![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
23 Cards in this Set
- Front
- Back
|
What are the features of torticollis? |
1. limited lateral flexion to opposite side 2. limited rotation to same side ** patient's head will tilt to the side of lesion, and rotated opposite to the side of lesion ** only painful in acute torticollis, otherwise it is painless usually |
|
|
What are the causes of torticollis? |
(A) Congenital (prenatal, delivery, postnatal): - oligohydramnios - breech/traumatic delivery - plagiocephaly and other skeletal anomaly - atlantoaxial instability - SCM tumor - kilppel feil syndrome (B) Acquired: - Muscle inflammation (myositis, TB, lymphadenitis) - PID, OM, arthritis --> irritate nerve root - benign paroxysmal torticollis, migraine variant - ocular torticollis (CN4, 6) - hearing impairment |
|

Describe identify the side of lesion |
Head lateral flexion to left Head rotation to right facial asymmetry Plagiocephaly left SCM |
|
|
Definition of scoliosis |
It is a rotational deformity of the spine, with a cobb angle of greater than 10degrees |
|
|
management of torticollis? |

below 1y/o: - passive stretching, heat, massage of SCM above 1y/o: - SCM release + halter traction/cervical orthosis post-op |
|
|
Causes of scoliosis? |
- 80% idiopathic (normally curves to the right, if it curves the other way, consider other causes) - Infantile scoliosis/ Congenital scoliosis Structural causes: - osteopathic scoliosis AKA congenital scoliosis (can be hemi-vertebrae, wedge vertebrae, block vertebrae, block vertebrae) - neuromuscular/paralytic scoliosis (due to polio,CP, myelomeningocele, muscular dystrophy etc —> leading to muscle strength imbalance) |
|
|
Signs of scoliosis? |
- Adam's bend forward test (measurement of rib hump confirms scoliosis) - abnormalabdominal reflexes (to check for cord tethering, which can be a complication/cause) - also look for stigmata ofneurocutaneous diseases - ask patient to sit down, and check if the scoliosis is resolved (to check for flexible scoliosis)- do a neurovascular examination |
|
|
Complications of scoliosis? |
visceral impingement if the cobb angle is more than 70 degrees |
|
|
Management of scoliosis? |
Depends on the Cobb's angle:
• Atcobb angle of 30 in adults, there’s a chance of future progression despiteskeletal maturity • Atcobb angle of 50, there will be a near definite future rate of progression of 1degree per year, so need surgery |
|
|
What is the epidemiology of congenital talipes equinovarus (clubfoot)? ** clubfoot is a diagnosis, clubbing of feet is a morphological description |
1-2 per 1000 live births boy:girls = 2:1 bilateral in 50% |
|
|
What is the difference between flexible club foot and structural club foot? |
Flexible club foot: - Able to dorsiflex, passively external rotate foot - Foot has full ROM - easily treated by physiotherapy and orthotics Structural club foot: - Usually idiopathic - may be due to neuro causes (CP, spina bifida, pathological peroneal nerve) - may be syndromic causes (distal type arthrogryphosis) - requires early intervention |
|
|
What are the signs of a clubfoot? |

1. posterior and medial skin creases 2. Cavus (of midfoot) 3. Adduction (of metatarsus in forfoot) 4. Varus (of hindfoot) 5. Equinus (of heel) ** watch out for calf wasting |
|
|
Management of clubfoot? |
conservative: 1. serial manipulation and casting (Ponseti method) - supinate forefoot to reduce cavus, abduct forefoot, heel valgus force, KIV TA tenotomy for equinus deformity - weekly manipulations - repeat manipulation till external rotation of 60 degrees achieved - do this for 4 months 2. followed by dennis brown boots to maintain correction (23h/day for 3 months, then wean until child begins to cruise, then night and nap till 4 y/o) Surgical: - tibial tendon lengthening - tendon release - tendon transfer - bone surgery (corrective osteotomy/fusion) |
|

What is this? |
ponsetti cast |
|

What is this? |
dennis browne bar and boots (ankle foot orthosis) |
|
|
what is Klipel feil syndrome? what is the triad? what is it associated with? |
1. characterized by the congenital fusion of any two of the seven cervical vertebrae 2. a)restricted mobility of the neck and upper spine b)short neck c)low hairline at the back of the head 3. scoliosis, spina bifida, sprangel's deformity, cleft palate and many others |
|
|
What is pes planus? What are the signs of pes planus? |
1. collapse of arch of foot, with the entire sole coming into contact with the ground 2. forefoot: pronation, may have hallux valgus and bunion midfoot: collapse of arch hindfoot: heel valgus, too many toes sign special tests: (a) tip-toe/dorsiflex foot (b) Jack's test (c) beighton score |
|
|
What are the causes of pes planus? |
1. Infantile pes planus --> congenital vertical talus 2. Children/adolescent flexible pes planus --> either generalized ligamentous laxity OR tight tendo-achilles tendon OR collagen disorders 3. Rigid pes-planus - bone: tarsal coalition - muscle: CP - ligaments: Marfan's, Ehler Danlos - idiopathic 4. Adult pes planus: - RA - posterior tibial tendon dysfunction (rupture/synovitis) --> palpate for tenderness along muscle tendon behind the medial malleolus |
|
|
management of pes planus? (depends on etiology) |
General advice: - rocker bottom shoes, medial arch support (in-soles) TA tightness: TA stretching posterior tibialis dysfunction: operative repair/tendon replacement if there is a rupture of PTT rigid pes planus: KIV operation |
|
|
What are the causes of in-toeing gait? |
1. Physiological (usually bilateral): - metatarsal adduction (forefoot) - internal tibial torsion - femoral anteversion 2. Pathological* (TRO): - Neuromuscular diseases (eg, cerebral palsy) - Disorders of the hip (eg. DDH/perthes/SCFE) - Lower leg deformities (eg, clubfoot, skewfoot) |
|
|
What are the normal age of onset for metatarsal adduction, internal tibial torsion, femoral anteversion etc? |

- metatarsal adduction resolves by 1 y/o - internal tibial torsion resolves by 5 y/o - femoral anteversion resolves by 11 y/o - only femoral anteversion have patella pointing internally |
|
|
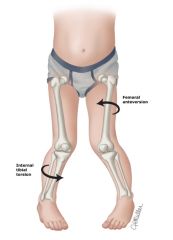
example of femoral anteversion and internal tibial torsion |
|
|
what is athrogryposis |
Arthrogryposis, or arthrogryposis multiplex congenita (AMC), comprises of nonprogressive conditions characterized by multiple congenital joint contractures |