasty, ventricular remodeling (the Batista technique) are all? |
advancing heart failure treatment techniques |
|
|
Jarvik 7, CardioWest, and AbioCor are all? |
FDA-approved artificial hearts |
|
|
mydicar |
gene replacement of SERCA2A (removes Ca from cardiomyocyte back into SR) employs adeno-associated viral vector to get into the cardiomyocytes 1 time infusion into coronary arteries phase II CUPID study |
|
|
ixmyelocel-T |
patient specific, expanded multicellular therapy manufactured from the patient's own bone marrow works by increasing repair of damaged heart tissue |