Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
66 Cards in this Set
- Front
- Back
|
What are the three primary cells that make up the Islet’s of Langerhans and what hormones/proteins do they secrete?
|
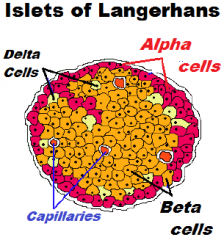
1. Alpha Cells - Glucagon (15-20% of cells)
2. Beta Cells - Insulin/Amylin (60-80% of cells) 3. Delta cells - Somatostatin (3-10% of cells) |
|
|
In addition to the rise in blood glucose, what other four events stimulate the release of insulin?
|
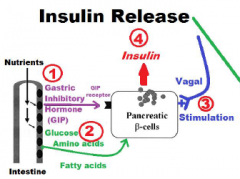
1. Amino Acid
2. Fatty Acid 3. Gastrointestinal Hormones 4. Parasympathetic of Vagal Action |
|
|
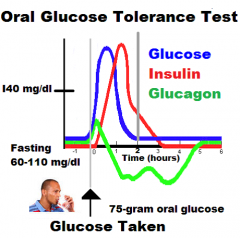
Describe the normal response of blood levels of glucose, insulin, and glucagon to an oral glucose tolerance test (OGTT).
|
|
|
|
Explain the 1st step that occur in the beta cell release of insulin.
|
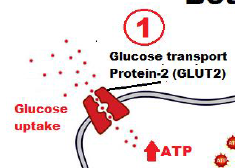
Glucose transported into beta cell by facilitated diffusion through a glucose transport protein-2 (GLUT2);
|
|
|
Explain the 2nd step that occur in the beta cell release of insulin.
|
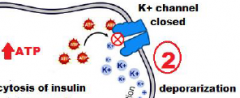
Entrance of glucose activates production of ATP, which closes potassium channels (K+ channels), thus depolarizing the cell
|
|
|
Explain the 3rd step that occur in the beta cell release of insulin.
|
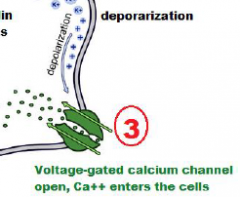
Deporization of cell opens voltage-gated calcium channels, and Ca++ enters the cell;
|
|
|
Explain the 4th step that occur in the beta cell release of insulin.
|

Entrance of Ca++ triggers exocytosis of insulin-containing secretory granules.
|
|
|
Besides glucose, what other nutrients will stimulate insulin release by beta cells?
|
1. Fats (fatty acids);
2. Proteins (amino acids) |
|
|
What are the three target cells (i.e., tissues) of insulin and what are the actions of insulin at each tissue?
|
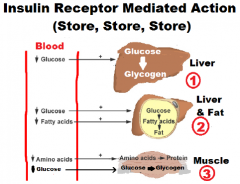
1. Liver; Glucose->Glycogen
2. Liver/Fat cells ; Glucose->Fatty Acids->Fat 3. Muscle; AminoAcids->Protein Glucose->Glycogen |
|
|
Why is Insulin called an “anabolic hormone”?
|
Anabolic Hormone in general:
stimulate growth, mineralization of bone, growth of muscle mass Insulin causes synthesis/formation of: -glycogen (from glucose) -triglycerides (from glucose) -protein (from amino acids) |
|
|
What are the cellular action of insulin at the target cell?
|
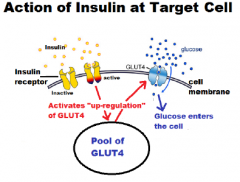
Insulin @ Receptor -> up regulate Glucose Transport Protein-4 (GLUT4)
Up regulation GLUT4 -> Entrance of glucose |
|
|
In the “Fed State”, what factors inhibit the release of glucagon from the alpha cells?
|
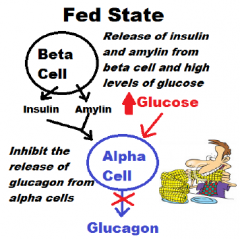
1. Insulin / Amylin (beta cells) secretion
2. Entrance of glucose into the alpha cells |
|
|
In the “Fasting State”, what two factors allow for the release of glucagon from the alpha cell?
|
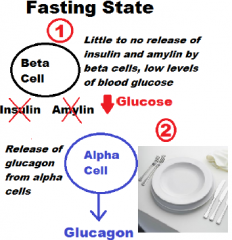
1. little to no release of insulin and amylin by the beta cells
2. Removal of the inhibitory effect that glucose entry into the alpha cells has |
|
|
What effect does Glucagon have on the liver’s glycogen (what is the term for this)?
|
Glycogenolysis:
Liver converts Glycogen -> Glucose |
|
|
What effect does Glucagon have on the liver in terms of its handling of Amino Acids (what is the term for this)?
|
Gluconeogenesis:
Liver converts Amino Acids -> Glucose |
|
|
What effect does Glucagon have on fat cells (what is the term for this)?
|
Lipolysis:
Fat cells: Triglycerides -> Fatty acids Ketogenesis: Liver: Fatty acids -> Ketones |
|
|
What effect does Glucagon have on blood levels of Ketones?
|
Liver releases ketones into the blood and therefore, increase blood levels of ketones
|
|
|
What effect does Glucagon have on blood sugar?
|
Increases blood glucose
|
|
|
What are the three types of diabetes studied in this course?
|
1. Type 1 DM
2. Type 2 DM 3. Gestational Diabetes (Type 3) |
|
|
Which one is identified with autoimmune destruction of the beta cells?
|
Type 1 DM
|
|
|
Which type of diabetes goes with Insulin insensitivity?
|
Type 2 DM
also: Gestational Diabetes (called Type 3) during pregnancy |
|
|
Which type of diabetes goes with Pregnancy?
|
Gestational Diabetes (considered type 2 b/c assoc. with insulin resistance during pregnancy)
|
|
|
What are the terms “childhood diabetes” misnomers?
|
Type 1 DM occurs in middle age or elderly
|
|
|
What are the terms “adult onset diabetes" misnomers?
|
Type 2 DM can occur in adolescents
(obesity) |
|
|
What are the terms “insulin independent diabetes” misnomers?
|
Insulin:
-treatment in the latter states of Type 2 DM |
|
|
What is the usual age range for the onset of type 1 diabetes?
|
Childhood / Adolescence
peak onset: early adolescents |
|
|
When considering the time line of type 1 diabetes, what is meant by “silent Beta cell loss”?
|
No symptoms until Symptomatic onset
|
|
|
In type 1 diabetes, by the time symptoms are demonstrated, what percentage of functional islet cell loss has occurred?
|
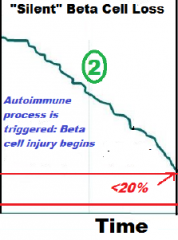
<20%
|
|
|
In type 1 diabetes, what two conditions cause diuresis?
|
High blood glucose
Ketone levels **These spill over into the urine, taking water and solutes along with them in the a process known as osmotic diuresis |
|
|
What do the terms polyuria mean?
|
Excessive Urination
(caused by Osmotic diuresis) |
|
|
What do the terms polydipsia mean?
|
Excessive Thirst
(Polyuria causes dehydration) |
|
|
In type 1 diabetes, what four symptoms are caused by Ketoacidosis?
|
1. Abdominal pains
2. Vomiting 3. Mental Confusion 4. Hyperventilation |
|
|
What are the three characteristics of type 2 diabetes?
|
1. Insulin Resistance
2. Relative Insulin deficiency 3. Hyperglycemia |
|
|
What does insulin resistance mean?
|
Higher than normal levels of insulin are needed to control blood glucose levels
|
|
|
What does relative insulin deficiency mean?
|
The beta cells become "exhausted" and cant produce sufficient amts of insulin to control blood sugar levels
|
|
|
What causes hyperglycemia?
|
-insulin resistance
-insulin deficiency (from chronic high blood glucose levels) |
|
|
What are the two metabolic defects that characterize type 2 diabetes?
|
Genetic Component
1. Derangement of beta-cell secretion of insulin (relative insulin deficiency) Environmental Component 2. Inability of peripheral tissues to respond to insulin (insulin resistance) |
|
|
What would be normal prediabetic and diabetic readings for a FASTING plasma glucose test?
|
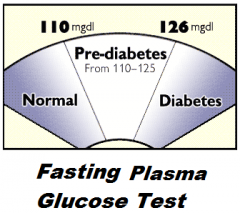
Pre-Diabetic = 110-126
Diabetic = >126 |
|
|
What would be normal prediabetic and diabetic readings for an OGTT (oral glucose tolerance test)?
|
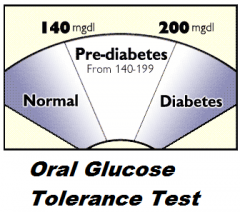
Pre-Diabetic = 140-200
Diabetic = >200 |
|
|
It is said that fasting plasma glucose test and the oral glucose tolerance test gives you a “snap shot” of a persons blood glucose whereas a glycated hemoglobin (glycosylated) hemoglobin (HbA1c) gives a clinician a “bigger pictures” of a patient’s blood glucose levels. Explain.
|
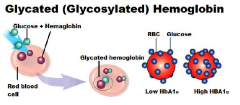
Average plasma glucose level (60-90 days)
|
|
|
What percent levels of HbA1c could be considered:
-Healthy -“at risk” developing type 2 diabetes -diagnosis for diabetes? |
≤ 5.6%: Good / healthy range
5.7 – 6.5%: At risk >6.5%: Diabetes diagnoses |
|
|
Identify the name given to areas of the body for major diabetic complications:
eyes |
Retinopathy
|
|
|
Identify the name given to areas of the body for major diabetic complications:
brain and cerebral circulation |
Cerebrovascular Disease
|
|
|
Identify the name given to areas of the body for major diabetic complications:
kidney |
Nephropathy
|
|
|
Identify the name given to areas of the body for major diabetic complications:
heart and coronary circulation |
Coronary Heart Disease (CHD)
|
|
|
Identify the name given to areas of the body for major diabetic complications:
lower limbs |
Peripheral Vascular Disease (PVD)
|
|
|
Identify the name given to areas of the body for major diabetic complications:
peripheral nervous system |
Neuropathy
|
|
|
Identify the name given to areas of the body for major diabetic complications:
diabetic foot |
Ulceration and amputation
|
|
|
How can the complications from eyes, brain, heart, kidney, lower limbs, peripheral nervous system, and diabetic foot be controlled or prevented?
|
Control Hyperglycemia
(medications / lifestyle) |
|
|
In general, what is a diabetogenic hormones?
|
Hormones that block/suppress the action of insulin
(therefore cannot stimulate uptake of glucose) |
|
|
Where are the diabetogenic hormones produced during pregnancy?
|
placenta
|
|
|
In gestational diabetes, what trimester do symptoms begin to appear?
|
3rd trimester
(Glucose levels are Elevated and diabetic symptoms begin to appear) |
|
|
factors that increase risk of Gestational Diabetes?
|
-family hist of diabetes
-obesity -abnormal birth (large baby, stillbirth, prev. birth defects) -age >25 |
|
|
Differentiate the foods with a high glycemic index (GI) in terms of speed at which glucose is released into the blood and insulin demand
|
Processed Foods / simple carbs:
-break down quickly during digestion -Release glucose rapidly into the bloodstream -spike in Insulin follows |
|
|
What types (low or high glycemic index) should a type 2 diabetic consume to help control his/her blood sugar level?
|
-Low GI (glycemic index) = lower insulin demand
-Improved long-term blood glucose |
|
|
Differentiate foods with a low glycemic index (GI) in terms of speed at which glucose is released into the blood and insulin demand
|
Complex carbs, protein, etc:
-break down more slowly -releasing glucose gradually into the bloodstream -no rapid spike in Insulin |
|
|
Glucose Levels for: Diabetic
HbA1C, Fasting Plasma Glucose, OGTT |
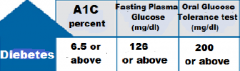
HbA1C: >6.5%
Fasting: >126 OGTT: >200 |
|
|
Glucose Levels for: Prediabetic
HbA1C, Fasting Plasma Glucose, OGTT |

HbA1C: 5.7-6.4%
Fasting: 100-125 OGTT: 140-199 |
|
|
Glucose Levels for: Normal
HbA1C, Fasting Plasma Glucose, OGTT |
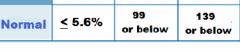
HbA1C: <5.6%
Fasting: <99 OGTT: <139 |
|
|
What is the glycemic index (GI) measuring?
|
the effects of carbohydrates on blood sugar levels
|
|
|
What are the 2 reference foods for glycemic values?
What are their GIs? |
white bread: 100
glucose: 140 |
|
|
Examples of Low GI foods
|
fruit/veggies, legumes/pulses, whole GRAINs, meat, eggs, milk, nuts, fructose, low carb foods
|
|
|
Examples of Medium GI foods
|
whole wheat products, basmati rice, sweet potato, sucrose
|
|
|
Examples of HIGH GI foods
|
baked potate, watermelon, white bread, most white rices, corn flakes, extruded breakfast cereal, glucose
|
|
|
what does gestational diabetes put the mother at risk for?
|
Later in life: Type2 DM
(especially if overweight before pregnancy) |
|
|
what does gestational diabetes put the baby at risk for?
|
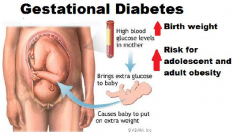
high birth weight
childhood and adulthood obesity |