![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
101 Cards in this Set
- Front
- Back
|
list 10 parts of the screening neuro exam |
1. Well vs. Unwell 2. Vitals 3. GA 4. Mental status 5. Handedness 6. Cranial nerves 7. Motor 8. Sensory 9. Coordination/cerebellar 10. Gait |
|
|
frontal release signs? (included under mental status) |
Glabellar tap.. |
|
|
4 parts of motor exam |
1. tone (screen UMN with pronator drift) 2. bulk 3. strength 4. reflexes |
|
|
4 parts of sensory exam |
1. light touch 2. pain/temp 3. proprioception (very SMALL movements) 4. vibration |
|
|
parts of coordination/cerebellar exam 6 |
1. bradykinesia 2. coordination 3. tremor 4. nystagmus 5. hypotonia, pendular reflexes) 6. dysarthria |
|
|
parts of Gait exam 8 |
1. rhomberg here as they are standing 2. rising from a chair 3. posture 4. arm swing 5. "base" of the gait (wide or narrow) 6. stride length/height 7. turning 8. add'l maneuvers as required |
|
|
examining for diplopia |
d |
|
|
General inspection of eyes |
trauma, inflammation, erythema, discharge |
|
|
Exam of CN II 6 big points to hit |
1. visual acuity with snellen chart 2. colour perception 3. visual fields 4. examine pupils via light reflex 5. check for accommodation 6. fundoscopic exam |
|
|
note on VA : test one eye at a time! |
k |
|
|
color perception: |
test red perception on snellen chart |
|
|
2 rules for examining visual fields |
1. only test one eye at a time 2. compare to your field of vision. if testing left eye, close your right eye and only do things you can see |
|
|
visual fields: 2 methods |
1. static technique 2. kinetic technique |
|
|
how to examine light reflex |
1. ensure room is dim 2. shine light between eyes, check that both peoples constrict 3. If anisocoria present, move to CN III exam 4. if anisocoria absent, proceed to swinging flashlight test 5. if pupils do not react, check for argyle robertson pupil |
|
|
HOW to check for argyle robertson pupil |
= bilateral small pupils that reduce in size when the patient focuses on a near object (they accommodate) but do not constrict when exposed to bright light |
|
|
how to check for accommodation |
have patient fix on a point far away and then suddenly look at at an object eg finger that moves close to their face. |
|
|
Next: exam of III, IV, and VI first glance: how do palsies of each of these present? |
III: down and lateral IV: eye up and medial VI: eye directed medially |
|
|
lids; significance of ptosis |
suggests CN III palsy or myasthenia gravis |
|
|
Thyroid opthalmopathy) 4 |
proptosis, lid edema, lid lag, lid retraction? |
|
|
examining for diplopia: explain the cover/uncover test |
1. monocular if diplopia extinguishes with one eye covered but not with the other eye covered 2. binocular if diplopia vanishes with either eye covered 3. monocular: suggests optho etiology, binocular suggests neuro/muscular cause |
|
|
if binocular diplopia detected, determine : which mm is weak and which eye is the problem? |
which mm is weak: which direction makes the diplopia worse narrows it down to two possible extraocular mm. which eye is the problem: use red glass. the most peripheral image belongs to the affected eye or ask patient to close one eye: if the more peripheral image is extinguished, that is the affected eye. |
|
|
CN VI palsy: what is one thing that can exacerbate diplopia |
distance vision will cause diplopia |
|
|
how to test for CN IV palsy |
ask pt to tilt head towards affected side. CN IV palsy shows hypertropia |
|
|
stroke vs bells palsy (essentially UMN vs. LMN cranial nerve findings) |
d |
|
|
CN II: how would stroke affect visual field |
depends on site of lesion.. homonymous hemianopia or quadrantanopia |
|
|
how would stroke affect visual acuity? |
should be normal.. |
|
|
stroke: what would findings in pupillary response to light and accommodation? |
normal exam in stroke (unless brainstem? or horners) |
|
|
swinging flashlight test in stroke |
should be normal. both pupils should constrict strongly RAPD is an issue with CN II .. |
|
|
review: triad of horner's syndrome |
ipsilateral miosis, ptosis, and anhidrosis |
|
|
stroke: III, IV, and VI |
binocular diplopia possible. also note gaze preference towards side of lesion |
|
|
checking V: sensation: |
both sides, 3 divisions 1. light touch: test with cotton/kleenex 2. pain sensation stroke: sensation may be diminished in hemi distribution |
|
|
Motor exam of V |
1. mm wasting 2. clench teeth, feel masseters 3. test pterygoids: ask patient to open their mouth against your hand |
|
|
V: jaw jerk reflex |
jaw jerk reflex. mouth hanngs loosely open. use finger as a brace, hit with hammer, and look for reflex closing of jaw. unilateral stroke: jaw jerk testing usually normal |
|
|
V: corneal reflex |
touch cornea, look for direct and consensual blink may be absent in brainstem stroke |
|
|
afferent and efferent component of corneal reflex |
afferent: CN V efferent: CN VII |
|
|
VII: facial nerve Inspection |
facial symmetry and presence of passive motor signs possible changes to tearing? and may report changes to hearing (hyperacusis via stapedius involvement) |
|
|
signs of VII involvement (stroke or bell's palsy) |
nasolabial fold flattening, mouth droop, retracted eyelids, other asymmetry |
|
|
VII: motor exam 4 |
1. forehead wrinkling (absent = LMN. able to wrinkle = UMN) NB 2. close eyes tightly, resist you trying to open them 3. puff out cheeks 4. show teeth |
|
|
quick screen for VIII |
hearing acuity: rub fingers toogether at side of patients head: move inward till patient hears noise. compare with other side |
|
|
IX and X: sensory |
gag reflex (plus taste to posterior 1/3 of tongue, which we don't test here) |
|
|
IX and X: motor 3 |
say "AH" to check palatal elevation have patient drink water and assess swallowing comment on gag reflex, but don't check... |
|
|
findings if there's a lesion to IX, X? |
in brainstem stroke, asymmetric absence of gag reflex and / or dysphagia may occur.. diminished palate elevation may occur ipsilateral |
|
|
testing XI |
cortical stroke: patient may have weakness in ipsilateral SCM and contralateral trapezius...? |
|
|
testing XII |
ask patient to stick out tongue branstem stroke: deviates to side of lesion cortical stroke: away from side of lesion |
|
|
Motor exam: inspection |
bulk, atrophy, fasciculations (no suspected abnormality in acute stroke) |
|
|
Motor exam: tone |
1. flaccid (LMN) 2. velocity dependent = spastic (stroke) 3. rigid = velocity independent (Parkinson's?) |
|
|
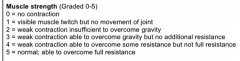
scale for testing muscle strength |
|
|
|
note: how does UMN lesion affect upper and lower limb strength? |
Flexion predominates in upper limb, extension predominates in lower limb |
|
|
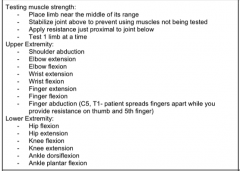
testing mm strength: list that goes through the exam |
|
|
|
Motor exam: 4 tests to do after strength |
+ reflexes!! |
|
|
when to perform coordination and gait? |
|
|
|
exam of arm weakness (UMN vs LMN) |
d |
|
|
arm weakness: Inspection 3 |
1. Bulk (mainatined in UMN, down in LMN) 2. fasciculation (LMN) 3. position of arm (decerebrate posture = UMN) |
|
|
arm weakness: Motor exam 0. pronator drift 1. check tone 2. list the myotomes you would check |

|
|
|
arm weakness: motor exam 1. check arm reflex 2. special test... |

|
|
|
arm weakness: sensory exam: 1. which dermotomes to check? 2. findings if anterolateral pathway disrupted? 3. findings if DCML disrupted |
anterolateral: pain, temp, light touch DCML: proprioception, vibration, light touch |
|
|
notes: 1. demonstrate on one side, and state that you would compare with the other side of the body 2. offer to demonstrate techniques |
k |
|
|
If UMN signs found when examining arm, what else might be present given left arm weakness is due to a right cortical lesion? 4 |
1. left lower face droop with forehead sparing 2. cortical sensation loss: 2 point discrim, stereognosis, graphesthesia, localization of tactile stimulus, extinction 3. extension of leg (spastic paralysis) 4. left visual field neglect |
|
|
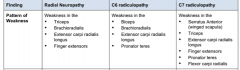
patterns of weakness that would be characteristic of 1. Radial neuropathy 2. C6 radiculopathy 3. C7 radiculopathy |
j |
|
|
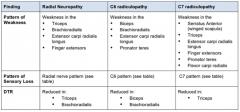
Patterns of sensory loss AND DTRs in 1. radial neuropathy 2. C6 radiculopathy 3. C7 radiculopathy |
|
|

|
k |
|
|
onto exam of Foot drop. ddx of foot drop? 3 |
1. sciatic nerve 2. peroneal nerve 3. L5 radiculopathy |
|
|
foot drop-motor exam. strength testing if peroneal nerve injury? 3 |
weak ankle dorsiflexsion (tib ant.), eversion (peroneus), and toe extension (ext dig.) |
|
|
foot drop-motor exam. strength testing if L5 radiculopathy 6 |
1. weak ankle dorsiflexion 2. weak plantarflexion (gastroc) 3. hip extension (glut max) 4. hip abduction (glut med) 5. knee flexion (hamstrings) 6. toe extension (ext dig |
|
|
foot drop-motor exam. strength testing findings of sciatic nerve injury |
1. ankle dorsiflexion (tib ant) 2. eversion 3. knee flexion 4. ankle plantarflexion 5. ankle inversion 6. toe exetnsion |
|
|
suggested approach to foot drop wrt order of testing weakness. NB |
1. test sciatic: IF a) plantarflexion and b) toe flexion are intact, tibial nerve and therefore sciatic is intact. 2. THEN distinguish L5 from peroneal by testing a) knee flexion b) hip extension c) hip abduction all of these are innervated by L5, but are above peroneal nerve. |
|
|
foot drop-motor exam. reflexes explain significance of achilles reflex finding |
peroneal nerve does NOT contribute to achilles reflex. therefore, if diminished or absent, suggests sciatic neuropathy or L5 radiculopathy |
|
|
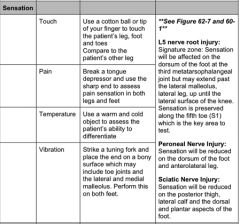
sensory testing in foot drop. summary given here, refer to tables for details .. |
|
|
|
note: sensory distributions for L5, sciatic, and peroneal n. |

|
|
|
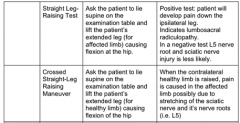
special tests for sciatic neuropathy/L5 radiculopathy |
|
|
|
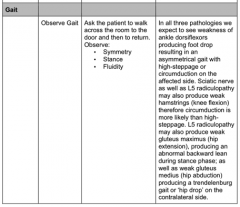
gait in peroneal vs. sciatic vs. L5 |
|
|
|
Examination of cerebellar ataxia prompt: seeing a patien twith pernicious anemia and who is also a heavy alcoholic.. differentiate sensory ataxia from a dorsal column issue or cerebellar ataxia |
d |
|
|
general appearance: 1 relevant finding related to speech, in addition to well/unwell, etc. |
cerebellar ataxia: patient may have dysarthria. slurred, slow, and irregular in rhythm and volume |
|
|
Cranial nerves, motor, and reflexes.. not expected to complete in this particular prompt |
d |
|
|
Sensory exam in ataxia : relevant findings with light touch, temp and pain? |
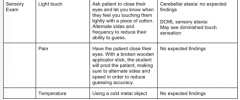
may see dimiished light touch if DCML sensory ataxia |
|
|
sensory exam in ataxia: how to assess vibration? |
check against bony prominennces. begin with sternum. test the distal interphalangeal joints first. if the patient can feel those, there is no need to test proximally |
|
|
vibration: findings in ataxia? |
cerebellar: no findings DCML sensory ataxia: diminished vibration sense |
|
|
ataxia: how to test proprioception |
grasp patients toe or finger lightly at the sides and bend it up and down. with patient watching, demonstrate UP and DOWN. Have patient close their eyes, and ask if they detect motion, and which direction it is. |
|
|
proprioception: findings in ataxia 3 |
normal: this may be incorrect 10% of time cerebellar ataxia: no expected finding DCML ataxia: poor detection |
|
|
onto special tests.. list the special tests to do in cerebellar ataxia 6 |
1. finger-nose test
2. heel-knee-shin 3. dysdiadochokinesia 4. hypotonia 5. nystagmus 6. rhomberg |
|
|
and don't forget Gait! findings in cerebellar vs. sensory ataxia |
cerebellar: wide based gait, staggering or swaying possible DCML sensory ataxia: patient looks down, walks as if throwing feet, feet slap ground. "high-steppage gait" |
|
|
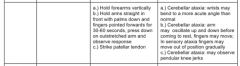
how to perform finger nose testing? relevant findings? |

|
|
|
heel knee shin testing.. how to perform relevant findings |
1. ask P to move heel of one leg down the shin of opposite leg. repeat on other side 2. cerebellar ataxia: may notice decompensation of movement. ie. patient moving heel abnormally high before starting the maneuver. |
|
|
4 tests for dysdiadochokinesia + relevant findings |
1. forearm pronation an supination 2. hand clapping 3. finger tapping? 4. foot stamping in cerebellar ataxia, may notice slower speed and irregular rhythm, range, and accuracy. dysdiadochokinesia = inability to perform rapid movements |
|
|
how to assess for hypotonia
|
stabilize joint from above and passively flex and extend limb in slow, repetitive fashion. compare with other side. tone may be reduced |
|
|
wtf? |
|
|
|
what type of nystagmus consistent with cerebellar lesion? |
conjugate horizontal jerk nystagmus (both eyes moving together, with an abnormal slow drifting in one direction, than fast jerk in other direction. NOT expected in DCML sensory ataxia... |
|
|
romberg test: |
ask patient to stand with feet together and closed eyes for 60 sec. look for swaying. only positive in sensory ataxia |
|
|
fundamental signs of cerebellar ataxia? 4 |
1. cerebellar gait 2. nystagmus 3. hypotonia 4. dysarthria |
|
|
fundamental signs of DCML sensory ataxia |
1. high-steppage gait 2. positive rhomberg 3. impaired proprioception 4. impaired vibration in affected limbs |
|
|
Parkinson's checklist |
d |
|
|
PD: GA and vitals |
comment and offer to assess.. |
|
|
PD: inspection. 6 points |
1. resting tremor 2. dry skin (xeroderma) 3. decreased blinking 4. hypersalivation 5. lack of facial expression w/ conversation 6. softened, breathy voice |
|
|
features of resting tremor 5 |
1. slow frequency tremor upon resting limb 2. asymmetrical 3. classic pill-rolling tremor 4. aggravated by stress 5. inhibited by movement |
|
|
PD: 4 special tests to hit |
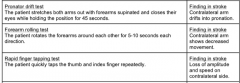
1. bradykinesia 2. glabellar tap 3. test rigidity 4. parkinsonian gait |
|
|
how to test bradykinesia (4) |
1. tap fingers, beginning with index finger and moving laterally 2. inching and circling: patient rapidly pinches together index finger and thumb of one hand while simultaneously performing a circling movement with the index finger of their opposite hand. instruct p. to direct gaze towards the circling finger to distract. 3. twiddling: patient rapidly circumducts their hands over each other. inspect for asymmetry of movement 4. tapping of heels, one foot at a time |
|
|
glabella tap reflex |
percuss patients forehead with index finger. both eyes should reflexly blink blinking should extinguish after 5-10 cycles. persistent blinking is positive sign (Myerson sign) |
|
|
how to test rigidity |
1. pick a joint: elbow, wrist, ankle 2. pick a side: the side with the most prominent tremor 3. passively range the joint 4. feel for "lead pipe rigidity" or cogwheeling (alternating periods of resistance and relaxation) |
|
|
note: why to test rigidity slowly |
make sure the increased tone is not velocity dependent |
|
|
features of parkinsonian gait |
1. flexed posture of neck, trunk, hips, arms 2. difficulty initiating gait, freezing, en block turning 3. small, flat footed shuffling steps with narrow base 4. diminished arm swing 5. festination (involuntary speeding up) 6. retropulsion: poor postural control. stand in front of wall with patient in front of you, while giving them a pull from behind |
|
|
what are 5 features that suggest a parkinson plus syndrome |
1. marked autonomic dysfunction (postural hypotension, neurogenic bladder or bowel 2. early severe dementia 3. pyramidal findings (any UMN. hyperreflexia, spasticity, babinski) 4. cerebellar findings (limb ataxia, gait ataxia, nystagmus) 5. supranuclear gaze palsy (difficulty looking down) |