![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
76 Cards in this Set
- Front
- Back

|
COLOBOMA Defective closure of embryonic fissure Usually inferior nasal Manage refractive error Evaluate for other congenital anomalies Possible specialized CL |
|

|
PERSISTENT PUPILLARY MEMBRANE Most common ocular congenital anomaly More common in dark eyes (80% of dark eyes, 35% light eyes) Type 1: Only attached to iris Type 2: Iridolenticular adhesions If problematic, YAG laser |
|

|
HETEROCHROMIA IRIDIS Unilateral 2 colors, 1 iris Remove foreign bodies Manage uveitis |
|

|
HETEROCHROMIA IRIDUM Bilateral, different colored irises Remove foreign bodies Manage uveitis |
|

|
RUBEOSIS IRIDES Neovascularization of iris and angle Due to ocular ischemia, most commonly diabetic retinopathy Usually requires PRP Intra-vitreal anti VEGF (Avastin) |
|

|
RUBEOSIS IRIDES Abnormal blood vessels on iris (usually at pupillary margin) Usually requires PRP Intra-vitreal anti VEGF (Avastin) |
|

|
RUBEOSIS IRIDES Asymptomatic if no angle involvement Can cause neovascular glaucoma Usually requires PRP Intra-vitreal anti VEGF (Avastin) |
|

|
Aniridia Abnormal iris development due to genetic mutation Predisposes patient to Wilm's Tumor (life threatening) 3 classifications (AD, Sporadic, Gillespie Syndrome) |
|

|
Aniridia Abnormal iris development due to genetic mutation Predisposes patient to Wilm's Tumor (life threatening) 3 classifications (AD (66%), Sporadic (33%), Gillespie Syndrome (<1%)) |
|

|
Aniridia Abnormal iris development due to genetic mutation Predisposes patient to Wilm's Tumor (life threatening) 3 classifications (AD (66%), Sporadic (33%), Gillespie Syndrome (<1%)) |
|

|
ANIRIDIA demonstrates MGD Dry Eye and Limbal stem cell deficiency |
|

|
ANIRIDIA 75% of cases develop glaucoma Onset late childhood |
|

|
ANIRIDIA Lens subluxation (superiorly), cataract, or aphakia Often surgical intervention Artificial pupil Manage symptoms/conditions (cataract, glaucoma, etc) |
|

|
ANIRIDIA Foveal Hypoplasia, ONH hypoplasia, choroidal coloboma Often surgical intervention Artificial pupil Manage symptoms/conditions (cataract, glaucoma, etc) |
|

|
IRIDOCORNEAL ENDOTHELIAL SYNDROME (ICE) Unilateral Middle aged women Associated with glaucoma (50%) 3 types (Essential Iris Atrophy, Chandler's Syndrome, Cogen Reese Syndrome) Manage glaucoma Trabeculoplasty and trabculectomy often unsuccessful Often requires filtering shunt |
|

|
ICE - Essential Iris Atrophy hammered silver endothelium Progressive severe iris changes |
|

|
ICE - Chandler's Syndrome hammered silver endothelium Mild Iris Changes |
|

|
ICE- Cogan Reese Syndrome hammered silver endothelium Iris nevus syndrome Iris Atrophy absent in 50% (mild in the rest) Severe corectopia |
|

|
ICE Corneal endothelium flakes off and moves to iris where it blocks outflow = glaucoma (50%) |
|

|
ICE may need corneal transplant |
|

|
ICE may need corneal transplant |
|

|
Primary Epithelial Iris Cyst at pupil border Argon laser photocoagulation |
|

|
Primary Epithelial Iris Cyst at iris root Argon laser photocoagulation |
|

|
Primary Stromal Iris Cyst Onset in 1st years of life Needle aspiration/Surgical excision Inject ethanol for 60 seconds to eliminate recurrence Spontaneous regression has been noted |
|

|
Secondary Iris Cyst Implanted: Pearl |
|

|
Secondary Iris Cyst Implanted: Serous |
|

|
Secondary Iris Cyst Miotic Induced |
|

|
Secondary Iris Cyst Parasitic |
|

|
Brushfield Spots (associated with Down's Syndrome) |
|

|
Lisch Nodules Associated with Neurofibramoatous 1 |
|

|
Inflammatory Nodules Busacca Nodules Anterior iris surface |
|

|
Inflammatory Nodules Koeppe Nodules Pupillary border |
|

|
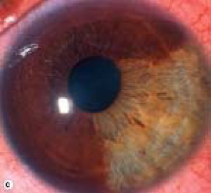
Iris Nevus Less than 3mm in diameter |
|
|
Iris Nevus Usually inferior |
|

|
Diffuse Iris Nevus |
|

|
Iris Nevus Syndrome (Cogan Reese Syndrome) |
|

|
Iris Melanoma |
|

|
Iris Melanoma |
|

|
Iris Melanoma |
|

|
Iris Melanoma |
|

|
Iris Melanoma |
|

|
Iris Melanoma |
|

|
Iris Melanoma Tapioca Melanoma |
|

|
Iris Melanoma Diffuse (Loss of crypts of fuch) |
|

|
Iris Melanoma (Hyphema) |
|

|
Iris Metastatic Tumor |
|

|
Iris Metastatic Tumor |
|

|
Iris Metastatic Tumomr (Retina looks like breast cancer metastasis - creamy, fluffly, lumpy) |
|

|
Preseptal cellulitis Infection anterior to orbital septum Staph infection, hordeolum, dacryocystitis, sinusitis, URI NO PROPTOSIS, O.N. PROBLEMS, OR EOM PAIN/HINDERING Systemic: Augmentin 250-500 mg tid Bactrim in PCN allergy Topicals dont help much, but would use Vigamox qid If severe- Admit to hospital- Antibiotic IV: Vancomycin |
|

|
Preseptal cellulitis Infection anterior to orbital septum Staph infection, hordeolum, dacryocystitis, sinusitis, URI NO PROPTOSIS, O.N. PROBLEMS, OR EOM PAIN/HINDERING Systemic: Augmentin 250-500 mg tid Bactrim in PCN allergy Topicals dont help much, but would use Vigamox qid If severe- Admit to hospital- Antibiotic IV: Vancomycin |
|

|
Preseptal cellulitis Infection anterior to orbital septum Staph infection, hordeolum, dacryocystitis, sinusitis, URI NO PROPTOSIS, O.N. PROBLEMS, OR EOM PAIN/HINDERING Systemic: Augmentin 250-500 mg tid Bactrim in PCN allergy Topicals dont help much, but would use Vigamox qid If severe- Admit to hospital- Antibiotic IV: Vancomycin |
|

|
Orbital cellulitis Infection posterior to orbital septum (life/sight threatening) Most commonly from ethmoid sinusitis Also from Dacrocystitis, dental decay, trauma, orbita surgery, preseptal cellulitis extension Admit to hospital- IV antibiotics Monitor ON function every 4 hours Freq. Fatal with mucormycosis |
|

|
Orbital cellulitis Infection posterior to orbital septum (life/sight threatening) Most commonly from ethmoid sinusitis Also from Dacrocystitis, dental decay, trauma, orbita surgery, preseptal cellulitis extension Admit to hospital- IV antibiotics Monitor ON function every 4 hours Freq. Fatal with mucormycosis |
|

|
Orbital cellulitis Infection posterior to orbital septum (life/sight threatening) Most commonly from ethmoid sinusitis Also from Dacrocystitis, dental decay, trauma, orbita surgery, preseptal cellulitis extension Admit to hospital- IV antibiotics Monitor ON function every 4 hours Freq. Fatal with mucormycosis |
|

|
Orbital cellulitis Infection posterior to orbital septum (life/sight threatening) Most commonly from ethmoid sinusitis Also from Dacrocystitis, dental decay, trauma, orbita surgery, preseptal cellulitis extension Admit to hospital- IV antibiotics Monitor ON function every 4 hours Freq. Fatal with mucormycosis |
|

|
Orbital cellulitis Infection posterior to orbital septum (life/sight threatening) Most commonly from ethmoid sinusitis Also from Dacrocystitis, dental decay, trauma, orbita surgery, preseptal cellulitis extension Admit to hospital- IV antibiotics Monitor ON function every 4 hours Freq. Fatal with mucormycosis |
|

|
Orbital cellulitis Infection posterior to orbital septum (life/sight threatening) Most commonly from ethmoid sinusitis Also from Dacrocystitis, dental decay, trauma, orbita surgery, preseptal cellulitis extension Admit to hospital- IV antibiotics Monitor ON function every 4 hours Freq. Fatal with mucormycosis |
|

|
Orbital cellulitis Infection posterior to orbital septum (life/sight threatening) Most commonly from ethmoid sinusitis Also from Dacrocystitis, dental decay, trauma, orbita surgery, preseptal cellulitis extension Admit to hospital- IV antibiotics Monitor ON function every 4 hours Freq. Fatal with mucormycosis |
|

|
HSV >80% of population over 20 infected < 6% manifest symptoms 2nd most common venereal disease Leading cause of infectious blindness in US 60% of corneal ulcers in developed countries are due to HSV 10 million ppl with herpetic eye disease |
|

|
HSV >80% of population over 20 infected < 6% manifest symptoms 2nd most common venereal disease Leading cause of infectious blindness in US 60% of corneal ulcers in developed countries are due to HSV 10 million ppl with herpetic eye disease |
|

|
HSV 1 Upper body usually Direct contact transmission |
|

|
HSV 2 Lower body usually Sexual and neonatal transmission |
|

|
HSV - Primary Ocular Infection 94% subclinical 54% blepharoconjunctivitis 63% keratitis |
|

|
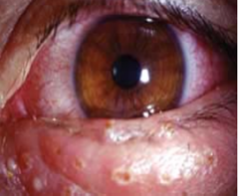
HSV BLEPHAROCONJUCTIVITiS Periocular Vesicles, Follicular conjunctivitis Ipsilateral PAL Drying Agents: Calamine Lotion, Camphor Oil, 70% alcohol Secondary Infection = Antibiotic ointment Systemic Antivirals : Acyclovir 400 mg 5x/d 1wk Valtrex: 1 g 1x/d 1wk Topical Antivirals: Viroptic 9x/d 1-2 wks Zirgal gel 5x/d 1-2 wks |
|
|
HSV BLEPHAROCONJUCTIVITiS Periocular Vesicles, Follicular conjunctivitis Ipsilateral PAL Drying Agents: Calamine Lotion, Camphor Oil, 70% alcohol Secondary Infection = Antibiotic ointment Systemic Antivirals : Acyclovir 400 mg 5x/d 1wk Valtrex: 1 g 1x/d 1wk Topical Antivirals: Viroptic 9x/d 1-2 wks Zirgal gel 5x/d 1-2 wks |
|

|
HSV KERATITIS Dendritic ulver with terminal buds |
|

|
HSV Keratitis NO STEROIDS Self resovling, but has a lot of scarring and neo Cycloplegic: Cyclogyl 1% bid ATs Top. Antirvirals: Viroptic 9x/day, Zirgan gel 5x/d Debridement Oral Antivirals: Acyclovir 400 mg 5x/day 1-2 wks Valcyclovir 500 mg tid 1-2 wks |
|

|
Infectious epithelial keratitis Looks like primary keratitis Dendritic pattern preceded by punctate staining |
|

|
Post-infectious keratitis Failure for proper re-epithelialization after an ucler has healed Bandage CL with Antibiotic Prophylaxis: Vigamox qid Muro 128 Antivirals generally not needed Avoid Steroids if possible |
|

|
Post-infectious keratitis Failure for proper re-epithelialization after an ucler has healed Bandage CL with Antibiotic Prophylaxis: Vigamox qid Muro 128 Antivirals generally not needed Avoid Steroids if possible |
|

|
Interstitial stromal keratitis Viral replication in the stroma Cycloplegic: Cyclogyl 1% bid Top. Steroid: Pred forte qid, long taper Antivirals: Topical- Viroptic qid, Zirgan tid-qid Oral- Acyclovir 400 mg po bid |
|

|
Interstitial stromal keratitis Viral replication in the stroma Cycloplegic: Cyclogyl 1% bid Top. Steroid: Pred forte qid, long taper Antivirals: Topical- Viroptic qid, Zirgan tid-qid Oral- Acyclovir 400 mg po bid |
|

|
Disciform Stromal Keratitis HSV infection of corneal endothelium or hypersensitivity to virus Cycloplegic: Cyclogyl 1% bid Top. Steroid: Pred forte qid, long taper Antivirals: Topical- Viroptic qid, Zirgan tid-qid Oral- Acyclovir 400 mg po bid |
|

|
Disciform Stromal Keratitis HSV infection of corneal endothelium or hypersensitivity to virus Cycloplegic: Cyclogyl 1% bid Top. Steroid: Pred forte qid, long taper Antivirals: Topical- Viroptic qid, Zirgan tid-qid Oral- Acyclovir 400 mg po bid |
|

|
DISCIFORM STROMAL KERATITIS Wesley's Ring- Antibody/antigen ring surrounding edema |
|

|
IRIDOCYCLITIS High IOP due to trabeculitis Cycloplegic- cyclogyl 1% bid Topical steroids- Pred Forte qid or q1h If IOP is high, Timolol 0.5% bid Antiviral- Viroptic 9x/day, Acyclovir 400 mg 5x/day NO PROSTAGLANDINS |