Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
34 Cards in this Set
- Front
- Back

Left: Concentric hypertrophy due to pressure overload (HTN, aortic stenosis), parallel sarcomeres
Right: Eccentric hypertrophy due to volume overload (MV or AV regurg, series sarcomeres |
-
|
|
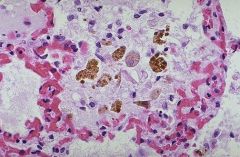
heart failure cells due to pulmonary edema, alveolar macrophages consume extravasated RBCs=>hemosiderein laden marcophages, consequence of LHF with pulmonary congesition and edema
|
-
|
|
|
heart disease US morlatlity
|
40% of US deaths, 50% greater mortality than all forms of cancer combined
|
|
|
weight and ventricular thickness of normal heart
|
weight=250-350 grams, RV=.3-.5 cm, LV=1.3-1.5 cm
|
|
|
Describe the distribution of blood supply to the heart
|
1. LAD=apex, ant 2/3 of septum, anterior wall of LV 2. LCA-laterall wall of LV 3. RCA=posterior 1/3 of septum, posterior basal wall of LV, RV free wall, flow occurs during diastole
|
|
|
which region/ layer of the heart is most vulnerable to ischemia
|
subendocardium
|
|
|
define CHF
|
inability of the heart to pump blood at a rate to meet the needs of active tissues or can only do so form an elevated filling pressure, leading discharge Dx in pts over 65, 1 millino admissinon/yr, 50,000 death, 1 yr mortality =45%
|
|
|
three general mechanisms of CHF
|
1. abnormal load presented to heart 2. impaired ventricular filling 3. obstruction due to valve stenosis
|
|
|
Causes of systolic dysfunction leading to heart failure
|
IHD, pressure or volume overload, dilated cardiomyopathy
|
|
|
causes of diastolic dysfxn leadint to HF
|
Massive LVH, amyloidosis, fibrosis, constrictive pericarditis
|
|
|
Describe the rapidly occuring compensation for HF
|
1. Frank-Starling-increase preload dilation 2. Activation of neurohormonal systems (NE/epi, Renin/Ang/ alodosteronse)
|
|
|
Hypertrophy is a compensation to HF. Expalin the two patterns of hypertrophy and what causes them
|
1. Concentric hypertrophy-caused by pressure overload, sacomeres are parallel (HTN, aortic stenosis) 2. Eccentric hypertrophy- cause by volume overload (mitral or aortic regurg), sarcomeres in series
|
|
|
how does sustained cardiac hypertrophy lead to cardiac failure
|
increased myocyte size=decreased capillary density, increased oxygen demand, altered gene expression, myocyte apotosis
|
|
|
5 causes of LHF
|
IHD, HTN, Aortic/Mitral valve diseae, Cardiomyopathies, Myocarditis
|
|
|
What are the clinical effects of LHF on the heart
|
LVH and dilation=mitral insufficiency, secondary enlargement of LA= afib, murual thrombis, S3, S4
|
|
|
what are the clinical effects of LHF on the lung
|
edema, congestion, heart failure cells, dysnpnea, PND, orthopena, crackles
|
|
|
what are heart failure cells
|
LHF leads to pulmonary congestion and extravasation of RBCs. Alveolar macs eat the RBCs and retain the iron=hemosiderin laden macrophages
|
|
|
What are the clinical effects of LHF on the kidney
|
decreased perfusion=renin/AngII/aldosteron activation=increased volume and TPR, moderate azotemia if perfusion deficit is severe
|
|
|
what are the clinical effects of LHF on the brain
|
erebral hypoxia, encephalopathy
|
|
|
the effects of RHF are mainly due to
|
engorgement of systemic and portal venous systems
|
|
|
the effects of LHF are primarly due to
|
progressive damming of blood within the pulmonary ciruclation and diminished peripheral blood pressure and flow
|
|
|
primary cause of RHF
|
secondary to LHF (others include pulmonary HTN, primary myocaridal disease, tricuspid/ pulmonary valve disoders
|
|
|
clinical effects of RHF on the heart
|
RV hypertrophy and dilation, fxnl TV regurg, S3, S4
|
|
|
clinical effects of RHF on the lungs
|
pleural effusion, atelectasis
|
|
|
clinical effects of RHF on the kidney
|
venous congestion, flud retention, severe azotemia
|
|
|
clinical effects of RHF on the liver
|
elevated portal pressue= congestion=nutmeg liver, HSM, cardiac cirrosis, ascites,
|
|
|
clinical effects of RHF on the brain
|
venous congestion, hypoxic encephalopathy
|
|
|
clinical effects of RHF on the peripheral body
|
peripheral (ankle, sacral) edema progressing to generalized massive anasarca, JVD, congestion of mucus membranes, liver congestion
|
|
|
nutmeg liver is a characteristic sign of
|
RHF, liver congestion due to increased portal pressure
|
|
|
compare the azotemia caused by LHF and RHF
|
RHF is worse- severe venous congestion of kidneys=cannot remove metabolites, LHF=less severe, poor perfusion=lack of nutrients
|
|
|
___hypertensive heart diseases Causes LHF and ___ causes RHF
|
systemic HTN=LHF, pulmonary HTN=RHF
|
|
|
heart morphology associated with systemic HTN
|
concentric LVH (pressure overload, parallel sarcomeres), no dilation (until failure),
|
|
|
define cor pulmonale
|
RVH and/or dilation and failure secondary to pulmonary HTN (accute=PE, dilation w/o hypertrophy; chronic=primary or secondary HTN due to chronic lung disease)
|
|
|
how does chronic lung disease lead to pulmonary hypertenisive lung disease (cor pulmonale) and reventually RVH/RHF
|
lung disease= hypoxia= vasonconstriction=increased afterload=RVH=RHF
|