Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
290 Cards in this Set
- Front
- Back

|
Trypanosoma gambiense.
(African trypanosomiasis) |
|
|
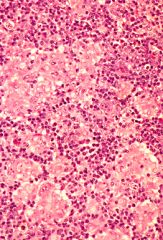
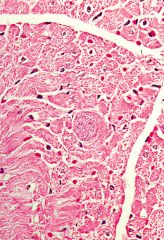
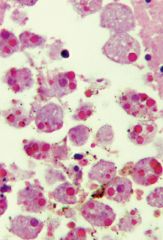
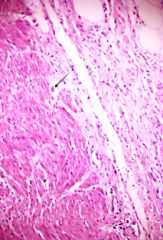
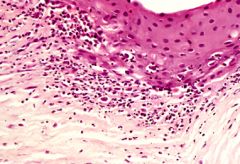
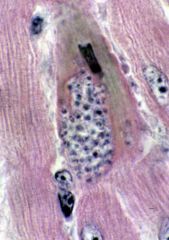
Trypanosoma cruzi.
The muscle fibers filled with Leishmania forms of the organism can be identified. |
|
|
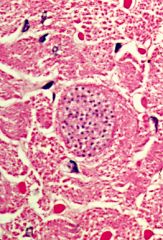
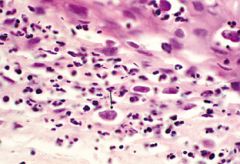
Trypanosoma cruzi.
The muscle fibers filled with Leishmania forms of the organism can be identified. This is more clearly seen in the high power where the nucleus and kinetoplast in each of the Leishmania forms can be easily seen. These organisms must be distinguished from Toxoplasmosis in which multiple single nuclei are present within the parasitised muscle fibers. |
|

|
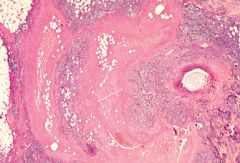
Cutaneous Leishmaniasis.
The lesion has heaped-up edges and an ulcerated center. |
|
|
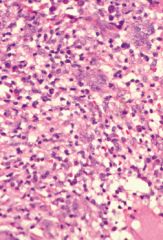
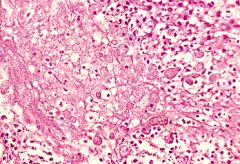
Cutaneous Leishmaniasis.
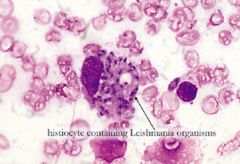
The inflammatory infiltrate can be seen to consist of lymphocytes, plasma cells, eosinophils, and foamy histiocytes which have organisms in the cytoplasm. |
|
|
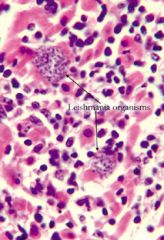
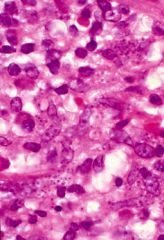
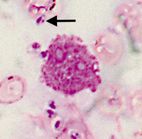
Cutaneous Leishmaniasis.
Under oil immersion, the parasites have the morphological features of Leishmania. They are round with an eccentric nucleus, and in some of them a smaller micro-nucleus or kinetoplast can be seen. |
|

|
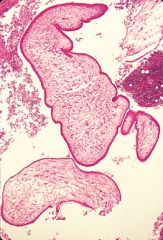
The leptomonad form of Leishmania.
The nucleus, kinetoplast and flagellum are clearly visible. This is the appearance of Leishmania organisms in the sandfly vector. |
|
|
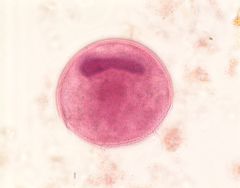
Leishmania parasites that have a nucleus and a small kinetoplast.
|
|
|
How is leishamaniasis differentiated from histoplasmosis?
|
The distinction is made by identifying the presence of a kinetoplast in association with the nucleus, as seen in Leishmaniasis. In addition, the Histoplasma capsulatum yeast is PAS positive, whereas the Leishmania organisms are PAS negative.
|
|
|
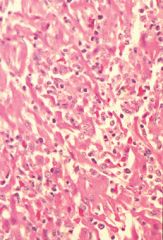
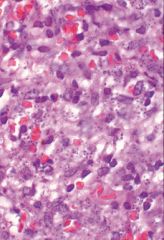
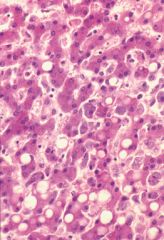
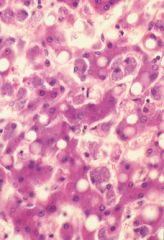
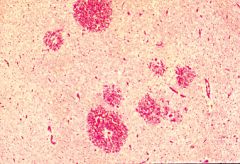
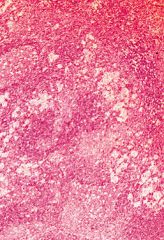
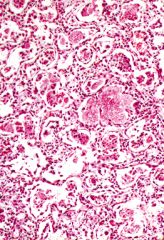
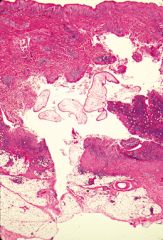
Visceral lesihmaniasis.
The hepatocytes are morphologically normal, but the sinusoids are markedly distended by proliferating Kupffer cells which are filled with Leishmania organisms. |
|
|
Visceral leishmaniasis.
The hepatocytes are morphologically normal, but the sinusoids are markedly distended by proliferating Kupffer cells which are filled with Leishmania organisms. |
|
|
Visceral leishmaniasis.
|
|
|
Visceral leishmaniasis.
|
|
|
Visceral leishmaniasis.
|
|
|
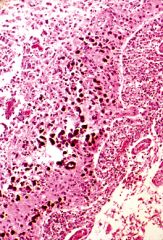
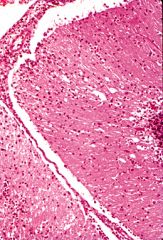
Cerebral malaria.
Cerebral malaria presents with a variety of neurological manifestations. It may present as acute psychosis, fitting or abnormal behaviour. These can progress quite quickly to coma and death.Very often the post mortem examination of the brain shows no macroscopic abnormality. The classical abnormality however, is the presence of multiple petechial hemorrhages throughout the white matter. |
|
|
Cerebral malaria.
Areas of hemorrhage (low power). |
|
|
Cerebral malaria.
Thrombosis of a vessel, destruction of the vessel wall and haemorrhage into the brain substance. Many of the red blood cells contain ring forms of P. falciparum. |
|
|
Cerebral malaria.
Shows a cerebral capillary in which the red blood cells contain malaria pigment and ring forms of P. falciparum. This appearance can be seen in the capillaries throughout the brain. This is the usual finding in patients dying of cerebral malaria when no macroscopic abnormality can be seen in the slices of post mortem brain. |
|
|
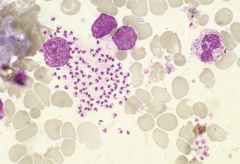
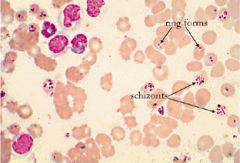
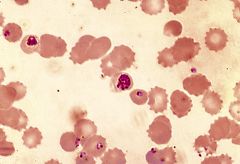
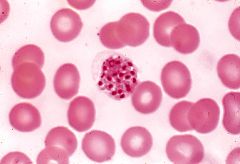
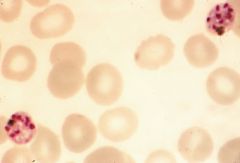
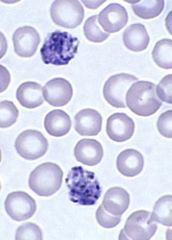
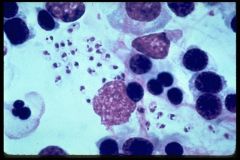
Malaria.
Ring forms and schizonts can be seen. Schizonts are not seen in peripheral blood smears in malaria except as a pre-terminal event. If schizonts are seen in peripheral smears the patient will die quite quickly unless treatment is started as a matter of urgency. |
|
|
How does the size of the various types of malaria in infected red blood cells compare to the size of uninfected red blood cells?
|
P. falciparum - the parasitized red blood cells are the same size and shape as the non-parasitized cells.
P. vivax - the parasitized red blood cells are larger than the non-parasitized ones. P. malariae - the parasitized red blood cells are not enlarged and are the same size as the non-parasitized ones. P. ovale - the parasitized red blood cells are enlarged and most of them are oval in shape. |
|
|
What are the parasite size and shape of the various types of malaria?
|
P. falciparum - the trophozoites are all small rings with a red staining nuclear dot and a small amount of blue-staining cytoplasm.
P. vivax - the trophozoite may be in a ring form with a nuclear dot and a crescent of cytoplasm or it may be much larger and have an irregular contour (an amoeboid form) P. malariae - the trophozoite has a large round nucleus and a solid blue cytoplasm. Very frequently this cytoplasm adopts a shape which looks like a thick band across the red blood cell. P.malariae often has a well defined blob of brown malarial pigment in the red blood cell. P. ovale - the trophozoite is large with a big nucleus and abundant, irregularly distributed cytoplasm. |
|
|
How do the schizonts of the various types of malaria compare?
|
P. falciparum - schizonts are present in the peripheral blood only in the pre-terminal phase of the infection. The schizonts contain 12 - 24 merozoites (nuclear dots). The red blood cell containing the schizont is not enlarged.
P. vivax - contains 12 - 24 merozoites and the infected red blood cell is enlarged. P. malariae - the schizont contains 8 - 12 merozoites. The infected red cell is not enlarged. P. ovale - the schizont contains 12 - 24 merozoites. The infected red blood cell is enlarged and is an oval shape. |
|
|
How do the gametocytes of the various types of malaria compare?
|
P. falciparum - the gametocytes are crescent shaped.
Gametocytes of the other three species are round with a large eccentric nucleus at the edge. Gametocytes are about the same size as the schizont for the particular species. |
|
|
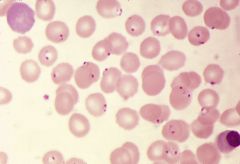
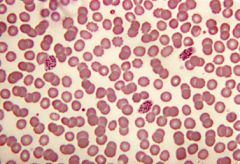
A thick blood film from a fairly heavy infection of P. falciparum. Numerous ring forms (trophozoites) can be seen.
|
|

|
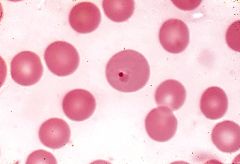
A very occasional ring form of P. falciparum in a thick film.
|
|
|
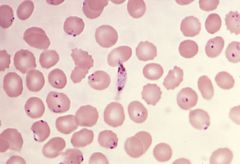
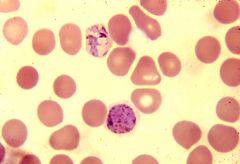
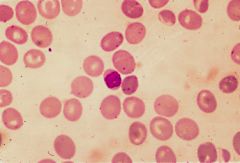
Thin film from a patient with a heavy infection of P. falciparum.
Malaria causes a hemolytic anemia. This blood film shows the presence of haemolysis with a polychromatic red cell in the top left hand corner and a nucleated red cell in the bottom right hand corner. This is P. falciparum because the red cells are all about the same size and shape, and the parasites are all small rings. |
|
|
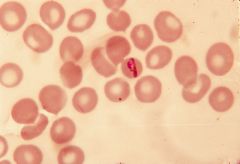
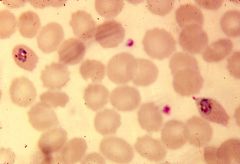
Presence of a characteristic crescent-shaped gametocyte of P. falciparum. It usually takes about eight days from the beginning of the first fever until gametocytes appear in the peripheral blood, so this patient would have had his fever for at least one week.
|
|
|
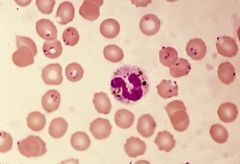
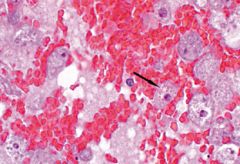
P. falciparum.
It shows a neutrophil with malarial pigment in the cytoplasm. |
|
|
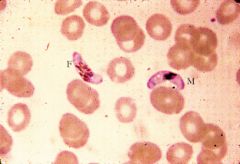
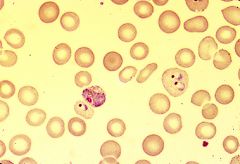
P. falciparum.
There is a female gametocyte of P. falciparum on the left and a male on the right. The nuclear material in the female is more diffuse than in the male. |
|
|
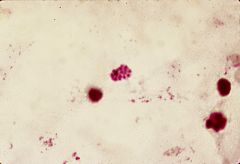
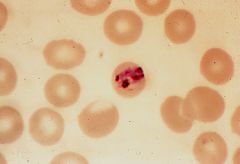
P. falciparum.
It shows a schizont which contains about sixteen or eighteen merozoites, together with some pigment. This patient would have died within a few hours if treatment had not been started at once. |
|
|
Thick blood film of P. vivax. There is a schizont in the middle of the field.
|
|
|
Thin blood smear that shows trophozoites and a gametocyte of P. vivax. The parasitized red blood cells are larger than their neighbours, and the trophozoites are large ring forms. The gametocyte is round and has a single red nuclear dot.
|
|
|
Thin blood film showing P. vivax. The trophozoite is an amoeboid form. The lower parasite is a gametocyte. Both parasites are in red blood cells that are enlarged.
|
|
|
Schizont of P. vivax. The red blood cell is enlarged and there are eighteen merozoites in the schizont.
|
|
|
Ring form of P. vivax. This appearance presents one of the diagnostic problems in the species identification of malaria. The trophozoite is only marginally larger than the trophozoite of P. falciparum but it is P. vivax because the infected red blood cell is enlarged. In such cases one usually finds more characteristic trophozoites of P. vivax in other parts of the smear.
|
|
|
Peripheral blood smear that shows P. malariae. The infected red blood cell is not enlarged. The trophozoite is large and is forming a band across the middle of the red cell.
|
|
|
P. malariae infection. The red cell is not enlarged. The trophozoite is in a band form and there is a large blob of pigment associated with the parasite. This prominent malarial pigment is a feature of P. malariae.
|
|
|
Two schizonts of P. malariae. The red cells are not enlarged. The schizont has ten merozoites and each schizont has a large blob of pigment within it.
|
|
|
Gametocyte of P. malariae. The red blood cell is not enlarged, the gametocyte is round and there is a single nucleus at one margin.
|
|
|
Blood smear that shows three schizonts of P. ovale. The red blood cells are enlarged and an oval shape. Each schizont contains approximately twelve to sixteen merozoites.
|
|
|
P. ovale parasites. The red blood cells are enlarged and their shape is changed. One is a definite oval shape and the other is flattened on one edge. The trophozoites are large and amoeboid in form.
|
|
|
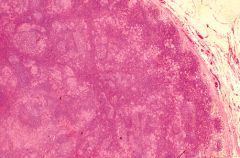
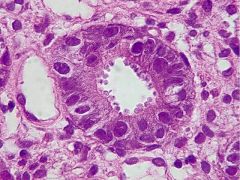
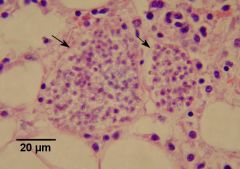
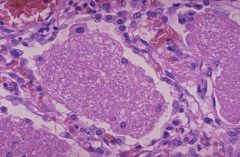
Histological appearances of toxoplasmosis in a lymph node. The normal lymph node architecture is retained. There is some follicular hyperplasia. Scattered throughout the node there are well circumscribed and tightly packed foci of pale staining histiocytes.
|
|
|
Histological appearances of toxoplasmosis in a lymph node. The normal lymph node architecture is retained. There is some follicular hyperplasia. Scattered throughout the node there are well circumscribed and tightly packed foci of pale staining histiocytes.
|
|
|
Histological appearances of toxoplasmosis in a lymph node. The normal lymph node architecture is retained. There is some follicular hyperplasia. Scattered throughout the node there are well circumscribed and tightly packed foci of pale staining histiocytes.
|
|
|
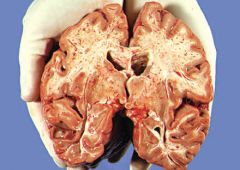
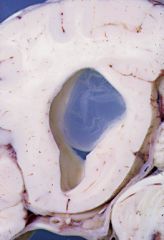
Toxoplasmosis.
Anterior half of the brain sliced through the mamillary bodies. There is marked dilatation of the frontal and temporal horns of the lateral ventricles with very marked thinning of the cerebral cortex. |
|

|
Toxoplasmosis.
Posterior half of the brain showing hydrocephalus of the occipital horns of the lateral ventricles with marked thinning of the overlying cerebral cortex. As the brain was being cut there was a slightly gritty sensation which corresponded to calcification in the thinned cortex. Calcification lining the dilated ventricles can be seen in x-rays of children with Neonatal Toxoplasma Encephalitis. |
|
|
Toxoplasmosis.
Cerebral cortex at a higher power. This shows the presence of calcification and a moderately heavy chronic inflammatory cell infiltration in the subarachnoid space. |
|
|
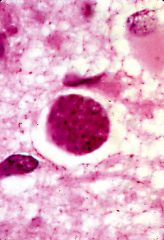
Cyst of Toxoplasma that was found in an area of cortex in which there was only a minimal degree of inflammation.
|
|
|
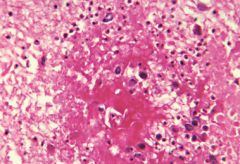
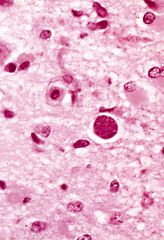
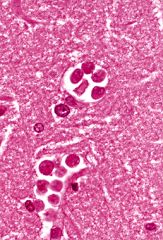
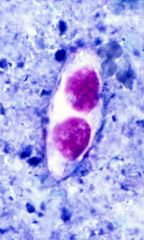
Toxoplasma cyst.
Frequently such cysts are found in areas of inflammation and active encephalitis. The main differential diagnosis of a Toxoplasma cyst is from (i) an aggregate of Leishmania organisms. This can be done by noting the absence of kinetoplast in the Toxoplasma cyst. (ii) Histoplasma capsulatum. These yeasts are a similar size to the individual Toxoplasma organisms but they stain positively with PAS. |
|
|
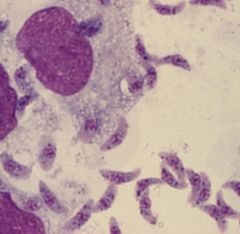
High power view of individual crescentic Toxoplasma organisms grown in culture in peritoneal fluid of a laboratory mouse.
|
|
|
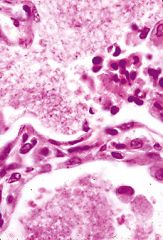
The heart of a middle aged male who died from AIDS. The Toxoplasma cyst is expanding the myocardial muscle fiber. In this case there is no inflammatory reaction associated with the cyst. The presence of an inflammatory reaction is variable.
|
|
|
The heart of a middle aged male who died from AIDS. The Toxoplasma cyst is expanding the myocardial muscle fiber. In this case there is no inflammatory reaction associated with the cyst. The presence of an inflammatory reaction is variable.
|
|
|
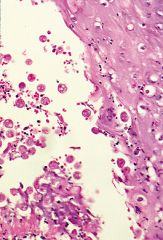
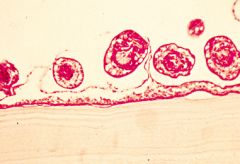
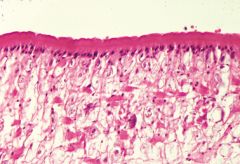
Pneumocystis infection causes focal or diffuse collections of "fluffy" pink staining material in the alveolar spaces. At a low power this pink material looks somewhat like pulmonary edema except that the latter is more homogeneous.
|
|
|
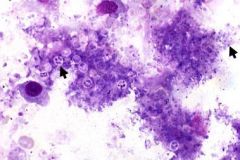
Pneumocystis carinii.
High power shows that the exudate is rather honeycombed, and even in the Haematoxylin and Eosin stained sections, the blue nuclear dots of the trophozoites of Pneumocystis can be seen. The spaces around the dots are the cysts. The cysts can be more easily seen in silver stains, for example, Grocott. |
|
|
Pneumocystis carinii.
Low power view of a Grocott stain of lung. The individual cysts stain black. |
|
|
Pneumocystis carinii.
Grocott stain of lung. The individual cysts stain black. |
|
|
The Pneumocystis infection does not excite a very florid inflammatory cell reaction in the lung. The predominant cell in such inflammatory reactions is the plasma cell. The first descriptions of Pneumocystis pneumonia referred to the condition as "plasma cell" pneumonia.
Interstitial plasma cell infiltration in the lung. The pulmonary macrophage shows a cytomegalovirus within the nucleus. This opportunistic virus is frequently seen in association with a Pneumocystis infection. |
|
|
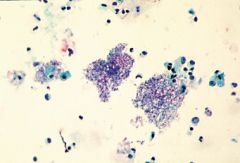
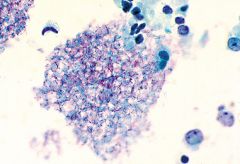
Pneumocystis carinii.
Bronchial lavage preparation stained with Giemsa stain. This outlines the cyst walls and demonstrates the trophozoites within the cyst. Each cyst usually contains four or eight trophozoites. Silver stain or Gram stain are equally useful in staining smear preparations. |
|
|
Pneumocystis carinii.
Bronchial lavage preparation stained with Giemsa stain. This outlines the cyst walls and demonstrates the trophozoites within the cyst. Each cyst usually contains four or eight trophozoites. Silver stain or Gram stain are equally useful in staining smear preparations. |
|
|
Pneumocystis carinii.
Bronchial lavage preparation stained with Giemsa stain. This outlines the cyst walls and demonstrates the trophozoites within the cyst. Each cyst usually contains four or eight trophozoites. Silver stain or Gram stain are equally useful in staining smear preparations. |
|
|
E. histolytica.
|
|
|
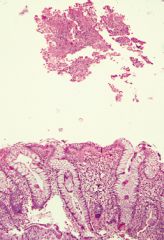
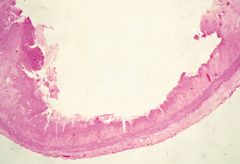
Amebic diarrhea.
Histological examination shows rectal mucosa and purulent exudate on its mucosal surface. |
|
|
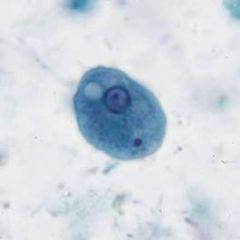
The rectal mucosa itself does not show significant inflammation but the trophozoites of E. histolytica can be easily seen in the purulent exudate under medium power magnification
|
|
|
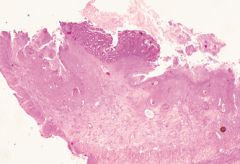
Microscopic section taken across one of the ulcers in E. histolytica. It emphasises the deep erosion into the muscle layer of the bowel and the undermining of the mucosal epithelium at the edge of the ulcer.
|
|
|
Exudate in E. histolytica.
|
|
|
Amoebae can be found within the exudate of E. histolytica.
|
|
|
E. histolytica in exudate.
|
|
|
E. histolytica in exudate.
|
|
|
E. histolytica in exudate.
|
|
|
E. histolytica invading blood vessels.
|
|

|
Amebic liver abscess.
|
|

|
Brown colored pus from amebic abscess.
|
|
|
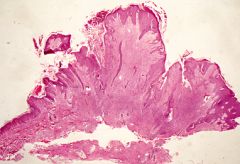
Cutaneous amebiasis.
Shows normal skin at the edge of an area of very marked epithelial proliferation and thickening. |
|
|
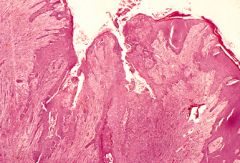
Ulcer in cutaneous amebiasis in which pus contains E. histolytica.
|
|
|
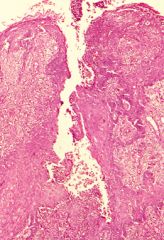
Ulcer in cutaneous amebiasis in which pus contains E. histolytica.
|
|
|
|
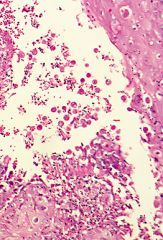
Ulcer in cutaneous amebiasis in which pus contains E. histolytica.
|
|
|
Ulcer in cutaneous amebiasis in which pus contains E. histolytica.
|
|
|
Ulcer in cutaneous amebiasis in which pus contains E. histolytica.
|
|

|
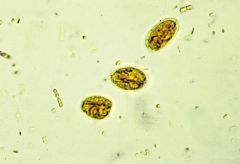
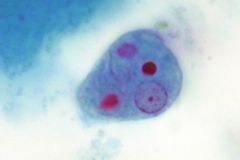
The Entamoeba histolytica cyst is fairly small, up to 25 microns in diameter. It contains four nuclei, each with a well-defined central karyosome.
|
|
|
Naegleria fowleri. Microscopically the meninges are filled with mononuclear inflammatory cells and the amoebae can be seen mixed with this cellular infiltrate.
|
|
|
Naegleria fowleri.
The amoebae invade the brain by way of the Virchow-Robin spaces. The amoebae are small, approximately 10 microns in diameter. They have a nucleus and very little cytoplasm. |
|
|
Within these areas of hemorrhage there are many ameba with morphological features of Acanthamoeba. These organisms are approximately 20 microns in diameter. They have a well-defined nucleus that contains a prominent nucleolus. The cytoplasm is abundant and contains numerous vacuoles.
|
|
|
Patients who use contact lenses sometimes develop corneal ulceration caused by the free-living Acanthamoeba. The amoebae live in the water in which the contact lenses are kept overnight.
|
|
|
Patients who use contact lenses sometimes develop corneal ulceration caused by the free-living Acanthamoeba. The amoebae live in the water in which the contact lenses are kept overnight.
|
|
|
Base of an ulcer in the colon, where Balantidium coli organisms can be seen. These are large organisms approximately 50 microns in diameter. They are round, have a large nucleus and vacuolated cytoplasm.
|
|
|
Base of an ulcer in the colon, where Balantidium coli organisms can be seen. These are large organisms approximately 50 microns in diameter. They are round, have a large nucleus and vacuolated cytoplasm.
|
|

|
Balantidium coli.
Oil immersion picture of formalin fixed faeces from stools from a laboratory monkey. The tiny cilia can be seen on the surface of the organism adjacent to the macronucleus. |
|
|
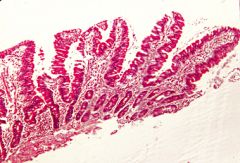
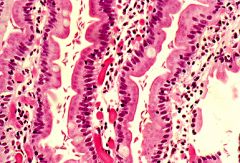
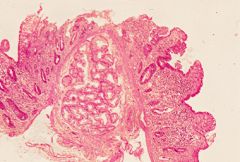
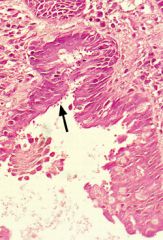
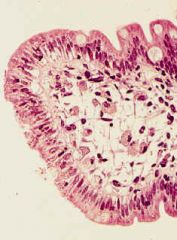
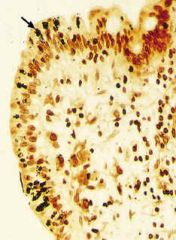
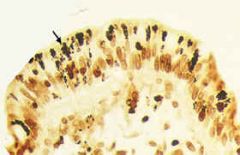
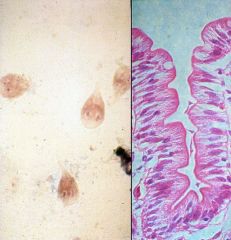
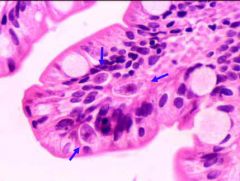
The usual appearance of a small intestinal biopsy in a patient with giardiasis. The small bowel is morphologically normal. The villi are of normal length. There is no inflammation. Large numbers of organisms can be seen in the surface mucus and in the recesses between adjacent villi.
|
|

|
The usual appearance of a small intestinal biopsy in a patient with giardiasis. The small bowel is morphologically normal. The villi are of normal length. There is no inflammation. Large numbers of organisms can be seen in the surface mucus and in the recesses between adjacent villi.
|
|
|
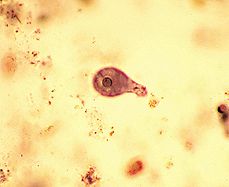
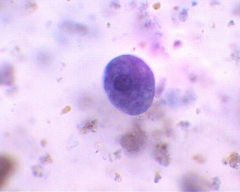
Giardia.
|
|
|
Giardia.
An oil immersion view showing the trophozoites on end and "en face". The pear-shape of the organism is best seen in the front face view and then the two nuclei are visible, resembling a pair of eyes. |
|
|
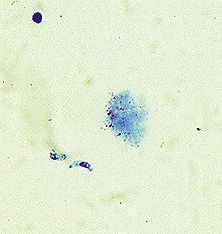
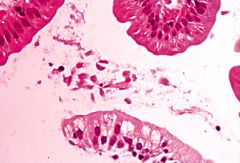
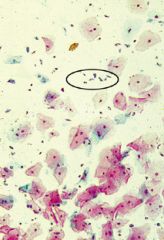
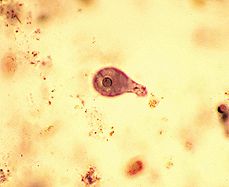
Motile trophozoite of Giardia from a wet preparation of duodenal aspirate.
|
|
|
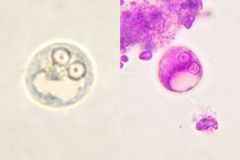
Small, oval, thick walled cysts of Giardia lamblia as seen in a sample of feces.
|
|
|
Trichomonas.
|
|
|
|
Trichomonas.
|
|
|
Trichomonas.
|
|
|
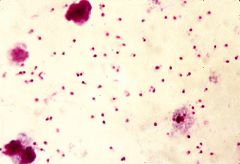
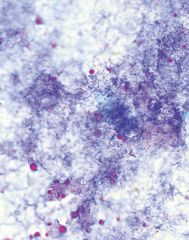
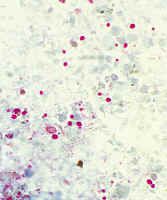
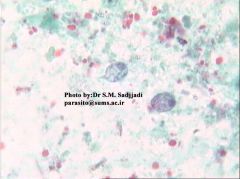
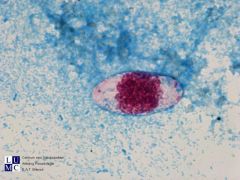
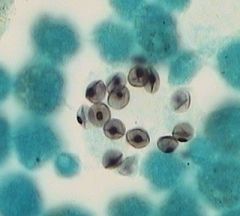
Cryptosporidiosis.
An oil immersion view of the oocysts in diarrhoeal feces. The feces sample was concentrated and stained by a modified Ziehl Neelsen stain. The organisms stain a bright pink color. |
|
|
Cryptosporidiosis.
The villi are somewhat shortened, the surface epithelium is damaged and there is a moderate increase in the number of chronic inflammatory cells in the lamina propria. The oocysts can be seen on the surface of the epithelial cells as rounded, regular, blue-stained bodies. |
|
|
Cryptosporidiosis.
|
|

|
Cryptosporidiosis.
|
|
|
Oil immersion magnification of spores of Enterocytozoon bieneusi in diarrhoeal feces of an AIDS patient who was suffering from diarrhoea. The feces sample was concentrated and stained with a modified Giemsa stain.
|
|
|
Microsporidiosis.
|
|
|
Microsporidiosis.
Warthin Starry. |
|
|
Microsporidiosis.
Warthin Starry. |
|

|
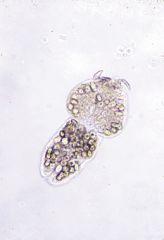
Dog tapeworm - E. granulosus. It is a small worm, about 5mm long. It has a head (scolex) with suckers and hooklets. It has one mature and one gravid segment. In the gravid segment the uterus is filled with eggs. The genital pore opens laterally in the middle of the gravid segment.
|
|

|
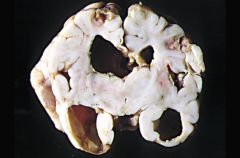
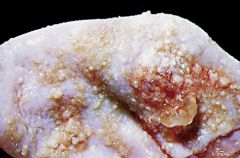
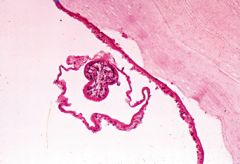
Echinococcus.
Liver is the commonest organ in which hydatid cysts develop. The cysts may produce palpable enlargement of the liver. Hydatid cyst in a liver specimen from a 53 year old sheep farmer. It was an incidental post mortem finding. The cyst is composed of a thick white outer membrane one or two millimetres thick. Adjacent to the cyst there is a chronic inflammatory cell reaction with fibrosis in the adjacent tissue. Within the cyst there are multiple daughter cysts of varying size. If the main cyst ruptures these daughter cysts spill into other tissues and continue to grow. |
|
|
Echinococcus.
Inner lining of the laminated membrane. The laminated membrane is lined by a single layer of germinal epithelium from which new daughter cysts develop. The developing daughter cysts can be seen as granular projections on the inner lining of the cyst. As these daughter cysts grow, they break off from the germinal epithelium and float freely in the cyst. |
|
|
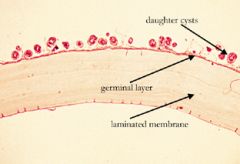
Echinococcus.
Low power view of the laminated membrane lined by the germinal layer with daughter cysts developing from it. |
|
|
Echinococcus.
Medium power view. The laminated membrane can be clearly seen. Sometimes in biopsy specimens there is no germinal layer and one cannot see developing daughter cysts. The appearance of the laminated membrane itself is usually enough to make a positive diagnosis of hydatid cyst. At this power the germinal membrane and the developing daughter cysts can be easily seen. |
|
|
Echinococcus.
Higher power view to show a developing daughter cyst. A new scolex (or head) is forming within the cyst. |
|
|
Ehinococcus.
Scolex from which hooklets are breaking off from the top. |
|

|
Echinococcus.
Scolex with intact hooklets. |
|

|
Echinococcus.
Chest x-ray from a 10 year old boy who was recovering from an attack of pneumonia. It shows a large opacity in the lower part of his right lung. |
|

|
Echinococcus.
The white laminated membrane has begun to pull away from the tissue reaction in the lung. A careful family history failed to reveal any contact with either dogs or sheep. This is not an uncommon story. It is very difficult to explain how such patients develop their infection. |
|

|
Echinococcus.
Left kidney which has been bisected longitudinally. The upper two thirds of the kidney has been compressed and replaced by a hydatid cyst. The calyceal system of the kidney is hydronephrotic, being dilated because of the compression on the collecting system by the enlarging hydatid cyst. This kidney came from a six year old male who was investigated for recurrent attacks of urinary tract infection. |
|
|
Echinococcus.
A slice of the brain at post mortem with a transparent daughter cyst floating in the greatly dilated lateral ventricle. |
|
|
Sparganosis.
Low power view of a section taken from a subcutaneous lump on the back of a 28 year old male. He said that the lump on his back was slowly moving. He lived in a country town and often spent weekends hunting wild pigs. The section shows an inflammatory abscess with a cross section of a "worm" in the center. |
|
|
Sparganosis.
Higher power of the "worm" - the sparganum. It has a well defined integument, no internal organs, and no scolices. |
|
|
Sparganosis.
The integument at higher power. The surface shows the presence of microvilli and on the inner surface of the integument there is a line of well defined tegumental cells. Within the body of the sparganum there are a number of small muscle fibres. In the centre there is a small focus of calcification (a fairly common finding in this parasite). |
|
|
Sparganosis.
Section of a subcutaneous lump removed from the left thigh of an 81 year old farmer. In the centre of an abscess within the lump there is a degenerate worm surrounded by a brisk acute on chronic inflammatory cell reaction. |
|

|
Sparganosis.
The wall of a somewhat degenerate sparganum larva. |
|

|
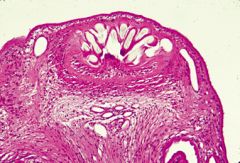
Cysticercosis.
An almost complete Taenia solium tapeworm that was passed after the patient had been given treatment to expel the worm. The head end is at the upper part of the photograph. It is thinner than the distal end, which contains the gravid proglottids, filled with eggs. The head of the worm is missing. |
|

|
Cysticercosis.
Closer view of the scolex (head) of a Taenia solium. There is a row of hooklets above the part of the scolex which bears the four suckers. The presence of a worm in the intestine usually causes no observable symptoms. Fragments of proglottid may be passed in the faeces, and the patient may notice the presence of motile fragments of flat, white, soft tissue. Otherwise, symptoms are related to the presence of cysticerci. |
|

|
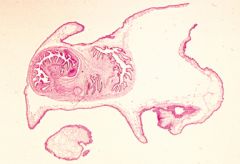
Cysticercosis.
Longitudinal section through one of the gravid proglottids. Genital pores occur laterally in the middle of the proglottids. They open on alternate sides of succeeding proglottids. |
|
|
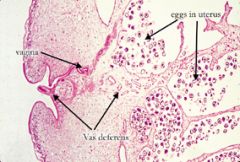
Cysticercosis.
Closer view of the genital pore. The vagina opens superiorly as a well defined tube. The vas deferens is a smaller tube and is somewhat twisted as shown by the presence of large numbers of transverse sections leading away from the genital pore. The testis consists of multiple small rounded structures in the connective tissue septum between the branches of the uterus towards the right side of the photograph. |
|
|
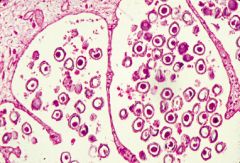
Cysticercosis.
High power view of the multi-branched uterus filled with eggs. |
|

|
Cysticercosis.
Eggs in the feces. They are a brown colour, round with a thick capsule. They measure approximately 36 microns in diameter. |
|

|
Cysticercosis.
Under diffracted light (Figure 29.8) radial striations can be seen in the capsule of the egg. Eggs from all species of tapeworm are morphologically identical. |
|
|
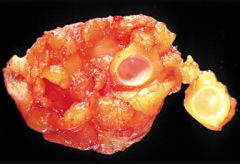
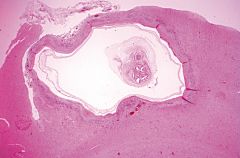
Cysticercosis.
The lump is 10mm in diameter and it was removed with some surrounding adipose tissue. The lump was a cysticercus. The piece on the right includes the cysticercus with the white nodule of the head (scolex) within it. The remainder of the cyst on the left consists only of cyst wall. |
|

|
Cysticercosis.
In the specimen on the left, the membrane of the cysticercus has been cut in two pieces. Both of them have separated easily from the surrounding tissue response of the body. In the specimen on the right the cysticercus has floated out of the cystic cavity. These macroscopic features of the surgical specimen can cause diagnostic confusion for the histopathologist. |
|

|
Cysticercosis.
Unless the scolex is included in the section the histopathologist may get a section. Here the only abnormality is an empty cyst lined by granulation tissue. |
|
|
Cysticercosis.
The correct approach would be to section not only the cyst wall, but also the cysticercus itself. Now, one sees the head of the new worm and the wall of the cysticercus. |
|

|
Scolex of a cysticercus.
|
|
|
Cysticercosis.
Scolex of a cysticercus. |
|
|
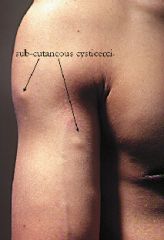
Cysticercosis.
multiple, soft, subcutaneous lumps, each approximately 10mm in diameter on the right upper arm and chest. This 29 year old agricultural student from Thailand had multiple similar lumps over all parts of his body. He had a fairly heavy infection of sub-cutaneous cysticerci. |
|

|
Cysticercosis.
A number of calcified areas in his calf muscle. These represent degenerate cysticerci that have become calcified. |
|

|
Cysticercosis.
A section through muscle in which there are multiple cysticerci present. |
|

|
Cysticercosis.
A section through muscle in which there are multiple cysticerci present. |
|

|
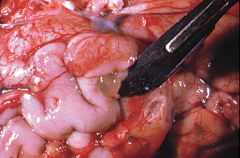
Cysticercosis.
Undersurface of the temporal lobe of the brain. There are two transparent cysticerci under the leptomeninges at the anterior end of the temporal lobe. This was an incidental post mortem finding in a 72 year old male immigrant to Australia from Pakistan. |
|
|
Cysticercosis.
Undersurface of the temporal lobe of the brain. There are two transparent cysticerci under the leptomeninges at the anterior end of the temporal lobe. This was an incidental post mortem finding in a 72 year old male immigrant to Australia from Pakistan. |
|
|
Cysticercosis.
Low power microscopic section which shows the head and thin wall of the cysticercus. The surrounding brain shows a thick membrane formed by gliosis. |
|
|
Wet mounts are good for looking for which parasites?
|
Motile trophozoites and cyst forms.
|
|
|
Detection of what is enhanced by adding a dilute iodide to a wet mount?
|
Cyst forms.
|
|
|
Modified acid-fast stains are positive with which parasites?
|
Cryptosporidium, cyclospora, and isospora.
|
|
|
Genital pore injection is used to aid in the diagnosis of what species?
|
Taenia.
|
|
|
What does genital pore injection determine?
|
Uterine branching pattern of Taenia species.
|
|
|
What are the uterine branching patterns for the various types of Taenia species?
|
T. solium = <13 lateral branches.
T. saginatum = >13 lateral branches. Dipylidium caninum = 2 genital pores. |
|
|
What are amebae (sarcodinia)?
|
Unicellular organisms that are motile by pseudopodal extension.
|
|
|
What is the primary pathogen in the amebae?
|
Entamoeba histolytica.
|
|
|
What are the features of E. histolytica?
|
The nucleus is characteristically a small, central karyosome with finely beaded heterochromatin that is applied evenly to the innter nuclear membrane. Can have ingested red cells in the cytoplasm. Display progressive unidirectional motility under direct examination in wet mounts. Cyst forms have up to 4 nuclei and chromatoidal bodies with smooth, rounded, ends.
|
|
|
What are the clinical manifestations of E. histolytica?
|
It is acquired through ingestion of cysts in contaminated food or water. It is the main cause of intestinal amebiasis, which consists of protracted diarrhea. Can lead to extraintestinal manifestations such as amebic abscess within the liver, spleen, or brain that are described as having anchovy paste-like material. The lesion if intestinal amebiasis is the "flask-shaped" ulcer in the cecum. Protracted infection can lead to a napkin-ring lesion (ameboma) that mimics adenocarcinoma.
|
|
|
Entamoeba histolytica
|
|
|
Entamoeba histolytica.
|
|
|
Entamoeba histolytica cyst.
|
|
|
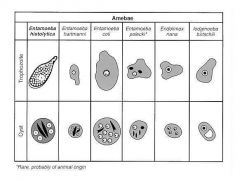
How is entamoeba coli distinguished from entamoeba histolytica?
|
Entomoeba coli has nondirectional motility, eccentric karyosome, clumped nuclear chromatin, frayed chromatoidal bodies, and has up to 8 nuclei in cyst forms. Also, E coli does not contain ingested red cells.
|
|
|
How is entamoeba hartmanii distinguished from E. histolytica?
|
E. histolytica is larger (25 μm) than E. hartmanii (5-10 μm).
|
|
|
How is entamoeba nana distinguished from E histolytica?
|
E nana has a large knobby "ball and socket" central karyosome. The cyst form has the same nuclei and lacks chromatoidal bodies.
|
|
|
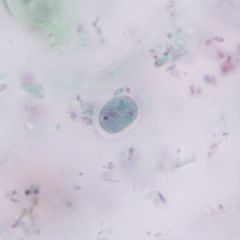
Entamoeba coli.
Has the characteristic eccentric karyosome. |
|
|
Entamoeba coli.
Eccentric karyosome. |
|
|
Amebae
|
|
|
Entamoeba nana.
Trichrome stain. |
|
|
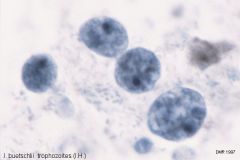
What is the appearance of Iodamoeba butschlii?
|
The cyst has a prominent iodine-staining vacuole. The trophozoite and cyst form have a large "ball and socket" central karyosome, but the nuclear membrane is inconspicious.
|
|

|
Iodamoeba butschlii.
|
|
|
Iodamoeba butschlii.
|
|
|
What is the classic history of infection with Naegleria fowleri?
|
Fatal meningoencephalitis arising in children who have been swimming in fresh-water pools. The frontal lobe is infected via the cribriform plate, and the infection is fatall within days.
|
|
|
What does Acanthamoeba cause?
|
Granulomatous amebic encephalitis (GAE) and contact lens-associated acanthamoebic keratitis.
|
|
|
Where can Naegleria fowleri and Acanthamoeba be found?
|
Soil, water, and other environmental substrates.
|
|
|
How is Naegleria fowleri cultured?
|
N. fowleri found in CSF can be cultured on a lawn of inactivated Escherichia coli. A visible trail formed when the ameba moves across the plate ingesting the E. coli is confirmatory.
|
|
|
Naegleria fowleri.
The clear spaces around the trophozoites represents shrinkage of the amebae. |
|
|
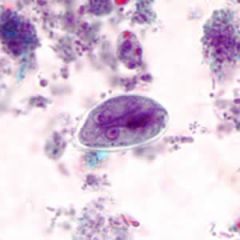
What is the microscopic appearance of Giardia lamblia?
|
They are kite-shaped when viewed from the top with a central axostyle running along their length. The flagella are not easily seen. From the side view, the organisms are comma-shaped. The cysts are oval, thick-walled, and have 4 nuclei located along a central axostyle.
|
|
|
What is the characteristic motility of Giardia lamblia on wet mount called?
|
"Falling-leaf" motility.
|
|
|
What is the most common cause of protozoal gastroenteritis?
|
Giardia.
|
|
|
Giardia lamblia cyst.
Trichrome stain. |
|
|
Giardia lamblia.
|
|
|
What is Chilomastix mesnili?
|
It is a nonpathogenic lumen-dwelling flagellate. It lasck a central axostyle, has rotary motion, and has only anteriorly located flagella. The cyst form has a single nucleus located adjacent to a safety pin-shaped structure. There is tapering of the end opposite the nucleus.
|
|
|
Chilomastix mesnili.
|
|

|
Chilomastix mesnili.
|
|
|
What is the microscopic appearance of Dientamoeba fragilis?
|
It is a round binucleate structure that has a nucleus with a fragile central karyosome. There is a single flagellum which appears attached to the wall of the organism at several points.
|
|
|
What does Dientamoeba fragilis cause?
|
It can cause diarrhea and anal pruritus, particularly in children.
|
|
|
What is the microscopic appearance of Trichomonas vaginalis?
|
It is a pear-shaped organism with 2 nuclei located at the anterior end of a central axostyle. Has an undulating membrane that extends halfway down the organism.
|
|
|
What is Trichomonas hominis?
|
It is a nonpathogenic organism that has a single nucleus located at the anterior end of a central axostyle. Has an undulating membrane that extends along the top of and all the way down the organism.
|
|

|
Trichomonas vaginalis.
|
|
|
Trichomonas vaginalis.
|
|
|
Trichomonas hominis.
|
|
|
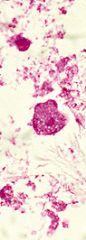
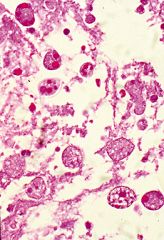
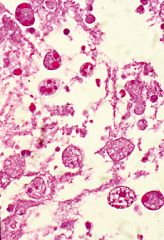
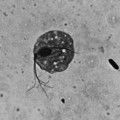
What is Trypanasoma cruzi?
|
It is the cause of Chagas disease (American trypanosomiasis). It is a cause of congestive heart failure and achalasia. It is acquired from the reduviid bug, whose inoculation site (Chagoma) when present about the eye is called the Romaña sign.
|
|
|
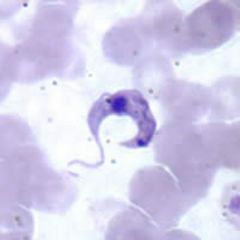
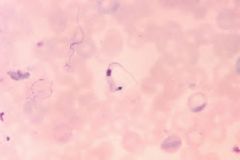
What is Trypanasoma brucei?
|
It is the cause of African sleeping sickness (African trypanosomiasis), an acute febrile illness that results in death. Acquired through the tsetse (glossina) fly. East African trypanosomiasis is caused by T. brucei rhodesiense. West African trypanosomiasis is caused by T. brucei gambiense.
|
|
|
Which has the larger kinetoplast: T cruzi or T brucei?
|
T cruzi.
|
|
|
On what medium can trypanasoma species be culture?
|
Novy-MacNeal-Nicolle medium.
|
|
|
Trypanasoma cruzi.
|
|
|
Trypanasoma cruzi.
|
|
|
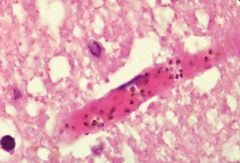
Trypanosoma cruzi.
Amistigotes in heart. |
|
|
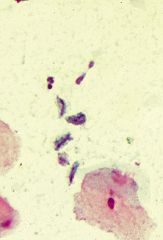
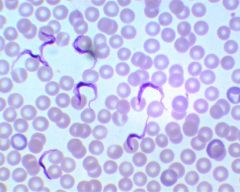
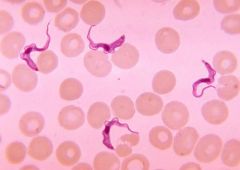
Trypanosoma brucei.
Delicately curved structures with an undulating flagellum that is attached along its length, ending in a whip-like tail. |
|
|
Trypanosoma brucei.
Delicately curved structures with an undulating flagellum that is attached along its length, ending in a whip-like tail. |
|
|
What is the only ciliate?
|
Balantidium coli.
|
|
|
What is the microscopic appearance of Balantidium coli?
|
A 50-70 μm organism with cilia uniformly covering its surface. Has a kidney bean-shaped macronucleolus. The cyst form has cilia that can be seen beneath the outer cyst wall as well as the kidney bean-shaped macronucleolus.
|
|

|
Balantidium coli trophozoite.
|
|
|
Balantidium coli cyst.
|
|
|
What does Cryptosporidium parvum cause?
|
It is a major cause of protracted diarrhea in immunocompromised patients. It can also ascend the biliary tree to cause strictures.
|
|
|
What is the microscopic appearance of Cryptosporidium parvum?
|
It is a dome-shaped 8-15 μm, basophilic structure that appears to be adherent to the small intestine brush border but is in acutality located within an apical vacuole.
|
|
|
Cryptosporidium parvum.
|
|

|
Cryptosporidium parvum.
The eggs are weakly acid-fast. |
|
|
Isospora belli.
|
|
|
Isospora belli.
|
|
|
Isospora belli.
|
|
|
What is the microscopic appearance of Isospora belli?
|
Thin elliptical structures with weakly acid-fast eggs with one (unsporulated) or two (sporulated) sporocysts.
|
|
|
What is the microscopic appearance of microsporidium?
|
Microsporidia appear in small intestinal biopsies as numerous tiny intracellular organisms within the apex of enterocytes.
|
|
|
Microsporidium.
|
|
|
What is Cyclospora?
|
It is an organism acquired from ingestion of contaminated fruit and leafy vegetables in Nepal, Peru, Haiti, and Guatemala. It is acid-fast by modified techniques.
|
|
|
What is the characteristic syndrome of Cyclospora infection?
|
Several days of fever, severe watery diarrhea, followed by an extended period of anorexia and fatigue.
|
|
|
What is the pathogenesis of Sarcocystis?
|
It is acquired from beef or pork and leads to self-limited gastroenteritis.
|
|
|
What is the microscopic appearance of Sarcocystis?
|
It appears as an hour glass-shaped eggs with two sporocysts.
|
|

|
Sarcocystis.
|
|
|
What is the definitive host for Toxoplasma gondii?
|
Cat. Infection is acquired through ingestion of material contaminated with cat feces.
|
|
|
What is the risk if maternal infection of Toxoplasma gondii occurs in the first trimester of pregnancy?
|
Risk of fetal loss.
|
|
|
What is the risk if maternal infection of Toxoplasma gondii occurs in late pregnancy?
|
Risk of fetal CNS infection that centers around the retina and ventricles, with the residual effect of periventricular calcification and chorioretinitis.
|
|
|
Are women previously infected with Toxoplasma gondii safe from intrauterine toxoplasmosis infection?
|
Yes.
|
|
|
With what symptoms does a person present with Toxoplasma gonddi infection?
|
Mononucleosis-like syndrome (fever and posterior cervical lymphadenopathy).
|
|
|
What laboratory values suggest recent Toxoplasma gondii infection?
|
IgG titers >1:1024 or still rising.
|
|
|
What establishes the diagnosis of congenital and acute infection of Toxoplasma gondii?
|
Anti-toxoplasma IgM.
|
|
|
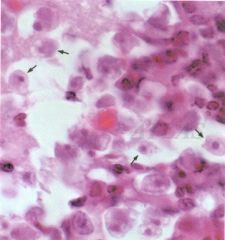
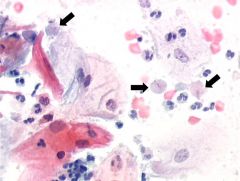
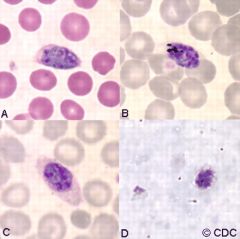
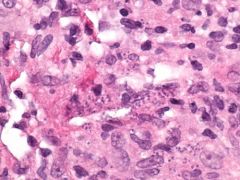
What is the microscopic appearance of Toxoplasma gondii?
|
The tachyzoite is a small curved, 3-5 μm free form of the organism. The bradyzoite is a pseudocyst form of the organism in which numerous organisms are packed into the cytoplasm of a histiocyte. Giemas is good for demonstrating the organism.
|
|
|
Toxoplasma gondii.
Tachyzoite. |
|
|
Toxoplasma gondii.
Bradyzoite. |
|
|
Fever spikes every 48 hours (tertian fever) for which species of Plasmodium?
|
P. falciparum, P. ovale, P. vivax.
|
|
|
Fever spikes every 72 hours (quartan fever) for which species of Plasmodium?
|
P. malariae.
|
|
|
Which species of Plasmodium is called malignant tertian malaria and why?
|
P. falciparum due to its lethality and every other day fever.
|
|
|
Which species of Plasmodium are called benign tertian malaria?
|
P. vivax and P. ovale.
|
|
|
Which Plasmodium is associated with nephrotic syndrome?
|
P. malariae.
|
|
|
Which Plasmodium is associated with CNS involvement?
|
P. falciparum.
|
|
|
Relapse is seen in which species of Plasmodium?
|
P. vivax and P. ovale.
|
|
|
Which species of Plasmodium infect younger erythrocytes?
|
P. vivax and P. ovale.
|
|
|
Which species of Plasmodium infects older erythrocytes?
|
P. malariae.
|
|
|
Which species of Plasmodium infects any erythrocytes?
|
P. falciparum.
|
|
|
Where do most cases of P. ovale infection occur?
|
Western Africa.
|
|
|
What blood group antigen mediates attachment of P. vivax?
|
Duffy.
|
|
|
What condition is protective against P. falciparum?
|
Hemoglobin S trait (HbSA).
|
|
|
What condition is protective against all Plasmodium species?
|
Glucose-6-phosphate dehydrogenase (G6PD).
|
|
|
What are the morphological features of P. falciparum?
|
Only early ring forms and gametocytes are seen within peripheral blood erythrocytes. Multiple rings may be seen in a single erythrocyte. Schizonts are not usually seen. Gametocytes are banana-shaped. Infected RBCs are not enlarged.
|
|
|
What are the morphological features of P. malariae?
|
Infected erythrocytes are not enlarged, no Schuffner dots, schizonts have 6-12 nuclei, coarse malarial pigment may be present.
|
|
|
What are the morphological features of P. vivax and P. ovale?
|
Infected RBCs are slightly enlarged, gametocytes are amoeboid in shape, schizonts have 12-14 nuclei, P. ovale is associated with fimbriated erythrocytes.
|
|
|
Plasmodium ovale.
|
|
|
Plasmodium vivax.
|
|
|
What is the microscopic appearance of Babesia microti?
|
The trophozoites are usually multiple, located within RBCs, and form tetrads or Maltese cross arrangements. Extraerythrocytic ring forms are present, unlike Plasmodium species.
|
|
|
How is Babesia microti acquired?
|
The tick Ixodes dammini.
|
|
|
What are the clinical features of Babesia microti infection?
|
Nonperiodic fever and hemolysis, leukopenia, abnormal liver function tests, death.
|
|
|
What are the clinical features of Pneumocystis carinii infection?
|
Presents as a bilateral (butterfly) pulmonary infiltrates in an immunocompromised patient.
|
|
|
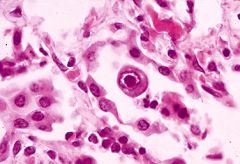
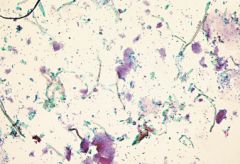
What is the microscopic appearance of Pneumocystis carinii?
|
The trophozoite appears as 5 to 8 μm concave discs when their walls are stained with GMS. There is a characteristic frothy exudate which suggests the organisms presence.
|
|
|
Pneumocystis carinii.
|
|
|
Pneumocystis carinii.
|
|
|
Pneumocystis carinii.
|
|
|
What is the pathogenesis of Echinococcus?
|
It is acquired when ingesting food contaminated with stool of an infected dog. Sheep and cattle are intermediate hosts. Results in the formation of cysts in various organs, particularly the liver.
|
|
|
How many cysts are seen in Echinococcus granulosis?
|
One or several unilocular hydatid cysts.
|
|
|
How many cysts are seen in Echinococcus multilocularis?
|
Multilocular cysts are seen.
|
|
|
Polycystic hydatid cyst disease is seen with which species of Echinococcus?
|
Echinococcus vogeli.
|
|

|
Echinococcus granulosis egg.
|
|
|
Echinococcus granulosis larvae.
|
|

|
Echinococcus granulosis.
|
|
|
What is the microscopic appearance of Dipylidium caninum?
|
It occurs in globular packets of 5-6 eggs enclosed by a thin membrane. The proglottis has a double genital pore, one exiting out of each side.
|
|
|
What is the pathogenesis of Dipylidium caninum?
|
It commonly infects cats and dogs and occasionally children.
|
|

|
Dipylidium caninum.
The proglottis has a double genital pore. |
|

|
Dipylidium caninum.
The egg consists of globular packets of 5-6 eggs enclosed by a thin membrane. |
|
|
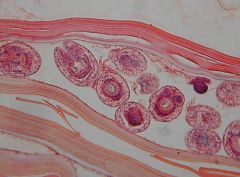
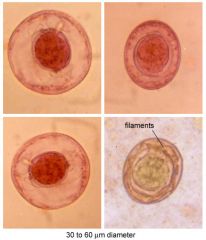
What is the microscopic appearance of Hymenolepsis nana (dwarf tapeworm)?
|
The egg consists of an inner shell and an outer shell with a wide space in between. The inner shell has two polar thickenincs, pairs of filaments that look like tiny bows.
|
|
|
What is the pathogenesis of Hymenolepsis nana infection?
|
It is a cestode that follows ingestion of contaminated water or food, the typical contaminant being rodent droppings.
|
|
|
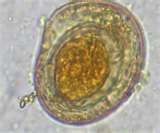
How is Hymenolepsis nana distinguished from Hymenolepsis diminuta?
|
H. diminuta does not have the pairs of filaments that look like bows.
|
|
|
Hymenolepsis nana.
|
|
|
Hymenolepsis nana.
|
|

|
Hymenolepsis diminuta.
|
|
|
What is the pathogenesis of Diphyllobothrium latum?
|
It is a fish tapeworm found in temperate zones and acquired through the ingestion of poorly-cooked freshwater fish. Infection can become complicated by vitamin B12 deficiency.
|
|
|
What is the morphology of Diphyllobothrim latum?
|
The egg is a 60-70 μm oval structure with a smooth shell and an unshouldered operculum ("hatch door) at one end and a small abopercular knob on the other end. The scolex appears as an elongated almond with longitudinal grooves. Each proglottid is characteristically wider than it is long.
|
|

|
Diphyllobothrium latum.
The uterus is rosette-shaped. |
|

|
Diphyllobothrium latum.
Almond-shaped scolex. |
|

|
Diphyllobothrium latum.
Egg. |
|
|
Diphyllobothrium latum egg.
|
|
|
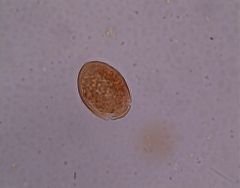
What is the pathogenesis of Taenia solium?
|
The pork worm is seen in the US most commonly with recent imitration. Infection occurs with ingestion of encysted organisms (cysticerci) in pork. Cysticersosis is a condition in which cysts containing larvae are found in the brain and elsewhere.
|
|
|
What is the microscopic appearance of Taenia solium?
|
The eggs are spherical with a thick radially striated wall and contains 3 pairs of hooks. The scolex has 4 suckers and many tiny hair-like hooks on its surface (armed rostellum). The proglottids are short and have <13 lateral uterine branches. An invaginated scolex with a double row of hooklets that are acid-fast and birefringent is key.
|
|

|
Taenia solium.
Scolex. |
|

|
Taenia solium.
Eggs. |
|
|
What is the pathogenesis of Taenia saginata?
|
It is common in South and Central American and acquired by ingestion of encysted organisms (cysticerci) in beef. Results in small bowel infestation by the adult worm.
|
|
|
What is the microscopic appearance of Taenia saginata?
|
The egg is spherical, 30-40 μm, has a thick radially striated wall, and contains 3 pairs of hooks. The scolex has 4 suckers and a smooth surface (unarmed rostellum). Each proglottis is elongated and has >13 lateral uterine branches.
|
|

|
Taenia saginata.
Scolex. |
|

|
Taenia saginata.
Proglottid. |
|
|
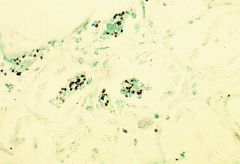
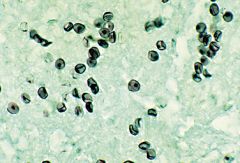
What is the microscopic appearance of Leishmania species?
|
They appear as multiple tiny 2-5 μm intracellular amastigotes within histiocytes. THe amastigote lacks an external flagellum. Appear as oval structures with a nucleus adjacent to a bar-like kinetoplast.
|
|
|
How is Leishmania species cultured?
|
It is cultured on Novy-MacNeal-Nicolle medium.
|
|
|
Which form of Leishmania species is seen on culture?
|
Promastigote.
|
|
|
What is the pathogenesis of Leishmania?
|
It is acquired from the sandfly (genuses Phlebotomuc and Lutzomyia).
|
|
|
What are the clinical manifestations of cutaneous leishmanias?
|
L. tropica, L. major, and L. aethiopica can result in a solitary cutaneous lesion that is self-limiting (L. aethiopica can dissieminate). Seen principally in the Mediterranean.
|
|
|
What does Leishmania donovani cause?
|
Widespread systemic disease (visceral leishmanias or kala azar) associated with hepatosplenomegaly and bone marrod infection. Found in Africa, Asia, India, and the Middle East.
|
|
|
What does Leishmania mexicana cause?
|
It resutls in new-world leishmania, which is a self-limiting solitary cutaneous lesion (chiclero ulcer of the ear lobe) seen in SOuth America and Texas.
|
|
|
What does Leishmania braziliensis cause?
|
It results in a form of new-world leishmaniasis known as mucocutaneous leishmaniasis that is characterized by persistent cutaneous and mucosal lesions. Seen in South and Central America.
|
|
|
Leishmaniasis.
|
|
|
Leishmaniasis.
|