Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
60 Cards in this Set
- Front
- Back

calcific aortic stenosis, most common of all valvular abnormalities, leads to LVH=>angina, ischemia, CHF, syncope, if occurs 5th-6hth decade=bicuspid valve
|
-
|
|

mitral annular calcification, degenerative calcific deposities on fibrous ring at base of valve, women >60, usually does not affect fxn but site for thrombus/ embolus
|
-
|
|

MV prolapse, caused by myxomatous degeneration. Usually no serious complications, leads to mid systolic click. Can progress to mitral regurg
|
-
|
|
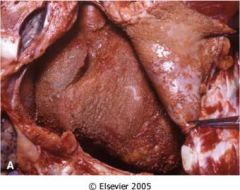
"bread and butter" pericarditis typical of the pancarditis associated with acute rheumatic fever. Can lead to a friction rub
|
-
|
|
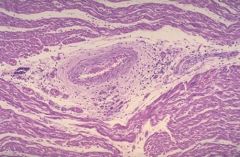
Aschoff body. Characteristic lesion of the myocarditis assoicated with acute rheumatic fever.
|
-
|
|
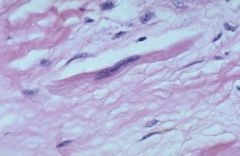
Anitschkow cell, macrophages with long, flattened nuclei. Loacted in Aschoff body, the characteristic lesion of acute rhumatic fever
|
-
|
|
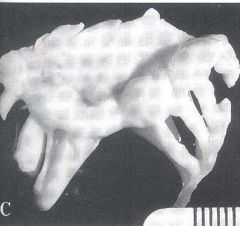
Thickening of the chordae tendineae, characteristic of chronic rheumatic heart disease
|
-
|
|

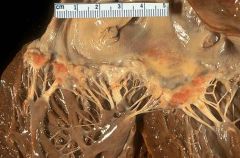
Vegetations associated with non-infective thrombotic endocarditis. The lesions are sterile and non-inflammatory and are located along the lines of closure
|
-
|
|
Endocarditis associated with Libman-Sacks non-infective endocarditis. The lesions can be located on both sides of the valve and may have intense inflammation. LSE is assoicated with SLE and primary antiphospholipid syndrome
|
-
|
|
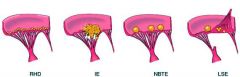
Patterns of vegetations with the vaious endocarditises, note the location of the lesion and the degree of destruction
|
-
|
|

Endocardial plaque like fibrosis assoicated with carcinoid heart diseease. SMC's and colagen are embeded in a MPS matrix. Caused by a carcinoid tumor with hepatic mets or direct secretion into systemic circulation producing various mediators. Results in TV insufficiency or PV stenosis
|
-
|
|
|
major causes of aquired aortic valve disease
|
senile calcific stenosis, insufficiency-dilation of thoracic aorta related to HTN, aging
|
|
|
major cuases of aquired mitral valve disease
|
rheumatic HD=stenosis, insufficeincy=myxomatous degneration (prolapse)
|
|
|
which is more common stenosis or insufficiency
|
stenosis
|
|
|
describe calcific aortic stenosis
|
dystrophic calcification of the aortic valve, occurs in 5th/6th decade w. bicuspid valve, 8th/9th if normale, Clinical effects-LVH, angina, ischemia, CHF, syncope, microangiopathic hemolytic anemia
|
|
|
Aortic stenosis auscutation finding
|
systolic ejection click with crescendo-decresendo murmur, S4
|
|
|
treatment of calcific aortic stenosis
|
valve replacement
|
|
|
the most common of all valvular anbormalities
|
calcific aortic stenosis
|
|
|
morphology of calcific aoric stenosis
|
calcified masses in cusps primarily ab the base, free cuspal edge is not involved and there is no fusion of the commusiures (distinuish from rheumatic HD)
|
|
|
mitral annular calcification
|
degenreative calcific deposite at base of MV ring, women >60, increased in pts with myxomatous valves or elevated Lvpressure, usually does not effect valve fxn but te for thrmobi
|
|
|
Pathogenesis of myxomatous mitral valve (prolapse)
|
very common esp young women, developmental anoamly of CT leads to deposition of mucoid material in valve
|
|
|
Clinical findings of MVP
|
usually asymptomatic, can have regurg. Complications include:infective endocarditis, mitral insufficiency, thrombi, arrythmia (with advacned insufficiency)
|
|
|
auscultaiton of MVP
|
mid systolic click, late systolic/ holosysolic murmur if regurgitation
|
|
|
pathogenesis of rheumatic heart disease
|
hypersensitivity rxn induced by group A beta hemolytic strep, antibodies against viral M protein cross react with glycoprotein antigen in heart
|
|
|
Most significant complication of Rheumatic HD
|
mitral stenosis
|
|
|
Morphology of acute Rheumatic HD
|
pancarditis: 1. bread and butter pericarditis 2. Myocarditis with Achoff bodies 3. Endocartitis affecting left sided valves with fibrinoid necrosis
|
|
|
the Achoff body is the classic leasion of
|
rheumatic HD
|
|
|
Describe Aschoff bodies
|
classic lesion of rheumatic HD. Found in the myocardium, contain collagen, swollen degenerated inflammation (lymphs, macs, plasma cells), contain Anitschkow cells (macs in aschoff bodies," Caterpillar cells")
|
|
|
describe the effect of rheumatic HD on the endocardium
|
fibrinoid necrosis and verrucae (lines of closure of valve cusps_
|
|
|
describe the effect of rheumatic HD on the myocardium
|
inflammation characterizied by Aschoff bodies with Anitschkow cells
|
|
|
describe the complications of CRHD
|
thickned valve leaflets, fusion of commissures (fishmouth/ button hole), fusion/ thickening of chordae tendineae
|
|
|
The major effect of CRHD is ___ which can lead to…
|
mitral stenosis= LA dilation=reduced CO, Pulmonary congestion, RVH, right sided heart failure
|
|
|
valves affected by CRHD
|
mitral alone>mitral _aortic> tricuspid> pulmonary
|
|
|
fishmouth or button hole deformitie of the mital valve are characteristic of
|
chornic rheumatic HD
|
|
|
fusion/ thickening of the chordae tendinae anthickend valve leaflest are characteristic of
|
CRHD
|
|
|
Diagnosis of rheumatic heart diase
|
1. Precedding group A strep infection 2. 2 major or 1 major and 2 minor manifestation
|
|
|
Major manifestations of RHD
|
JONES: Joints-migratory polyarthritis, O-Carditis, N-subcutaneous nodules, E-erethema marginatum S-Syndeham chorea
|
|
|
minor manifestations of RHD
|
fever, arthralgia, elevated acute phase reactants (ESR)
|
|
|
clinical course of RHD
|
acute: 1-4 wks after group A strep infection, kids 5-15, Chronic: years or decades after intial episode, valvular disease,
|
|
|
two forms of infectious endocarditis, cause, result
|
1. Acute-highly virulent organism infects normal vavle, necrotizing ulcerative invasive lesion requires surgery 2. Subacute-low virulent organism infects deformed valve, less destructive lesion, responds to antibiotics
|
|
|
predispositions for infective endocarditis
|
CV abnormality (RHD, myxomatous mitral valve, calcific valvular stenosis, artifical vavle), host factors (neutropneia, immunodeficiency, malignancy, diabetes, alcoholic, IV drug user
|
|
|
causes an endocarditis of deformed valves 50-60%, low virulence
|
Strep viridans (low VIRulence)
|
|
|
Causes an infective endocarditis in 10-20% of cases, most common cause in IVDA's
|
staph aureus (drugs give you an aura of hapiness)
|
|
|
Causes infective endocarditis in prosthetic valves
|
staph epidermidis (prothetics are Epi the body)
|
|
|
frequency of valves infected with endocarditis
|
most common=mitral, aortic, most common in IVDA's=tricuspid
|
|
|
criteria used to Dx bacterial endocarditis
|
Duke criteria. Major (positive blood culture, Echo, New valvular regur) Minor: predisposing heart lesion or IVDA, fever, uncommon findings from septic emboli (splinter hemorrhage, Janeway lesion, Osler node, Roth spots)
|
|
|
splinter hemorrahges in the finger nails are a sign of
|
septic emboli from bacterial endocarditis
|
|
|
Complications of bacterial endocarditis
|
valvular insufficiency, myocardial abcess, vegetations=>emboli, glomerulonephritis (immune complexes)
|
|
|
Tx of bacterial endocarditis
|
IV antibiotics (low virulence), valve replacement (high virulence), note use of prophylactic antiobiotics after valve damage
|
|
|
pathogenesis and eitology of nonbacterial thrombotic endocarditis
|
depositis of small masses of fibrin/platelets/ blood products on leaflest, often in debilitated pts, hypercoagulable state, mucin producing adenocarcinoma, endocardial trauma
|
|
|
Debiliated pts or those in a hypercoagulable state, with a mucin producing adenocarcinoma or endocardial trauma are at risk for what type of endocarditis
|
nonbacterial thrombotic
|
|
|
describe the morphology of non-infective thrombotic endocarditis
|
sterile, non-destructive, non inflmmatory vegetations along the lines of valve closure
|
|
|
Describe libman-Sacks endocarditis
|
vegetations th virbnous material and intense inflammation on either or both sides of the associated with SLE, primary antiphospholipid syndrome
|
|
|
Pts with SLE or primary antiphospholipid syndrome are at risk for what type of endocarditis
|
Libman-Sacks, nondestructive/ inflammatory, either or both sides
|
|
|
Describe the pattern of vegetations expected with RHD, IE, NBTE, and LSE
|
RHD-left sided valves, along the lines of closure; IE-friable, large, bulky, destructive, NBTE-small patches on leaflets, LSE-on both sides of valve
|
|
|
what is carcinoid syndrome
|
tumor that produces serotonin, kallikrein, bradykinin, histamine, prostaglandins, tachkinins, leads to flushing, cramps nausea, vomiting, diarhhea, leads to plauqe like fibrosis of right heart endocardium and valves (inactivation by lung MAO protects left heart)
|
|
|
which pts are are at risk for carcinoid syndrome
|
GI carcinoids with hepatic mets, carconids outside of the portal system of venous drainage leading to direct secretion into the systemic circulation
|
|
|
cardiac manifestations of carcinoid syndrome
|
plaque like fibrosis of right heart endocardium and valves (MAO in lungs protects left heart)
|
|
|
mitral stenosis ausculation
|
opening snap, diastolic rumble
|
|
|
aortic regurg auscultation
|
early blowing systolic murmur
|