![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
259 Cards in this Set
- Front
- Back
|
What is a co-morbidity? |
An additional disease co-occurring with a primary disease or disorder |
|
|
What are the main effects of co-morbidities on patients? |
Affects life prognosis Increases chances of fatality Increases bed days, disability, hinders rehabilitation, increases chances of decline in aged people |
|
|
What is meant by patient and public involvement? |
The engagement of patients and the public in decisions that affect their and others' health or health care |
|
|
What are examples of patient and public involvement? |
Bold = likely question, designed to trick Voting in an election Choosing your GP/ hospital for surgery Being a non-executive director of a hospital board Representing patient concerns e.g. LINks Responding to patient surveys/ consultations about local health service changes Involvement in decisions about own treatment Involvement in research ('with and by') |
|
|
Approximately what percentage of surveyed patients would like more involvement in decisions about their healthcare? |
40% Doctors believe it is only a minority |
|
|
What is the Elwyn et al (BMJ, 2010) definition of Shared Decision Making? |
An approach where clinicians and patients make decisions together using the best available evidence |
|
|
What are the three main principles of shared decision making? |
Patient well informed (knowledge) Knows what's important to them (values elicited) Decision consistent with values |
|
|
What are examples of preference - sensitive decisions? |
Breast conserving therapy or mastectomy for early breast cancer Repeat c-section or trial of labour after previous c-section Watchful waiting or surgery for benign prostatic hypertrophy Statins or diet and exercise to reduce CVD risk Diet and weight los or medication in diabetes |
|
|
What are the main benefits to Shared Decision Making? |
Improves adherence to medication Better outcomes in supported self-management Reduce unwarranted variation |
|
|
What do patient decision aids do? |
Help patients participate in decision making and make informed choices consistent with their values by presenting the clinical evidence and the likely effects of alternative treatments - Includes risk communication tools, counselling and coaching |
|
|
What are the difficulties with implementing patient decision aids? |
Lack of implementation strategy Time constraints Accessible knowledge Skills and experience Decision support for patients/ professionals Fit into clinical systems and pathways |
|
|
How are statistics used in a clinical setting? |
Prognostic indicators - Different disease characteristics Response to treatment - Different subgroups of patients Clinical trials data - Comparing a new treatment to the current standard treatment |
|
|
What is the difference between hazard and risk? |
Hazard - Anything that can cause harm Risk - Chance someone will be harmed by hazard |
|
|
A risk is a situation involving exposure to danger. What are the 3 common types of risk in a clinical setting? |
Behavioural Health Genetics |
|
|
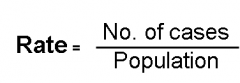
What is absolute risk? |
Absolute measures of risk (prevalence, incidence) Also known as rate Determines rates of disease by person, place or time |
|
|
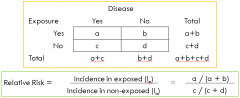
What is relative risk? |
Risk measured relative to something else Compares the risk in two different groups of people Used to identify risk factors for disease |
|
|
What is attributable risk? |
Risk that can be attributed to something Incidence of disease in an exposed group that could be avoided if the exposure was eliminated |
|
|
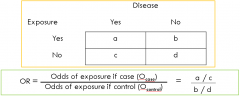
What is an odds ratio? |
Ratio of odds when comparing disease cases to controls Used in case-control studies where incidence can not be calculated |
|
|
What risk ratios would be used in a cohort study? |
Relative risk Odds ratios Relative risk reduction |
|
|
What risk ratios would be used in a randomised control trial? |
Relative risk Odds ratios Relative risk reduction |
|
|
What risk ratios would be used in a case-control study? |
Odds ratio |
|
|
How is absolute risk calculated? |
|
|
|
How is relative risk calculated? |
|
|
|
What does a relative risk >1 indicate? |
There is a positive association - Risk of outcome greater when factor present |
|
|
What does a relative risk =1 indicate? |
There is no association between the exposure and the disease - Risk of outcome unaffected by the presence/ absence of the factor |
|
|
What does a relative risk <1 indicate? |
There is a negative association - Risk of the outcome is greater when the factor is absent |
|
|
What does attributable risk show? |
How many 'extra' cases the exposure has caused = Incidence in exposed (Ie) - Incidence in non-exposed (In) |
|
|
How are odds ratios calculated? |
|
|
|
What does an odds ratio >1 indicate? |
There is a positive association - Exposure is more likely in the cases group |
|
|
What does an odds ratio =1 indicate? |
There is no association between the exposure and the disease - Exposure no more likely in the cases group |
|
|
What does an odds ratio <1 indicate? |
There is a negative association - Exposure is less likely in the cases group (protective effect) |
|
|
How are relative risk and odds ratios interpreted and used? |
Just ratios - tell of strength of association Context is important e.g. RR = 2 means risk is 2x higher in exposed group Association, not causation |
|
|
What are the strengths of the hippocratic oath? |
Contains certain ethical principles still adhered to by doctors today: - Commitment of time to training other doctors - Emphasis places on the good of the patient - Sexual contact with patients is forbidden - Importance of acting within limits of competence - Confidentiality imperative - Physician held accountable for adhering to code |
|
|
What are the weaknesses of the hippocratic oath? |
Some parts controversial/ irrelevant/ outdated/ incomplete: - Giving away money to your teacher, promising to teach medical arts to their sons - Abortion prohibited by code (not by UK law) - Euthanasia expressly prohibited - Not much written about relationship with society or wider justice |
|
|
What are the key components of the Declaration of Geneva (1948)? |
Re-confirms the role of the doctor as a servant to humanity and to first and foremost act for the benefit of the patient Places new emphasis on equality and the importance of doctors not violating human rights of civil liberties 'even under threat' |
|
|
What are the key components of the Nuremberg Code? |
Voluntary consent of human subjects essential Results unprocurable by other methods Anticipated results must justify performance Avoid physical/ mental suffering/ injury Should not perform where prior reason to believe death/ disabling injury will occur Risk < importance of problem Protect subject against injury Only done by the scientifically qualified Subject has option to end early Must be prepared to terminate at any stage |
|
|
What are the key features of the Declaration of Helsinki? |
Similar to Nuremberg code but allows for use of human remains, altering consent from essential to if possible. Introduces approval of ethic committee Must benefit the population taking part in the study to prevent exploitation |
|
|
What are the key features of the Declaration of Tokyo? |
No torture, inhuman/ degrading procedures (no presence/ provision of tools etc.) Confidentiality of information Complete clinical independence No artificial feeding of prisoners that have refused nourishment Support of the physician and their family in the face of threat or reprisals resulting from refusal to condone torture etc. |
|
|
What are the four main professional codes of practice? |
Declaration of Geneva - Patient's health is first priority Nuremberg Code - Voluntary consent of human subject is essential Declaration of Helsinki - Placebo controlled trials, patient's involved in study should have access to benefits Declaration of Tokyo - no torture, forced feeding |
|
|
What are the ethical issues raised in the treatment and care of people with a disability? |
Lack of sensitivity and respect may lead to patronising communication that does not empower patient |
|
|
What is the definition of stigma? |
Marking an individual as different from others, leading to some form of response. Has declined for physical illnesses but increased for mental illnesses - Predominantly shame/ embarassment |
|
|
What are the different ways disability be conceptualised? |
1. Impairment concerns abnormalities in the structure/ functioning of the body 2. Disability concerns the performance or otherwise of activities 3. Handicap refers to the broader social and psychological consequences of living with impairment and disability Consequence of the person's environment |
|
|
What are the basic features of a profession? |
A paid occupation, especially one that involves prolonged training and a formal qualification. Characteristics: - Philosophy of public service, altruism - Skills based on knowledge from research - Education and training prior to practice - Competence testing prior to practice - Explicit code of conduct - Self-regulation |
|
|
What are examples of diseases closely related to occupational exposure? |
Asbestosis Mesothelioma Silicosis Hand arm vibration syndrome |
|
|
What is Occupational Health? |
Interaction/ balance between work and health. Aims to: - Promote, protect maintain health, safety and welfare of staff - Carry out and promote research - Aide rehabilitation and placement where neccessary - Education |
|
|
How does Occupational Health take potential hazards and attempt to prevent/ control risk? |
- Risk assessment - Provision of specialist advice - Environmental protection - First aid and emergency planning - Treatment and provision of clinical services - Business planning and budgeting - Record keeping and reporting |
|
|
What are the main hazards that would be identified by Occupational Health? |
Physical e.g. noise Chemical e.g. fumes/ inorganic gases Biological e.g. body fluids Mechanical e.g. heavy lifting Ergonomic e.g. repetitive work Psychological e.g. lone working, dealing with violence/ aggression |
|
|
What is the impact of illness at work? |
Few conditions are an absolute bar to work, many impose relative reduction in capability but can still be productive with suitable adjustments |
|
|
How should an individuals 'fitness to work' be assessed? |
Functionally, should take into account job requirements and hence capabilities Detailed history, examination, information seeking and workplace assessment should be carried out |
|
|
What are the main causes of sickness absence? |
Multifactorial (e.g. back pain + stress) Musculoskeletal Psychological Respiratory Dermatitis |
|
|
What are the common consequences of prolonged unemployment for the individual (includes absence due to sickness)? |
Greater incidence of depression Decreased mental health (e.g. low self worth) Increased dependency on the state Increase in smoking, alcohol intake, risky sexual behaviour, use of illicit drugs |
|
|
What are the main reasons for telling the truth in a medical context? |
Respects patient autonomy Enhances trust in doctor-patient relationship Not to do so is an abuse of power Avoids complaint/ GMC referral/ lawsuit Would be difficult not to due to MDT Could be dangerous for patient to not know the truth as it has an impact on lifestyle and medication |
|
|
What are reasons for withholding the truth in a medical context? |
Therapeutic privilege - if disclosure would harm physical/ mental well-being Patient waiver - if requested to be withheld Hypotheses - giving every possible diagnosis for example could be information overload Lack of training in breaking bad news Conflict between ethics and protecting patient Requires clinical judgement, not explaining everything and letting patient decide |
|
|
What are acceptable reasons for disclosing information? |
If patient consents Within healthcare team If required by law e.g. infectious disease or through court order (unless irrelevant) If justified in public interest e.g outbreak of disease, if patient is a risk to themselves/ others, if situation with patient could affect others e.g. domestic violence in a home with children |
|
|
Can genetic information about a patient be shared with their family members? |
If justified in the public interest |
|
|
Can information about a patient be shared after their death? |
Only if it would have been during their life |
|
|
What does the GMC require every doctor to do in regards to concerns about colleagues? |
Be honest and open and act with integrity Act without delay if reason to believe a colleague is putting patients at risk Consult a suitably qualified colleague if your performance could be affected by a condition When leading a team deal openly and supportively with problems in the conduct, performance or health of team members |
|
|
What does the GMC require doctors who are managers to do in regards to concerns about colleagues? |
Respond constructively to signs colleagues have health problems - be alive to mental health problems, depression, alcohol dependence Make sure systems are in place to ensure incidents are investigated Protect patients from risk arising from own or colleagues' health |
|
|
What does the GMC require every doctor to do in regards to concerns about trainees? |
Inform Postgraduate Dean, Trust Medical Director and Clinical Director of trainees' drug or alcohol problem Trainees are likely to put themselves on better footing with the GMC if they disclose problems themselves |
|
|
What is Evidence Based Practice (EBP)? |
The conscientious, explicit and judicious use of current best evidence in making decisions about the care of individual patients - At the individual patient (clinical decision making) - At the population level (NICE guidance) |
|
|
What 3 elements make up EBP? |
Evidence i.e. clinically relevant, high quality research, ideally patient-centred, carried out on appropriate populations Clinical Expertise - using clinical skills and judgement with past experience to identify each patient's unique clinical state and risk profile Patient Values - Unique preferences, values, concerns and expectations each patient brings to a clinical encounter, and which must be integrated into clinical decisions |
|
|
What are the main strengths of EBP? |
Increased confidence that decisions are right Useful framework for education Useful vehicle for involving patients in decisions Smooths out variations in care, gives everyone best chance - doctors at same standard Highest quality of care Applies research to patient care Basis of medical legal practice |
|
|
What are the main limitations of EBP? |
Ever changing trends Multi-morbidity Real world validity Robust evidence for many areas of practice lacking/ inconclusive Evidence almost always based on population data Doesn't tailor to individual needs Need for practitioners to develop new skills Searching Critical appraisal Might be seen as a tool for rationing |
|
|
What are the 5 steps of EBP? |
1. Convert need for information into an answerable question 2. Track down the best evidence with which to answer than question 3. Critically appraise that evidence for its validity, impact and applicability 4. Integrate the critical appraisal with own clinical expertise and patient's own model 5. Evaluate effectiveness and seek ways to improve next time |
|
|
What four components do relevant and answerable clinical questions have? |
PICO: Patient and problem Intervention Comparison intervention Clinical Outcomes |
|
|
What are the challenges in applying EBP in the real world? |
Disparity between diagnostic skills and clinical judgement (increase with age/ experience) and clinical performance and up-to-date knowledge (decrease with age/ experience) Problem of not being able to devote more than a few seconds per patient for finding evidence, or setting aside more than a small amount of time each week for further research |
|
|
What might be considered misconduct in research? |
Fabrication Falsification Misrepresentation of data/ interests/ involvement Plagiarism Failures to follow accepted procedures e.g.: - Avoiding unreasonable harm to humans/ animals/ environment - Proper handling of privileged/ private information on individuals collected during research |
|
|
What are the main ethical issues in research? |
Purpose of the research Appropriate design Benefits outweighs harms Informed consent Just selection of subjects Confidentiality Would I take part as a subject? Conflicts of interest |
|
|
What is meant by 'purpose of research' in terms of ethical issues in research? |
Important or trivial? Whose interests are served? - Funding body - Researchers - Research subjects Whose interests are being overlooked? Research needs |
|
|
What is meant by 'appropriate design' in terms of ethical issues in research? |
Is this a technical issue or a technical issue? Resources Equipoise |
|
|
What is meant by 'benefits outweigh harms' in terms of ethical issues in research? |
What is a benefit? To whom? Does a benefit to one outweigh the harm to another? How much harm is acceptable? - MRC and colds - R v Brown Are there any conflicts of interest? Who decides? |
|
|
What is meant by 'informed consent' in terms of ethical issues in research? |
Patient is competent Adequate information is given Information is understood Consent is voluntary and not coerced Consent may be withdrawn at any time |
|
|
What is meant by 'just election of subjects' in terms of ethical issues in research? |
Fertile women Children (questionable legality of consent) Prisoners Mentally impaired Unconscious Students Financial inducement |
|
|
What is meant by 'confidentiality' in terms of ethical issues in research? |
Seek consent where practicable Anonymise Minimise disclosure Obey law |
|
|
What is meant by 'Would I take part as a subject?' in terms of ethical issues in research? |
Damage to health |
|
|
What are Zola's Triggers to consult with a doctor? |
1. Occurrence of interpersonal crisis 2. Perceived interference with social or personal relations 3. Sanctioning 4. Perceived interference with vocational/ physical activity 5. Temporalising of symptomatology |
|
|
What is the definition of a 'professional sector' in medical terms? |
The organised and legally sanctioned part of a healthcare system |
|
|
What are the roles of social workers in healthcare? |
Assessment and access to: - Home care - Meals - Equipment, adaptations - Day services, residential, nursing home care - Individual and carer assessments - Personal budgets, direct payments - Adult safeguarding procedures |
|
|
What is the definition of a 'voluntary sector' in healthcare? |
Organisations that exist to serve a public benefit, are self-governing, do not distribute any profits to members and depend to a meaningful degree on volunteers |
|
|
What are examples of complementary therapy? |
Reflexology Homeopathy Acupuncture Herbalism Osteopathy |
|
|
What are the four types of professionals and services available in the community to support people's health needs? |
Statutory - must be provided by law e.g. NHS Voluntary - Exist to serve public benefit, self-governing, do not distribute any profits Complementary Private e.g. residential homes, private physiotherapists, private home nurses |
|
|
What are the strengths and weaknesses of statutory services? |
Strengths - free to use, official, accountable, high levels of professional knowledge Weaknesses - long waiting times, essential services may be changed or cut, personal can't usually choose who they see |
|
|
What are the strengths and weaknesses of voluntary services? |
Strengths - User feels involved, organisation usually has local knowledge, flexible, usually free to use Weaknesses- Constant fund raising, reliance on volunteers who may be unreliable, may not be well or consistently funded |
|
|
What are the strengths and weaknesses of complementary services? |
Strengths - broad use, some evidence of efficacy of osteopathy and chiropractic, user often gets more time with the practitioner Weaknesses- lack of evidence base for effectiveness, little communication with other health professionals, often costly |
|
|
What are the strengths and weaknesses of private services? |
Strengths - self referral possible, patient 'control', flexible to user needs, should deliver high standards Weaknesses - Cost excluded many, clinicians rarely receive communication re. patient |
|
|
What are the main communication challenges facing multidisciplinary teams? |
Health care staff: - Tend not to adapt communication - Lack understanding and empathy - Often don't recognise stressful nature of healthcare interactions |
|
|
What are the main skills required in the context of communication in healthcare? |
- Making sure patient can see your face, talking clearly, not too fast but not too exaggerated - Never say 'nothing/ never mind/ it doesn't matter' - Writing things down is fine, doesn't cause offence, especially with medical words - Key is patience so the patient doesn't feel stressed or upset about communication |
|
|
What is meant by the health belief model? |
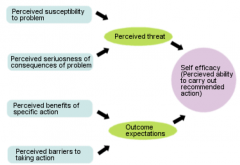
Image |
|
|
What is meant by theory of reasoned action? |
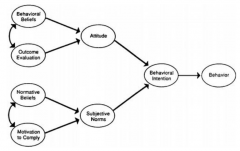
Image |
|
|
What is meant by behaviour change cycle? |
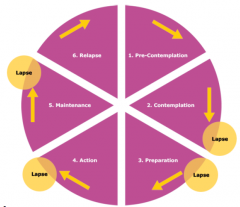
Image |
|
|
What is the WHO definition of health? |
A state of complete physical, mental and social well-being and not merely the absence of disease or infirmity |
|
|
What is meant by the iceberg of illness? |
Doctors won't find out everything about an illness, only the 'tip of the iceberg'. Often refers to things such as mental illness |
|
|
What are some of the key elements of patient self-care? |
Small steps of confidence building actions Goal setting using action plans Learning how to problem solve Reinterpreting your symptoms Develop a toolkit of skills that can be used |
|
|
What is an example of a vicious cycle of symptoms in a long term health condition? |
Long term condition Physical limitations Pain Stress/ anxiety Difficult emotions Depression SOB Fatigue Poor sleep Long term health condition |
|
|
How might patients manage their symptoms in a long term health condition? |
Distraction Expert Patient Programme Positive outlook Action plans |
|
|
What are the main benefits of patient self-management? |
Reducing the severity of symptoms Significantly decreasing pain Improving life control and activity Improving resourcefulness and life satisfaction |
|
|
What five core skills does the Expert Patient Programme teach? |
Problem solving Decision making Making the best use of resources Developing effective partnerships with healthcare providers Taking appropriate action |
|
|
How effective is the Expert Patient Programme? |
Good addition to current services for some individuals but not a solution for all Thought to be cost effective |
|
|
What is public health? |
The science and art of promoting health and preventing disease by the organised efforts of society |
|
|
What is the faculty of public health about? |
Improving and protecting health of groups of people rather than treating individual patients Public health consultants must look at the 'bigger picture' and then take action to promote healthy lifestyles, prevent disease, protect and improve general health, and improve healthcare services |
|
|
What is health promotion? |
The process of enabling people to exert control over, and to improve their health. Health is a positive concept emphasizing social and personal resources as well as physical capacities. Therefore, health promotion is not just the responsibility of the health sector, but goes beyond healthy lifestyles to wellbeing |
|
|
What is Tannahill's model of health promotion? |

- Socio, economic, physical, environmental and cultural factors - Equality and diversity - Education and learning - Services, amenities and products - Community-led and community-based activity |
|
|
What is disease prevention? |
The prevention of disease and associated disability and death by: - Reducing the risk of developing disease in those who are disease free - Identification and management of the early manifestations of disease - prevention of the chronic and disabling effects of disease |
|
|
What are primary, secondary and tertiary methods of disease prevention? |
Primary - reducing risk of disease in disease free Secondary - Identification/ management of early disease Tertiary - Prevention of chronic and disabling effects of disease |
|
|
Why are health promotion and disease prevention important? |
Lots of ill health is avoidable Avoidable ill health is wasteful - unnecessary health care and economic costs Avoidable ill health is not fairly distributed across society |
|
|
What are the evidence based approaches to health promotion and disease prevention? |
Evidence of: - Need (e.g. epidemiology) - Effectiveness (e.g. RCTs) - Safety (side effects?) - Efficiency (Cost-effectiveness) - Equity (Equal effects according to need) - Feasibility (Can it be implemented widely?) - Acceptability (To individuals and society) |
|
|
What is Rose's prevention paradox? |
A preventative measure that brings large benefits to the community offers little to each participating individual |
|
|
What are the main inequalities in health promotion? |
Likely to have a bigger impact on higher socioeconomic groups. Lower groups are less likely to eat healthily/ engage in physical exercise Can be reduced by making promotion (e.g. vaccine) compulsory and an opt-out system rather than opt-in |
|
|
What is health psychology? |
The study of psychological and behavioural processes in health, illness and health care Particular focus on understanding and modifying behavioural, emotional and health outcomes in prevention, treatment and rehabilitation |
|
|
What is Psychoneuroimmunology? |
The study of interaction between psychological processes and the nervous and immune systems of the human body |
|
|
Why is health psychology important in chronic illness? |
- Increase in proportion of illnesses that are chronic e.g. heart disease, diabetes - Many chronic illnesses are associated with 'liefstyle' factors e.g. diet, smoking, alcohol, stress - Increase in 'medically unexplained' symptoms e.g. back pain, chronic fatigue, migraine |
|
|
What are primary preventions of health? |
Lifestyle behaviours - major cause of illness and premature death - 48% avoidable in US? |
|
|
What are secondary preventions of health? |
Patients reduced delay in seeking help, poor adhence to treatment |
|
|
How can health professionals influence behaviour of patients and the general population? |
Implementation of EBP Knowledge transition gap |
|
|
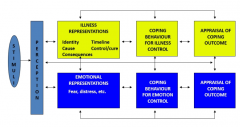
Psychology and chronic illness flowchart |
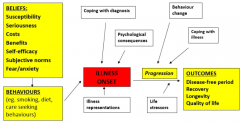
Image |
|
|
Biomedical model of health |
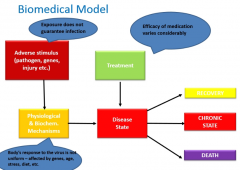
Image |
|
|
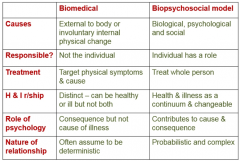
What are the key differences between the biomedical and biopsychosocial models of health? |
|
|
|
Common sense self-regulation model |
|
|
|
What factors are involved in patient coping procedures? |
Identity - label/ symptoms Timeline - acute/ chronic/ cyclic Cause Consequences Cure/ control - options Patients' representations are dynamic Patients are active problem solvers of own health Patients beliefs change with their treatment related and other experiences |
|
|
What is the Theory of Planned Behaviour (TPB)? |
Behaviour is determined by a person's intention, which is in turn defined by 3 factors: - Attitudes ('Doing X would be good for me') - Subjective norms ('friends think') - Perceived behavioural control ('I can do X') |
|
|
What are the limitations of the Theory of Planned Behaviour (TPB)? |
Effective at predicting behaviour but limited value for informing behaviour change interventions because: - Attenuation problem - changes in belief do not always translate to changes in behaviour - Technology problem - TPB does not suggest changes - Bottle-neck problem - Excludes many EBP techniques e.g. self-monitoring - Non-linear problem - interim behaviour gap |
|
|
What is Social Cognitive Theory? |
Behaviour is determined by 3 factors: - Goals - Outcome expectancies (physical, social, self-evaluative) - Self-efficacy |
|
|
What is self-efficacy? |
An individual's belief in their own abilities, and functions as a proximal determinant of: - Behaviour - Thought patterns - Emotional reactions Not a stable personality characteristic |
|
|
What are tips on increasing self-efficacy? |
Mastery - experience of successful performance, achieved by graded tasks (increasing difficulty) Vicarious - observation of someone else performing successfully Persuasion - by nurses/ dieticians/ GPs Psychological/ Somatic - Observation of changes in body while performing task (e.g. after exercise) |
|
|
How can planning improve self-efficacy? |
Proactive self-regulatory strategy In situations with sufficient resources Outside of demaning and risky situations SMART targets |
|
|
What are the roles of the doctor at the societal level? |
Social positions that carry privileges, obligations, rights and expectations Social control - processes that regulate individual and group behaviour in an attempt to gain conformity and compliance to the rules of a given society Consensus and conflict approaches |
|
|
What is Parsons model (consensus approach)? |
The sick role is a temporary social role instituted by society with the aim of returning sick people to fully functioning in society as quickly as possible |
|
|
What are the roles of the patient and doctor in the Parson's model of the doctor-patient relationship? |
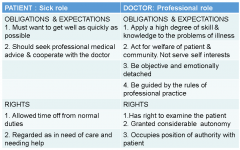
Image |
|
|
What is an example of the Parson's model and what are the potential issues? |
Patient given sick note for back pain, takes every possible action to remedy as wants to return to work ASAP. Doctor decides length of note Issue if no cause for pain is found and patient and doctor disagree on suitability for work Or no work for patient to return to due to high levels of local unemployment |
|
|
What is meant by conflict approaches in terms of the doctor-patient relationship? |
Characterised by a clash of perspectives e.g: - Values (convicted criminal) - Disclosure of information (child safeguarding action) - Social control (mental health act to hospitalise against will) - Managerial control (Dr won't give high cost treatment) |
|
|
What is Iatrogenesis? |
Preventable harm resulting from medical treatment or advice to patients Can be clinical, social or cultural |
|
|
What is clinical iatrogenesis? |
Side effects of medical treatment e.g. bleeding due to Warfarin given for atrial fibrillation to prevent a stroke |
|
|
What is social iatrogenesis? |
Population becoming increasingly dependent on medical treatments e.g. use of hormone replacement treatment in the menopause |
|
|
What is cultural iatrogenesis? |
Reduced ability of people to cope with normal provcesses of life e.g. desire of people to live longer and have all the medical treatments that will so enable |
|
|
What are the four models of the doctor-patient relationship? |
Paternalistic Mutuality Consumerist Default |
|
|
What is the paternalistic model of the doctor-patient relationship? |
High physician control Low patient control Often based on the biomedical model Example: emergency situations |
|
|
What is the mutuality model of the doctor-patient relationship? |
Equal partners Patient centred approach Shared decision making Example: Patient's ICE on antidepressants |
|
|
What is the consumerist model of the doctor-patient relationship? |
High patient control Low physician control Often fee based Doctor's perception of patient pressure important Example: patient wanting very expensive knee replacement so going to see a doctor privately |
|
|
What is the default model of the doctor-patient relationship? |
Neither doctor nor patient takes control Doctor tries to empower the patient Patient doesn't want to take control Lack of engagement |
|
|
Other than the four models, what are other ways of conceptualising the doctor-patient relationship? |
Funtionalists (1960's) - Consensus on roles - a competence hap exists between patients and doctor so accept their roles Conflict theorists (1970's) - Conflict of BM model with lay model regariung underlying disease/ pathology Interpretivists (1980's) - No competence gap, expert patient, doctor expert in diagnosis and treatment |
|
|
What is mental health? |
A state of well being in which every individual realises their potential, can cope with the normal stresses of life, can work productively and is able to make a contribution to his or her community |
|
|
What are the 5 models of mental illness? |
Spiritual e.g. hearing voices, treated by Shaman Medical e.g. physiological/ biochemical/ genetic causes Psychological - failure to adapt to life circumstances/ learning wrong responses Social - dysfunctional interpersonal behaviour or inability to perform sanctioned social role Biopsychosocial |
|
|
What are some issues with mental health definitions? |
Diagnoses are generalisations and simple whereas individuals are unique and complex Depends on doctor's subjective evaluation (need for good communication skills and self awareness) Medicalisation of life and social control |
|
|
What is the range of mental ill health? |
Ranges from stress to severe mental illness Triggers include life events and stressors of significance Changes at different times of life Recovery is possible, including from severe mental illness |
|
|
What is the frequency of mental ill health? |
One of the main causes of the burden of disease worldwide 28% in UK compared to 16% each for cancer, heart disease 1/4 people in UK will experience in any given year, women more likely than men |
|
|
How are common mental health problems such as depression and anxiety distributed across society? |
According to a gradient of economic disadvantage |
|
|
What is the leading cause of sickness absence in the UK? |
Mental ill health (anxiety, depression and stress related conditions) |
|
|
How are frequencies of long term physical and mental health problems linked? |
30% of people with LT physical problem also have mental health problem 46% of people with mental health problem also have LT physical problem |
|
|
How might mental health problems present to a doctor? |

Physical health problems Somatisation Direct presentation Crisis |
|
|
What is social stigma? |
Extreme disapproval of (or discontent with) a person or group on socially characteristic grounds that are perceived, and serve to distinguish them, from other members of a society May then be affixed to such a person, by the greater society, who differs from their cultural norms |
|
|
Are people with mental illness able to work? |
Most people have colleagues with a mental health problem |
|
|
'People with mental health illnesses are looked after and so not usually victims of crime' True or false? |
False. 45% of people with a mental illness have been victims of a crime |
|
|
'Times have changed and now the majority of people with mental health problems don't experience discrimination' True or false? |
False. 90% of people with mental health problems experience stigma |
|
|
What factors tend to increase the proportion of mental ill health and associated stigma? |
Women People who are gay/ lesbian/ bisexual Those with additional disabilities Middle ages, psychiatric patients |
|
|
What are the main impacts of stigma and discrimination? |
Prevents people seeking help Delays treatment Impairs recovery Isolates people Excludes people from day-to-day activities Stops people getting jobs |
|
|
What is the aetiology of depression? |
Interaction of: - Genetic predisposition - Vulnerability factors - Protective factors - Life events |
|
|
What are the 5 levels of presentation and care in relation to mental illness? |
In the community Consulting a GP Diagnosed with mental health problem Contact with psychiatric services Psychiatric in-patient |
|
|
What are the two main systems for classifying mental health? |
International Classification of Diseases (ICD 10) - 10 groups e.g. mood (affective) disorders Diagnostic and Statistical Manual of Mental Disorders (DSM 4) - 297 disorders classified in 5 domains |
|
|
What are the approaches to treatment of mental health problems? |
GP, other members of primary care team, including counsellor Community mental health team Psychotherapists Hospital-based psychiatry services Drug and alcohol services Self-help |
|
|
How are mental health problems treated? |
Prevention and health promotion 'Talking' - approaches from simply listening to in-depth psychoanalysis, CBT Physical - pharmacological, ECT, surgery Support |
|
|
What are the outcomes for mental health problems |
Getting better - changing attitues, newer therapies |
|
|
What is poor outcome for mental health problems associated with? |
Delayed/ insufficient initial treatment More severe illness Older age at onset Co-morbid physical illness Continuing problems with relationships Poor social support |
|
|
What % of sickness absence from work is due to anxiety/ depression? |
17% |
|
|
What are some types of drugs that can cause psychological symptoms? |
Steroids Oral contraceptives Anti-hypertensives Anti-Parkinson's drugs |
|
|
'The global burden of TB is greater than that of mental health problems' True or false? |
False. Mental health diagnoses are greater than TB or cancer` |
|
|
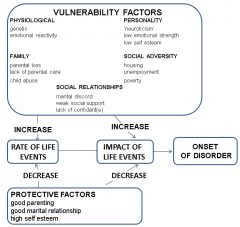
What are the vulnerability factors for mental ill health? |
Physiological - genetic, emotional reactivity Personality - 'neuroticism', low emotional strength, low self esteem Family - parental loss, lack of parental care, child abuse Social Adversity - housing, unemployment, poverty Social Relationships - marital discord, weak social support, lack of confidante |
|
|
What are the protective factors for mental ill health? |
Good parenting Good marital relationship High self esteem |
|
|
Vulnerability/ protective factors for mental health diagram |
Aetiology of depression |
|
|
How are mental health problems presented in a consultation? |
Directly expressed Indirectly expressed Physical manifestations of mental illness Psychological manifestations of physical illness 'Somatic' or 'functional' symptoms Psychological distress due to life stresses Other routes e.g. crisis, screening |
|
|
What is the difference between direct and indirect expression of mental illness? |
Direct - patient explicity says 'i feel depressed' etc. Indirect - disclosed only on direct questioning |
|
|
What are examples of physical manifestations of mental illness? |
Tiredness, poor sleep, loss of appetite in depression Palpitations, chest pain and breathlessness in anxiety |
|
|
What are examples of psychological manifestations of physical illness? |
Anxiety in thyrotoxicosis Lethargy in anaemia Hallucinations and mood changes with brain pathology Also the psychological impact of physical illness |
|
|
What is meant by 'somatic' or 'functional' symptoms of mental illness? |
An illness or symptoms where emotional factors produce physical symptoms, may be linked to stress |
|
|
What are the strengths and weakness of an individual high-risk based approach to health promotion/ disease prevention? |
Strengths - appropriate to individual, patient motivation, physician motivation Weaknesses - spend resources on identifying high risk, medicalise prevention, stigmatise individuals, limited effect |
|
|
What are the strengths and weakness of a whole population based approach to health promotion/ disease prevention? |
Strengths - attacks root causes, powerful level of effect, shifts cultural norms Weaknesses - can be difficult to achieve, benefit is small for each individual |
|
|
What is health education? |
Learning experiences that enable people to increase control over the determinants of health, health behaviours and the conditions that affect their health status |
|
|
What are examples of health education? |
Seminars and workshops in schools, community settings, adult education Individual advice/ counselling from GP, health visitor etc. Advertisements on TV, radio, newsprint Dramas and documentaries on TV, radio Articles in newsprint Leaflets and booklets Posters, billboards, hoardings Stickers, badges, post-marks, stamps etc. |
|
|
What are the twin aims of public health? |
To improve health and prevent disease in the population as a whole To reduce inequalities in health between the best and worst off |
|
|
What are intervention generated inequalities? |
When a public health intervention improves the health of the population as a whole but simultaneously increases inequalities between sub-groups within the population |
|
|
What are the characteristics of interventions likely to increase health inequalities? |
Educational component Rely on voluntary change One-size-fits all Financially regressive (gives advantage to richest) |
|
|
What is the PETeR model for health interventions? |
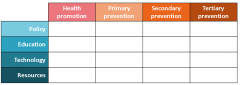
Policy, Education, Technology, Resources |
|
|
What, according to WHO Europe, are the top 5 best practices to reduce alcohol-related harm in populations? (Most cost-effective per DALY saved) |
Increase taxation Screening and brief interventions (SBI) Advertising ban Reduce opening hours (e.g. weekend closing day) Random breath tests for drivers |
|
|
What is meant by healthy public policy? |
Legal or fiscal controls, other regulations and policies and voluntary codes of practice aimed at promoting health or preventing disease |
|
|
What are examples of healthy public policy? |
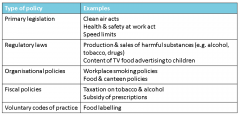
Table |
|
|
What is meant by healthy technologies? |
Any mechanical, chemical, electronic, biological or other technological innovation that can be used to promote health or prevent disease |
|
|
What are examples of healthy technologies? |
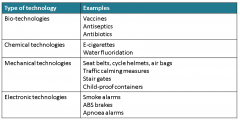
Table |
|
|
What is meant by resources for health? |
Any financial or other reward, or reduction or removal of a financial or other cost, aiming to promote health or prevent disease |
|
|
What are examples of resources for health? |
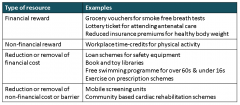
Table |
|
|
PETeR framework for public health interventions (filled) |
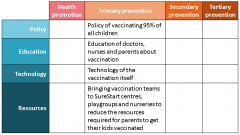
Image |
|
|
Examples of injury prevention using PETeR framework |
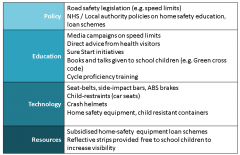
Image |
|
|
What is Making Every Contact Count (MECC)? |
An approach to behaviour change that utilises the millions of day to day interactions that organisations/ people have to encourage changes in behaviour that have a positive effect on the health and well-being of individuals/ communities/ populations |
|
|
What is the purpose of Making Every Contact Count (MECC)? |
Enables the opportunistic delivery of consistent and concise healthy lifestyle information and enables individuals to engage in conversations about their health at scale across organisations and populations |
|
|
What is 'Screening and Brief Intervention'? |
Secondary prevention - identifies incipient problems, often asymptomatic, but potentially responsive to change Case finding (universal or targeted) focused on non-treatment seekers followed by 5-20 minute input - simple structured advice using motivational counselling, provision of clear written information |
|
|
Three key messages about communicating risk and benefit to patients |
- Risk perceptions are influenced by psychological, social and cultural factors - Public risk perceptions which differ from scientific estimates are not eh result of ignorance - Public trust in expert knowledge is easily lost and difficult to regain |
|
|
What is risk? |
The probability that a hazard will give rise to harm |
|
|
What is risk communication? |
The open, two way exchange of information and opinion about risk, leading to a better understanding and better risk management decisions |
|
|
What influences perceptions? |
Personal experiences and beliefs Behavioural norms Myriad of other factors, not least the media Also: immediacy, controllability, novelty, unknown, catastrophic nature |
|
|
What is availability bias? |
People judge an event as more likely or possible if it is easily brought to mind e.g. more dramatic events |
|
|
What is conformation bias? |
People tend to look for confirming evidence (rather than disconforming) to support a belief |
|
|
What are the best ways to communicate risk in terms of numbers? |
Most people prefer numbers to categories such as high/ low People understand natural frequencies better than percetages e.g. 3 out of 10 is better than 30% Numeracy levels in general population are variable e.g. 1 in 25 or 1 in 250, which is greater risk? |
|
|
What are the general principles for communicating risk? |
Should be as simple as possible and responsive to individual needs More information generally leads to greater awareness Most effective when: takes place in context of trust, there are choices (if possible) and information is individualised e.g. cardiovascular risk calculators |
|
|
What are the best methods to communicate risk? |
Framing - use positive as well as negative e.g. 8/10 live Absolute risk vs relative (absolute is generally smaller) Convert odds to frequencies, use consistent denominators, avoid vague descriptive terms, relate to everyday events |
|
|
What are the seven simple strategies for helping patients understand risks? |
- Learn about the difficulties that patients have understanding risk - Accept that patients emotions will filter the facts and cannot be ignored - Revise the way you explain risk - Try to avoid using the concept of relative risk - Give positive as well as negative perspective - Use visual aids - Realise that sharing visual aids etc. enhances the doctor-patient relationship |
|
|
Behavioural Change Cycle (image) |

Image |
|
|
What is the value of the Cycle of Change model for behaviour? |
- Individuals are more or less receptive depending on their state of change - Acknowledges resistance to change - Assess stage of change: HCP is facilitator - offers help, information - Offering the wrong intervention at any stage is counterproductive |
|
|
What are the 6 stages of the Behaivoural Change Cycle? |
Precontemplation Contemplation Preparation Action Maintenance Relapse |
|
|
What is the precontemplation stage of the Behavioural Change Cycle? |
Patient does not want to change behaviour - it is acceptable, a social norm (health belief) or other priorities |
|
|
What is the contemplation stage of the Behavioural Change Cycle? |
Thinking about change, not yet ready, apprehensive. May accept information |
|
|
What is the preparation stage of the Behavioural Change Cycle? |
Ready to change, plan to do so soon, need help with problem solving and practical support e.g. NRT |
|
|
What is the action stage of the Behavioural Change Cycle? |
Actively quitting the behaviour, need follow up and support e.g. nurse-led quit smoking clinic |
|
|
What is the maintenance stage of the Behavioural Change Cycle? |
Maintaining change, needs support and reinforcement to prevent relapse |
|
|
What is the relapse stage of the Behavioural Change Cycle? |
Have gone back to the behaviour they sought to change |
|
|
What is motivational interviewing? |
A collaborative conversational style for strengthening a person's own motivation and commitment to change |
|
|
What are the 5 principles of motivational interviewing? |
Express empathy (reflective listening, explicit) Develop discrepancy (find their thoughts - assumes internal dialogue of pros vs cons) Avoid argumentation (don't let them say can't) Roll with resistance (search for common ground) Support self-efficacy (ask to remind of what has worked in the past, what they can achieve) |
|
|
How might a GP support self-management in COPD? |
Signpost to smoking cessation Early recognition and coping with symptoms Prompt access to treatments in axacerbation Support for exercise and pulmonary rehab Supply information - do not advise - facilitator not teacher |
|
|
Which health promotion interventions influence the number of smokers? |
Taxation (main) - especially in low income areas Advertising Smoking bans Pack labelling and health warnings NHS Quit Smoking Service |
|
|
What are the difficulties with Shared Decision Making (SDM)? |
Lack of implementation strategy Time constraints Accessible knowledge Skills and experience Decision support for patients/ professionals Fit into clinical systems and pathways |
|
|
What are the agendas of the patient and doctor during a consultation? |
Patient - ideas, concerns, expectations, feelings Doctor - symptoms, signs, investigations, patho-physiology |
|
|
What is clinical reasoning? |
The process by which a clinician sorts through and evaluates the cluster of features presented by a patent and assigns a diagnostic label or problem formulation, the goal being development of an appropriate, patient-centred and where possible evidence-based management strategy |
|
|
What are the reasons for making a diagnosis? |
So appropriate treatment can be given/ preventative action taken To be able to give a prognosis Labelling/ naming the problem Medico-legal reasons Intellectual satisfaction Research, audit, teaching |
|
|
What are the four main types of diagnosis? |
Pathological - e.g. diabetes mellitus Clinical - e.g. acute asthma attack Differential - e.g. SOB on exertion, abdominal pain Functional/ formulation (psychiatry) - e.g. unhappy child with tummy pains, headaches and school refusal |
|
|
What are the two main cognitive strategies doctors use? |
Pattern recognition - fast, automatic, frequent, emotional, stereotypic, subconscious Analytical approach - slow, effortful, infrequent, logical, calculating, conscious |
|
|
How does pattern recognition work in diagnosis? |
Presenting complaints elicited Small number of hypotheses formed (2/3) Validated/ rejected by selective questioning, selective physical examination, selective investigations |
|
|
What is the systematic approach to diagnosis? |
Full history Thorough examination Comprehensive investigations Diagnosis |
|
|
Why is the systemic approach to diagnosis important? |
Important for novices Medico-legal pressures Works when things are puzzling |
|
|
What are the limitations of the systematic approach to diagnosis? |
Cumbersome: - Can be wasteful, even dangerous - Overdiagnosis is a major focus of current concern |
|
|
How is the algorithmic approach to diagnosis used? |
Paramedics' protocols Nurse triage Clinical guidelines Non-experts in straightforward situations e.g. swine flu, rural health aid in developing world |
|

What type of headache is shown in the image? |
Sinus - pain usually behind the forehead and/ or cheekbones |
|

What type of headache is shown in the image? |
Cluster - pain is in and around the eye |
|

What type of headache is shown in the image? |
Tension - pain is like a hand squeezing the head |
|

What type of headache is shown in the image? |
Migraine - pain, nausea and visual changes are typical of classic form |
|
|
What are the serious causes of headache (red flags)? |
Subarachnoid haemorrhage - 'thunderclap' sudden onset, usually occipital, neck stiffness Meningitis - flu-like prodrome, fever, photophobia, neck stiffness with/ without rash Raised intracranial pressure - history of injury/ worse on a morning, worse on leaning forwards, present all/ most of the time |
|
|
What is fainting? |
Brief loss of consciousness due to momentary reduction in blood flow to the brain |
|
|
What are the causes of fainting? |
Reaction to pain or fear, emotional upset, exhaustion, lack of food, prolonged standing in warm atmospheres |
|
|
What are the symptoms of fainting? |
Pulse may be slow and weak Looking pale Low BP Some patients can twitch and jerk |
|
|
How can fainting be prevented? |
If feeling faint, sit down head between knees OR Lie down, deep breaths |
|
|
How is fainting treated? |
Lie casualty down. legs above head Loosen tight clothing (neck/ chest/ waist) Check airway, breathing, pulse and responsiveness Reassure Do not give anything by mouth until recovered Sit casualty up slowly |
|
|
What should be done if a casualty of fainting does not quickly regain consciousness (within 2 minutes)? |
Maintain airway and breathing Consider recovery position Summon aid Consider other causes of unconsciousness |
|
|
What is unconsciousness and how does it differ from sleeping? |
When a person is unable to respond to people/ stimuli - what people refer to as a coma/ comatose state Sleeping individuals can be disturbed by loud noises/ sleeping |
|
|
What should be done with an unconscious patient? |
BLS procedure Put casualty in recovery positions Ring for ambulance |
|
|
What are some of the common causes of unconsciousness in adults and children? |
Fainting Imbalance of heat Shock Head injury Stroke Heart attack Asphyxia Poisoning Epilepsy Diabetes |
|
|
What is a seizure? |
Results from temporary disruption to the normal conduction of impulses within the brain, can be partial or generalised Caused by: epilepsy, febrile convulsions, recreational drugs, alcohol, brain tumours, strokes, hypoxia, low blood sugar |
|
|
What are the stages of a generalised seizure? |
Tonic - every muscle becomes rigid, casualty may let our cry, fall to floor, back arch, lips go blue for 30 seconds Clonic - limbs make sudden violent jerks, eyes may roll, teeth may clench, saliva drools. May sound like snoring, incontinent Recovery - seizure stops, patient goes into deep sleep, become confused or agitated. Usually come around within a few minutes |
|
|
How are seizures managed in terms of first aid? |
Lie casualty down gently Clear safe space around casualty, remove dangerous items Loosen tight clothing, put something soft under head Take note of time Look for medic-alert ID When convulsions cease roll into recovery positions Stay with until recovered |
|
|
When would you call 999 for a seizing patient? |
If they have injured themselves badly If they have trouble breathing after the seizure stops If they are not known to have epilepsy/ is their first seizure If one immediately follows another with no recovery in between If it lasts two minutes longer than is usual If it lasts for 5 minutes/ unsure how long normally lasts If not showing sign of recovery of consciousness within 10 minutes |
|
|
What should not be done when a person has a seizure? |
Move the casualty unless in danger Forcibly restrain Put anything in mouth/ try to open it Try to wake Give anything to eat/ drink until fully alert |
|
|
How is hypoglycaemia managed from a first aid perpective? |
Help them take their own glucose gel/ equivalent, if not: 100mls non-diet sugary drink/ fruit juice Two teaspoons of sugar/ sugary sweets Then longer acting carbs e.g. biscuits, fruit, sandwich Glucogel can be applied to cheeks if unable to swallow |
|
|
What should be done if a hypoglycaemic patient does not respond within ten minutes or becomes unconscious? |
Follow DRSABC and call 999 |
|
|
What are the effects of anaphylaxis (allergic reaction) on the body? |
Blood vessels dilate Bronchioles in lungs constrict Blood capillary walls leak causing swelling, shock Heart contractions weaken Skin becomes itchy, rash can occur |
|
|
What are the signs and symptoms of anaphylaxis (allergic reaction) |
Sudden swelling of tongue, face, lips, neck, eyes Hoarse voice, lump in throat, developing into high pitched noisy breathing Wheezy breathing, tight chest Itchy skin, blotchy skin eruption Anxiety Drop in BP, increased pulse, pale skin, fainting all due to blood vessel dilation (up to 3x normal size) |
|
|
How often can the dose of adrenaline be repeated if there is no improvement in an anaphylactic patient or symptoms return? |
Every 5 minutes |
|
|
What commonly causes angina? |
Narrowing of the coronary arteries by atheroma (fatty patches/ plaques that develop inside the lining of the arteries) |
|
|
What commonly causes Myocardial Infarctions? |
Blood clot (thrombus) that forms inside one of the coronary arteries or one of its branches due to a ruptured plaque and blocks the blood to an area of the heart |
|
|
How are Angina and MI similar? |
Both: Site: Central chest pain Character: crushing/ heavy/ vice like/ dull/ can be mistaken for indigestion Radiation: can radiate to neck, jaw, left arm or abdomen etc. Associated symptoms: sweaty, pale, clammy, nauseated, SOB |
|
|
How are Angina and MI differentiated? |
Onset: A is predictable (e.g. during exercise), MI not Associated symptoms: MI has a sense of impending doom Timing: MI usually longer than 30 minutes, angina less |
|
|
What is basic initial treatment for angina/ MI? |
Sit down, make comfortable Half sitting position best, discourage walking Allow to take GTN spray if applicable Reassure, remove sources of stress |
|
|
When should a patient with suspected MI be allowed to chew on an aspirin tablet (300mg) and why would this be done? |
If they are not allergic and are over 16 years old May limit ischaemia |
|
|
When should the emergency services be called in a patient with symptoms of angina/ MI? |
If MI is suspected If casualty has not been diagnosed with angina before Symptoms are worse/ different to normal attacks Angina pain is not relieved by usual medication and rest after 15 minutes Angina pain has come on while at rest/ has woken them from sleep If you are in any doubt |
|
|
What are the common reversible causes of cardio-respiratory arrest in adults and children? |
Hypoxia Hypovolaemia Hyper/ hypokalaemia (electrolyte disturbance) Hypothermia Tension pneumothorax Toxic/ therapeutic disturbance Tamponade (cardiac) Thromboembolism |