Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
32 Cards in this Set
- Front
- Back
|
World Federation Neurosurgeons (WFNS) SAH grading
|
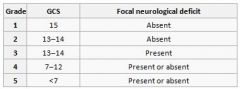
Score correlates with mortality
|
|
|
Child-Pugh Classification
|
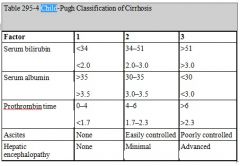
Operative mortality:
Score: 5-6 = Class A = low risk < 5% 7-9 = Class B = moderate risk 25% 10-15 = Class C = high risk > 50% |
|
|
Apgar Score
|

- Apgar’s are taken at 1 and 5min
- Memory aid: Activity (muscle tone) Pulse Grimace (reflex irritability) Appearance (colour) Respiration |
|
|
CHADS2
|
CHADS2=0, no therapy or Aspirin only is recommended
CHADS2=1, either Aspirin or Warfarin is recommended (depending on patient preferences) CHADS2 ≥ 2 should be managed with lifelong Warfarin (target INR 2.0-3.0) Overall risk of stroke in non-valvular AF is around 5% per year Warfarin reduces risk of CVA from 5% to 1% per annum Risk of major bleed 0.5% per annum |
|
|
Aortic Stenosis Severity (Echo)
|
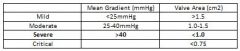
AHA Guidelines
|
|
|
Mitral Stenosis Severity (Echo)
|
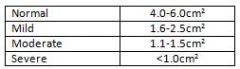
AHA Guidelines
|
|
|
Pulmonary Hypertension Severity (Echo)
|
Based on mean PAP:
Mild: 25-35 Moderate: 35-45 Severe: >45mmhg Based on RVSP: >40 has likely PHTN 50-60 moderate >60mmhg as severe |
|
|
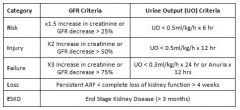
RIFLE Criteria
|
|
|
|
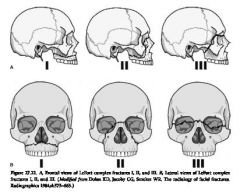
LeFort Fractures
|
|
|
|
Obstructive Lung Disease Severity
|
Severity based on FEV1% of predicted values (GOLD report on COPD 2011)
ᵒ Mild (stage 1) : >80% predicted ᵒ Moderate (stage 2): 50-80% predicted ᵒ Severe (stage 3): 30-50% predicted ᵒ Very Severe (stage 4) : <30% predicted |
|
|
STOP BANG
|
Snoring: loud snoring (can be heard through closed doors)
Tiredness: daytime somnolence Observed apnoea Plood pressure: Hx of hypertension BMI: >35 Age: >50 Neck Circumference: >40cm Gender: male >3 = High risk of OSA → refer for sleep testing |
|
|
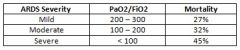
ARDS Severity
|
|
|
|
Soda Lime - Contents and reaction
|
Contains:
94% calcium hydroxide 5% sodium hydroxide 1% potassium hydroxide An indicator – such as ethyl violet Silica – increases hardness of the granules, minimising formation of alkaline dust which can be an airway irritant if inhaled The active ingredient is the sodium hydroxide, which acts as a catalyst, and is not actually consumed in the reaction: CO2 + H20 ↔ H2CO3 2NaOH + H2CO3 → Na2CO3 + 2H2O + heat Na2CO3 + Ca(OH)2 → CaCO3 + 2NaOH + heat |
|
|
Diastolic Heart Failure Echo Assessment
|
Transmitral flow velocity
E wave: peak filling velocity in early diastole A wave: peak filling velocity in late diastole E/A relationship Normal: E/A is > 1 As atrial kick only contributes 30% of filling Mild DD aka ‘Impaired relaxation’ E/A is <1 Relaxation is impaired and atrial contraction contributes relatively more to ventricular filling Moderate DD aka ‘Pseudonomral filling’ E/A normalises to E>A Compliance and relaxation reduced → impaired early diastolic filling and raised LAP → E >A Differentiated from normal by assessing transmitral flow with valsalva Severe DD aka ‘Restrictive filling’ E >> A LV compliance is extremely low → high LAP → high velocity E wave |
|
|
PONV
Apfel Simplified Risk Score Eberhart Simplified Risk Score |
Apfel Simplified Risk Score – In Adults
Four risk factors Female sex Non-smoker Hx of PONV or motion sickness Use of postoperative opioids Risk Score: 0 RF (baselines risk) = 10%, 1 RF = 20%, 2 RF = 40%, 3RF = 60%, 4 RF = 80% Eberhart Simplified Risk Score – In Children Four risk factors Age > 3 Surgery >30 mins Hx of POV, or PONV in 1st degree relative Strabismus surgery Risk Score: 0 RF (baselines risk) = 10%, 1 RF = 10%, 2 RF = 30%, 3RF = 55%, 4 RF = 70% |
|
|
MELD Score
|
Model for End-Stage Liver Disease (MELD) Score
Uses bilirubin, creatinine and INR MELD = 3.78[Ln serum bilirubin (mg/dL)] + 11.2[Ln INR] + 9.57[Ln serum creatinine (mg/dL)] + 6.43 Score correlates to 3month mortality |
|
|
ECG Lead sensitivity
|
V5 = 75%
V4 + V5 = 90% II + V4 + V5 = 98% |
|
|
Classification of breathing Circuits
|
A
ᵒ A spring loaded pop off valve located near the face ᵒ Gas flow enters at other end near reservoir bag B & C ᵒ Pop off valve at face with FGF also near patient. ᵒ Reservoir bag and tubing are a blind limb where FGF, dead space and alveolar gas collect D,E,F ᵒ FGF near patient, excess gas popped off at other end Efficiency Spontaneous ventilation: A>DFE>CB Controlled ventilation: DFE> BC >A DEF are commonly used, ABC very uncommonly used |
|
|
Mapleson A
|
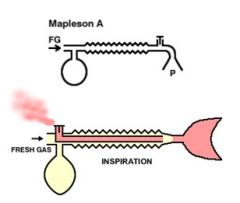
Efficiency
SV: FGF = MV CV: FGF = 3xMV |
|
|
Mapleson B & C
|
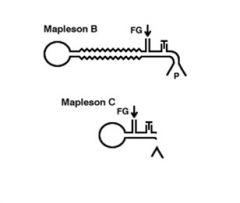
Efficiency
SV: FGF = 2xMV CV: FGF 50% > than MV required B more efficient with CV as has reservoir tube |
|
|
Mapleson D
|
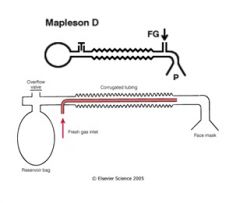
D most efficient for CV
Bain's = modified D - SV: 2-3xMV - CV: 1-2xMV |
|
|
Mapleson E & F
|
Mapleson E (Ayre's T-piece)
- FGF of 3xMV required in SV Mapleson F (Jackson Reese Modification) - FGF 2-3xMV required The volume of the reservoir tubing should be at least 1/3rd of the patient’s tidal volume. If the volume is too large, rebreathing may occur, and if too small, ambient air may be entrained |
|
|
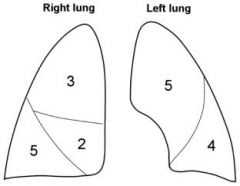
Lung Segments
|
|
|
|
Thoracics Cardiopulmonary Testing
|
CPEX
VO2max >20 mL/kg/min (or >15ml/kg/min & FEV1 >40% predicted) = low risk of respiratory complications VO2max <15 mL/kg/min = high risk of morbidity and mortality VO2max <10 mL/kg/min = 40-50% mortality, consider non-surgical management Stair Climb One “flight” = 20 steps at 6 inches/step Climbing five flights = VO2max >20 mL/kg/min Climbing two flights = VO2max of 12 mL/kg/min Patient unable to climb two flights is at extremely high risk 6MWT Distance correlates well with VO2max Distance <600m correlates to a VO2max <15 mL/kg/min and also correlates with a fall in oximetry (Spo2) during exercise Drops in SpO2 > 4% during exercise are associated with increased morbidity |
|
|
Define:
- Quality Assurance - Alternative Medicine - Attributes of the anaesthetist - Impairment - Autonomy - Beneficence - Non-malificence - Paternalism - Justice |
QA: “an organised process that assesses and evaluates health services to improve practice or quality of care”
Steps = planning, implementation, review, setting standards Alternative Medicine "Any substance which may be used by an individual for its effects on health or disease process, that is not recognised by the regulatory authorities of that country for these properties" Attributes of the anaesthetist - Communicator, Collaborator, Medical Expert, Manager, Professional, Health Advocate, Scholar Teacher Impairment when a colleague’s behaviour consistently departs from the expected behaviour set out in these codes of conduct, and impacts on his or her performance Autonomy: recognises the rights of individuals to make decisions regarding their own health – self-determination Beneficence: A practitioner should act in the best interest of the patient Non-Maleficence: A practitioner has a duty not to harm patients Paternalism: A practitioners decision to act for a patients good without regard for the patients conception of what would be good in the given situation Justice: The greatest good for the greatest number of people |
|
|
Classification of Head Injury
|
Mild = GCS 13-15
Need to monitor / CT Watch for BOS fracture, intoxication, vomiting, etc Moderate = GCS 9-12 High risk of morbidity Intubate and ventilate if not cooperative for CT Monitor 24 hrs Severe = GCS <9 Resuscitate Evaluation / Diagnosis Surgical Mx Monitoring ICU |
|
|
Current Thresholds
MACROSHOCK Sensation Pain Muscular contraction Respiratory insufficiency VF and burning MICROSHOCK |
MACROSHOCK
Sensation is about 1 mA Pain at 10mAmp Muscular contraction at 16 mA (i.e. ‘let go’ threshold) Respiratory insufficiency at 50 mA VF and burning at > 100 mA MICROSHOCK 0.05- 0.1mA (i.e. 1/1000 macroshock level & 1/100 sensation level) Electrocution causing VF can occur below the level of perception |
|
|
Circuit breaker current flow trigger
RCD trigger LIM limits |
Circuit breaker current flow trigger = >10mA for 1/10sec
RCD trigger: 5-10mA difference, triggers in 40milisec LIM limits: Prospective Hazard Current (P.H.C.) of 5mA |
|
|
ANATOMY
Subcostal Ilioinguinal/iliohypogastric Genitofemoral Pudendal Femoral Lateral femoral cutaneous Sciatic Obturator Pudendal branches Cardiac veins Spinal Cords Blood Supply |
Subcostal = lateral cutaneous branch of T12
Ilioinguinal/Iliohypogasric = Lateral cutaneous branches of L1 - Above ASIS - travel between TA & IO - Below ASIS - ilioinguinal between TA & IO, iliohypogastric between IO & EO Genitofemoral = L1, L2 Pudendal = anterior divisions S2-4 Femoral = L2-4 Lateral femoral cutaneous = L2,3 Sciatic = L4-5, S1-3 Obturator = L2-4 Pudendal Branches: inferior rectal nerve, dorsal nerves of the penis, perineal branch Cardiac veins - Great cardiac vein (anterior IV groove, runs with LAD) - Middle cardiac vein (inferior interventricular groove (with PDA) - Small cardiac vein (base of heart, with marginal branch of RCA) Spinal Cord Blood supply - Anterior spinal artery (from vertebral artery at level of forament magnum) - Radicular branches (lower cervical, lower thoracic, upper lumbar, adamkiewicz) - Posterior spinal artery x 2 (from posterior inferior cerebellar artery) - Venous drainage: radicular veins empty into epidural venous plexus |
|
|
Myasthenia Gravis - Predictors of need for Post-Op Ventilation
|
Predictors for need of post-op ventilation:
ᵒ Major body cavity surgery ᵒ Disease duration of longer than 6 years ᵒ Presence of chronic respiratory disease unrelated to MG ᵒ Daily dose of pyridostigmine >750 mg + significant bulbar dysfunction ᵒ Vital capacity < 2.9 L |
|
|
Dental Blocks
Anterior Superior Alveolar Middle Superior Alveolar Posterior Superior Alveolar Inferior Alveolar Nasopalatine Greater palatine |
Anterior Superior Alveolar
- Above lateral incisior/canine in mucobuccal fold Middle Superior Alveolar - Above 2nd maxillary premolar in mucobuccal fold, aim toward infraorbital foramen Posterior Superior Alveolar - Above 2nd MOLAR in mucobuccal fold. Needle at 45 degrees, aim superiorly, medially, laterally Inferior Alveolar - Maximally open the mouth, injection point is the mucosa immediately between the upper and lower molars Nasopalatine - V2 branch, supplied maxillary anterior palate from canine to canine - Inject into incisive foramen Greaterpalatine - V2 branch, supplied Palatal soft tissue from maxillary canine back - Insertion is ~1cm medial from 1st/2nd maxillary molar on the hard palate |
|
|
LARYNX ANATOMY
EXTRINSIC MUSCLES INTRINSIC MUSCLES Abductors of the cords Adductors of the cords Sphincters to vestibule Regulators of cord tension |
Sternothyroid
Thyrohyoid Inferior constrictor of the pharynx Abductors of the cords: posterior cricoarytenoids Adductors of the cords: lateral cricoarytenoids, interarytenoid Sphincters to vestibule: aryepiglottics, thyroepiglottics Regulators of cord tension: cricothyroids (tensors), thyroarytenoids (relaxors), vocales (fine adjustment) |