Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
195 Cards in this Set
- Front
- Back
|
Left brain
|
Language
sequence and perform movements, produce written and spoken language, analytic, controlled logical rational mathematical calculations express positive emotions process verbally coded information in an organized, logical and sequential manner |
|
|
Right brain
|
Non-verbal processing
Holistic processing of information Art General concept comprehension Hand-eye coordination Spatial relationships Kinesthetic awareness Understand music Understand nonverbal communication Mathematical reasoning Express negative emotions Body image awareness |
|
|
Barognosis
|
perceive the weight of different objects in the hand
|
|
|
Graphesthesia
|
identify a number or letter drawn on skin
|
|
|
Kinesthesia
|
direction and extent of movement of a joint or body part
|
|
|
Stereognosis
|
identify an object without sight - using the sense of touch
|
|
|
Allodynia
|
the sensation of pain in response to a stimulus that would not typically produce pain
|
|
|
Analgesia
|
absence of pain while remaining conscious
|
|
|
Anesthesia
|
absence of touch sensation
|
|
|
Causalgia
|
constant, relentless, burning hyperesthesia and hyperalgesia that develops after a peripheral nerve injury
|
|
|
Dysesthesia
|
distortion of any of the senses, particularly the sense of touch
|
|
|
Hyperpathia
|
extreme or exaggerated response to pain
|
|
|
Hypesthesia
|
diminished sensation of touch
|
|
|
Neuralgia
|
severe and multiple shock-like pains that radiate from a specific nerve distribution
|
|
|
Pullanesthesia
|
loss of vibration sensation
|
|
|
Chorea
|
form of hyperkinesia with brief, irregular contractions that are rapid, but not myoclonic
- related to damage to caudate nucleus - Huntington's disease |
|
|
Huntington's disease
|
Degeneration of basal ganglia (primarily the striatum)
Autosomal dominant Enlarged ventricles Extensive loss of quantity and activity of gamma-aminobutyric acid (GABA) and acetylcholine neurons Symptoms include chorea, bradykinesia, and rigidity; affective dysfunction, and cognitive impairment; speech disorders; unintentional facial expressions, tounge protrusion, eyebrow elevation. Eventually progresses to dementia, depression, dysphagia, incontinence, inability to ambulate/transfer, progression to rigidity Average age of onset - 35-55 years Fatal within 15-20 years of onset |
|
|
Bradykinesia
|
Abnormal slowness of movement
|
|
|
Dystonia
|
sustained involuntary muscle contractions frequently causing twisting, abnormal postures, and repetitive movements
Caused by genetic, acquired, secondary to medication; Parkinson's, CP, encephalitis |
|
|
Athetosis
|
Movement disorder with slow, twisting, writhing movements in a large amplitude
Primarily in face, tongue, trunk, and extremities Brief - "merge" with chorea Sustained - "merge" with dystonia Common finding in several forms of CP secondary to basal ganglia pathology |
|
|
Basal Ganglia
|
Gray matter masses located deep within the white matter of the cerebrum and include the caudate, putamen, globus pallidus, substantia nigra, & subthalamic nuclei.
Collectively responsible for voluntary movement, muscle tone, and control of motor responses. Dysfunction - Parkinson's, Huntington's, Tourettes, ADD, OCD, addictions. |
|
|
Agnosia
|
inability to interpret information
|
|
|
Agraphia
|
inability to write due to a lesion within the brain; typically found in combination with aphasia
|
|
|
Alexia
|
inability to read or comprehend written language secondary to a lesion within the dominant lobe of the brain
|
|
|
Anosognosia
|
The denial or unawareness of one's illness; often associated with unilateral neglect
|
|
|
Apraxia
|
inability to perform purposeful learned movements or activities even though there is no sensory or motor impairment that would hinder completion of the task
A disorder of motor planning |
|
|
Constructional apraxia
|
Inability to reproduce geometric figures and designs. A person is often unable to visually analyze how to perform a task
|
|
|
Decerebrate rigidity
|
Extension of trunk and all extremities
Characteristic of corticospinal lesion at the level of the brainstem |
|
|
Decorticate rigidity
|
Trunk and LE extension, UE flexion
Characteristic of corticospinal lesion at the level of the diencephalon |
|
|
Corticospinal tract
|
Descending - pyramidal motor tract
Anterior - ipsilateral voluntary, discrete, and skilled movements Lateral - contralateral voluntary fine movement Damage to corticospinal tract results in positive Babinski, absent superficial abdominal reflexes & cremasteric reflex, and loss of fine motor or skilled voluntary movement |
|
|
Cremasteric reflex
|
L1-L2
Scratch the skin of the upper medial thigh -> brisk and brief elevation of the testicle on the ipsilateral side |
|
|
Diencephalon
|
Located beneath the cerebral hemispheres and contains the thalamus, hypothalamus, subthalamus, epithalamus.
Where the major motor and sensory tracts synapse. Acts as an interactive site between the CNS and endocrine system, as well as complimenting the limbic system. |
|
|
Dysarthria
|
slurred and impaired speech due to a motor deficit of the tongue or other muscles essential for speech
|
|
|
Dysprosody
|
Impairment in the rhythm and inflection of speech
|
|
|
Emotional lability
|
characteristic of a R hemisphere infarct where there is an inability to control emotions and outbursts of laughing or crying that are inconsistent with the situation
|
|
|
Fluent aphasia
|
characteristic of receptive aphasia (wernicke's)
A person with this aphasia speaks normally but uses random or invented words; leaves out key words; substitutes words or verb tenses, pronouns, or prepositions; and utters sentences that do not make sense Includes Wernicke's Aphasia & Conduction Aphasia |
|
|
Wernicke's Aphasia
|
Lesion - posterior region of superior temporal gyrus
Also known as "receptive aphasia"; a type of fluent aphasia Comprehension (reading/auditory) is impaired Good articulation, use of paraphasias Impaired writing Poor naming ability Motor impairment not typical due to distance from Wernicke's area to the motor cortex |
|
|
Broca's Aphasia
|
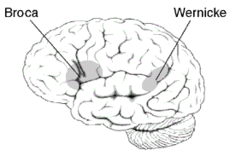
Non-fluent aphasia
"Expressive aphasia" Most common form of aphasia Frustration and language skill errors |
|
|
Paraphasias
|
Production of unintended syllables, words, or phrases during the effort to speak
Most common in patients with fluent forms of aphasia |
|
|
Conduction Aphasia
|
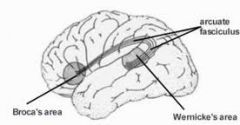
Lesion to supramarginal gyrus, arcuate fasciculus.
Severe impairment with repetition. Intact fluency, good comprehension. Speech interrupted by word-finding difficulties. Reading in-tact; writing impaired. |
|
|
Global Aphasia
|
Non-fluent aphasia
Lesion to frontal, temporal, parietal lobes, Comprehension, naming, writing, repitition skills severely impaired. May involuntarily verbalize, usually without correct context. Nonverbal skills used for communication |
|
|
Verbal apraxia
|
verbal expression is impaired secondary to deficits in motor planning
They are unable to initiate learned movements (articulation of speech) even though the understand the task |
|
|
Non-fluent aphasia
|
Lesion varies based on type - typically frontal lobe of dominant hemisphere
Poor word output and dysprosodic speech (impaired rhythm and inflection). Poor articulation and increased effort of speech. Content is present, but impaired syntax Examples - Broca's Aphasia, Global Aphasia, Verbal Apraxia, Dysarthria Writing is also impaired. |
|
|
Hemiparesis vs Hemiplegia
|
Paresis - weakness
Plegia - paralysis |
|
|
Homonymous hemianopsia
|
loss of right or left half of field of vision in both eyes
|
|
|
Ideational apraxia
|
a condition in which an individual is unable to plan movement related to an object because he has lost the perception of the object's purpose.
loss of ability to conceptualize, plan, and execute the complex sequence of motor actions involving the use of tools or object |
|
|
Ideomotor apraxia
|
a person plans a movement or task, but cannot volitionally perform it. Automatic movement may occur, however a person cannot impose additional movement on command
|
|
|
Neologism
|
Substitution within a word that is so severe that it makes the word unrecognizable.
|
|
|
Perseveration
|
repeatedly performing the same segment of a task or repeatedly saying the same word/phrase without purpose
|
|
|
Left sided neglect
|
most common neglect. Seen with lesion to right inferior parietal or superior temporal lobes
|
|
|
Frontal Lobe - Function
|
- Voluntary movement - primary motor cortex, precentral gyrus
- Intellect - Orientation / concentration - Broca's area - L hemisphere - speech - Personality - temper, judgement, reasoning, behavior, self-awareness, executive functions |
|
|
Frontal Lobe - Impairment
|
- Contralateral weakness
- Perseveration - Inattention - Personality changes, antisocial behavior - Impaired concentration, apathy - Broca's aphasia (expressive deficits) - Delayed or poor initiation - Emotional lability |
|
|
Parietal Lobe - Function
|
-Sensation - touch, kinesthesia, vibration, temperature
- Provides meaning for objects - Interprets language and words - Spatial and visual perception |
|
|
Parietal Lobe - Impairment
|
- Dominant hemisphere (typically L) - Agraphia, Alexia, Agnosia
- Non-dominant hemisphere (typically R) - Dressing apraxia, construcitonal apraxia, anosognosia - Contralateral sensory deficits - Impaired language comprehension - Impaired taste |
|
|
Temporal Lobe - Function
|
- Auditory processing and olfaction
- Wernicke's area - understand and produce meaningful speech - Memory, understanding language - Interpretation of other's emotions and reactions |
|
|
Temporal Lobe - Impairment
|
- Learning deficits
- Wernicke's aphasia - Antisocial, aggressive behaviors - Difficulty with facial recognition - Difficulty with memory, memory loss - Inability to categorize objects |
|
|
Occipital Lobe - Function
|
- Processing center for visual information - colors, lights, shapes, 3D
|
|
|
Occipital Lobe - Impairment
|
- Homonymous hemianopsia
- Impaired extraocular muscle movement and visual deficits - Impaired color recognition - Reading and writing impairment - Cortical blindness with bilateral lobe involvement (Damage to posterior cerebral artery) |
|
|
Hippocampus
|
- Forms and stores new memories (declarative)
- Critical for learning language TEMPORAL LOBE |
|
|
Amygdala
|
- Emotional and social processing
- Involved with fear and pleasure responses, arousal, processing of emotional memories TEMPORAL LOBE |
|
|
Thalamus
|
- Processing/relay center
|
|
|
Hypothalamus
|
- Receives and integrates ANS information
- Regulates hormones - Controls hunger, thirst, sexual behavior, and sleep - Regulates body temperature and adrenal/pituitary glands |
|
|
Subthalamus
|
(Subthalamic nucleus)
- Associates with basal ganglia and substantia nigra to regulate movements produced by skeletal muscles |
|
|
Epithalamus
|
Primarily the pineal gland
- Secretes melatonin and is involved in circadian rhythms - Some regulation of motor pathways and emotions (associated with limbic system and basal ganglia) |
|
|
Midbrain
|
Relay area for information passing from the cerebrum, cerebellum, and spinal cord
- Also a reflex center for visual, auditory, and tactile responses |
|
|
Cerebellum
|
- Responsible for fine-tuning movement
- Postuion re and balance - Rapid alternating movements - Damage to one side causes ipsilateral deficts - ataxia, nystagms, tremor, hypermetria, poor coordination, balance |
|
|
Pons
|
Assits w regulating respiration rate and orientaiton of head in relation to visual and auditory stimuli
|
|
|
Medulla oblongata
|
ANS activity
HR RR Has reflex centers for vomiting, coughing, sneezing Relays somatic sensory information from internal organs Controls sleep and arousal |
|
|
Brainstem
|
Includes midbrain, pons, and medulla.
Relay station HR RR |
|
|
CN I
|
Olfactory
Sensory - Smell Test - Identify familiar odors |
|
|
CN II
|
Optic
Sensory - Sight Test - Test visual fields |
|
|
CN III
|
Oculomotor
Motor - Raise eyelid; superior, medial, and inferior recti; inferior oblique muscle of eyeball - Autonomic - Smooth muscle of eyeball Test - Upward, downward, medial gaze; reaction to light |
|
|
CN IV
|
Trochlear
Motor - Superior oblique muscle Test - Downward & Lateral gaze |
|
|
CN V
|
Trigeminal
Sensory - Touch & pain of skin of face, mucous membranes of nose, sinuses, mouth, anterior tongue Motor - Muscles of mastication Test - Corneal reflex, face sensation, clench teeth, push down on chin to separate jaws |
|
|
CN VI
|
Abducens
Motor - lateral rectus muscle Test - lateral gaze |
|
|
CN VII
|
Facial
Taste - anterior tongue Motor - facial muscles Autonomic - lacrimal, submandibular, and sublingual glands Test - close eyes tight, smile and show teeth, whistle and puff cheeks, identify familiar tastes (sweet, sour) |
|
|
CN VIII
|
Vestibulocochlear (acoustic nerve)
Sensory - Hearing, balance Test - watch ticking, hearing tests; balance and coordination tests |
|
|
CN IX
|
Glossopharyngeal
Sensory - Touch, pain - posterior tongue, pharynx; taste - posterior tongue Motor - some muscles of pharynx; autonomic - parotid gland Test- Gag reflex; ability to swallow |
|
|
CN X
|
Vagus
Sensation - touch, pain - pharynx, larynx, bronchi. Taste - tongue, epiglottis Motor - muscles of palate, pharynx, larynx; autonomic - thoracic and abdominal viscera Test - gag reflex, ability to swallow, say "ahh" |
|
|
CN XI
|
Spinal accessory
Motor - SCM and upper trap Test - resisted shoulder shrug |
|
|
CN XII
|
Hypoglossal
Motor - tongue protrusion |
|
|
Dorsal scapular nerve
|
C5
Rhomboids Levator scapulae |
|
|
Long thoracic nerve
|
C5, 6, 7
Serratus anterior |
|
|
Nerve to subclavius
|
C5, 6 - Superior trunk
Subclavius muscle depresses and protracts scapula; protects brachial plexus and clavicle |
|
|
Suprascapular nerve
|
C5, 6 - Superior trunk
Infraspinatus Supraspinatus |
|
|
Lateral cord of brachial plexus
|
Lateral pectoral
Musculocutaneous Lateral root of median |
|
|
Medial cord of brachial plexus
|
Medial pectoral
Ulnar Medial root of median |
|
|
Posterior cord of brachial plexus
|
Upper subscapular
Thoracodorsal Lower subscapular Axillary Radial |
|
|
Lateral pectoral nerve
|
From lateral cord of plexus
Innervates clavicular head of pec major |
|
|
Musculocutaneous nerve
|
From lateral cord of plexus
Biceps Brachialis Coracobrachialis |
|
|
Median nerve
|
From lateral and medial cords of plexus
Innervates muscles in forearm, except FCU, and five muscles of the hand (thenar muscles plus 1st and 2nd lumbricals) |
|
|
Medial pectoral nerve
|
From medial cord of plexus
Pec major - sternal portion Pec minor |
|
|
Ulnar neve
|
Medial cord
FCU Flexor digitorum profundus Most hand intrinsics |
|
|
Upper subscapular nerve
|
Posterior cord
Subscap |
|
|
Thoracodorsal nerve
|
Posterior cord
Lats |
|
|
Lower subscapular nerve
|
Posterior cord
Subscap; teres major |
|
|
Axillary nerve
|
Posterior cord
Deltoid; teres minor |
|
|
Radial nerve
|
Posterior cord
Triceps Aconeus Supinator Wrist extensors Brachioradialis |
|
|
Femoral nerve
|
Anterior compartment of thigh - L2-L4 - knee extension
Quadriceps Iliacus Sartorius Pectineus |
|
|
Obturator nerve
|
Medial compartment of thigh - Hip adductors
Adductor longus Adductor brevis Adductor magnus Obturator externus Gracilis |
|
|
Inferior gluteal nerve
|
Glute max
|
|
|
Superior gluteal nerve
|
Hip abductors
Glute min, med TFL |
|
|
LE Innervation from sacral plexus
|
Hip ER muscles
Piriformis Superior gemellus Obturator internus Inferior gemellus Quadratus femoris |
|
|
Sciatic nerve
|
Exits inferior to piriformis in greater sciatic foramen
Tibial division - Semitendinosus, semimembranosus, biceps femoris ( long head ) Common peroneal division - short head o biceps Divides into common peroneal and tibial n for lower leg innervation |
|
|
LE Innervation from lumbar plexus
|
Psoas major and minor
Quadratus lumborum |
|
|
Deep peroneal nerve
|
Innervates lower leg anterior compartment
Tibialis anterior Extensor digitorum longus Extensor Hallucis longus Peroneus tertius Extensor digitorum brevis |
|
|
Superficial peroneal nerve
|
Innervates lateral compartment of lower leg
Peroneus longus Peroneus brevis |
|
|
Medial plantar nerve
|
Abductor hallucis
Lumbrical I Flexor digitorum brevis Flexor hallucis brevis |
|
|
Lateral plantar nerve
|
Abductor digiti minimi
Flexor digiti minimi Opponens digiti minimi Dorsal interossei Quadratus plantae Adductor hallucis Lumbrical II, III, IV Plantar interossei |
|
|
Tibial nerve
|
Posterior compartment of lower leg
Gastroc Plantaris Soleus Popliteus FDL FHL Posterior tib |
|
|
Abdominal reflex
|
T8-L1
Stroke from each quadrant of abdomen toward umbilicus Normal - contraction of abdominals and deviation of umbilicus toward stimulus |
|
|
Corneal reflex
|
trigeminal and facial nerves
"blink" reflex Have patient look up and away from you; Stroke the cornea with cotton BOTH eyes blink |
|
|
Gag reflex
|
glossopharyngeal and vagus nerves
|
|
|
Plantar reflex
|
L5-S1
Stroke foot - toes flex Babinski reflex - abnormal; CNS lesion |
|
|
Akinesia
|
inability to initiate movement; commonly seen in Parkinson's disease
|
|
|
Asthenia
|
generalized weakness, typically secondary to cerebellar pathology
|
|
|
Athetosis
|
involuntary movments combined with instability of posture. Peripheral movements occur without central stability
|
|
|
Clasp-knife response
|
Greater resistance at beginning of ROM of a hypertonic joint
|
|
|
Cogwheel rigidity
|
resistance to movement has a phasic quality to it; often seen with Parkinson's disease
|
|
|
Dysdiadochokinesia
|
inability to perform rapidly alternating movements
|
|
|
Dysmetria
|
inability to control range of a movement and force of muscular activity
|
|
|
Fasciculation
|
A muscular twitch caused by random discharge of a lower motor neuron and its muscle fibers; suggests a lower motor neuron disease
Can be benign |
|
|
Hemiballism
|
involuntary and violent movement of a large body part
|
|
|
Lead pipe rigidity
|
uniform and constant resistance to ROM; often associated with lesion to basal ganglia
|
|
|
Brown-Sequard
|
Typically traumatic (Stab)
Spinal cord hemisection IL paralysis and loss of vibratory/position (corticospinal tract and dorsal column) CL loss of pain and temp (lateral spinothalamic tract) |
|
|
Lateral spinothalamic tract
|
Pain & temp
CL loss |
|
|
Anterior spinothalamic tract
|
Crude Touch
CL loss |
|
|
Dorsal column
|
Deep touch, 2 point discrimination, vibration, joint position
IL Loss |
|
|
Anterior cord syndrome
|
Caused by damage to anterior cord or anterior spinal artery, usually cervical flexion
Loss of motor function and pain/temp sense below lesion due to ventral corticospinal and spinothalamic tracts |
|
|
Central cord syndrome
|
MOI usually cervical hyperextension
Damages spinothalamic tract, corticospinal tract, and dorsal colums UE>LE deficits Motor > sensory deficits |
|
|
Posterior cord syndrome
|
MOI - compression of posterior spinal artery
Loss of pain perception, proprioception, two-point discrimination, and stereognosis. Motor preserved |
|
|
ASIA Impairment Scale
|
A = complete - no sensory or motor function preserved in sacral segments S4-S5
B = sensory incomplete - sensory but not motor function preserved below level to S4-S5 C = Motor incomplete - motor preserved below, key muscles below have less than 3/5 D = Motor incomplete - motor preserved below, key muscles greater than or = 3/5 E = normal |
|
|
Neurapraxia
|
Mildest
All structures in tact Recovery 4-6 weeks Most common - pressure injury |
|
|
Axonotmesis
|
Level II Injury
Reversible damage to axons - regen. 1mm per day Sheath and supporting structures in tact Wallerian degeneration may occur Spontaneous recovery - spotty to no recovery May require surgery Traction compression, crush injuries |
|
|
Neurotmesis
|
Most severe nerve injury
All structures damaged; nerve transection Irreversable Total loss of sensation and flaccid paralysis Surgery may help - sensory returns before motor |
|
|
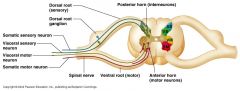
Anterior horn cell pathology
|
- sensory component in tact
- motor weakness and atrophy - fasciculations - decreased DTR Example: ALS, polio |
|
|
Muscle pathology
|
- sensory component in tact
- motor weakness; fasciculations are rate - normal or decreased DTR Example: muscular dystrophy |
|
|
Neuromuscular junction pathology
|
- sensory component in tact
- motor fatigue is greater than actual weakness - normal DTR Example: myasthenia gravis |
|
|
Peripheral nerve pathology (mononeuropathy)
|
- sensory loss along nerve route
- motor weakness and atrophy in a peripheral distribution; may have fasciculations Example: trauma |
|
|
Peripheral polyneuropathy
|
- sensory impairments; "stocking glove" distribution
- motor weakness and atrophy; weaker distally than proximally; may have fasciculations - decreased DTRs Example: diabetic peripheral polyneuropathy; GBS |
|
|
Spinal nerve root pathology
|
- dermatomal deficits
- motor weakness in an innervated pattern - may have fasciculations - decreased DTR Example: disc herniation |
|
|
Modified Ashworth Scale
|
For spasticity
0 - no increased muscle tone 1 - slight increase; "Catch" and release or minimal resistance at end-range 1+ - slight increased throughout whole ROM 2 - affected parts movable but with marked increase in tone 3 - passive movement difficult 4 - rigid |
|
|
Antiepileptic Agents
|
Side effects - ataxia, skin issues, behavioral changes, GI, headache, blurred vision, weight gain
- Clonazepam, valproic acid, gabapentin (neurontin) |
|
|
Antispasticity Agents
|
Promote relaxation by binding to CNS or directly to muscle cells
Side effects - drowsiness, confusion, headache, dizziness, generalized weakness, tolerance/dependence Implications - sedation; loss of function due to decreased tone - baclofen, valium (diazepam), dantrolene |
|
|
Cholinergic Agents
|
Mimic acetylcholine and bind directly to cholinergic receptor
Indications - glaucoma, dementia (alzheimer's), post-op decreased GI motility, myasthenia gravis Side effects - GI, impaired visual accomodation, bronchoconstriction, bradycardia, flushing, parasympathic effects Implications - Decreased HR/dizziness |
|
|
Dopamine Replacement Agents
|
Parkinson's
Side effects - arrhythmias (levodopa), GI, orthostatic hypotension, dyskinesias, mood and behavioral changes, tolerance Implications - Schedule therapy 1 hr after levadopa. Monitor BP for hypotension - levodopa, amantadine |
|
|
Muscle Relaxing Agents
|
For muscle spasm
Side effects - sedation, drowsiness, dizziness, nausea, vomiting, headache, tolerance, dependence - diazepam, flexeril, paraflex |
|
|
Brunnstrom Stages of Recovery
|
1 - No movement
2 - Appearance of synergies, Beginning of spasticity. 3 - Synergies are performed voluntarily; spasticity increases 4 - Spasticity begins; movement patterns not dictated solely by synergies 5 - Further dec in spasticity; independence from synergy patterns 6 - Isolated joint movements performed with coordination 7 - Normal |
|
|
UE Flexor Synergy Pattern
|
Scapular elevation and retraction
Shoulder abduction and ER Elbow flexion Forearm supination Wrist flexion Finger flexion with adduction Thumb flexion with adduction |
|
|
UE Extensor Synergy Pattern
|
Scapular depression and protraction
Shoulder IR and adduction Elbow extension Forearm pronation Wrist extension Finger flexion and adduction Thumb flexion and adduction |
|
|
LE Flexor Synergy Pattern
|
Hip abduction and ER
Knee flexion Ankle DF / supination Toe extension |
|
|
LE Extensor Synergy Pattern
|
Hip extension, IR, and adduction
Knee extension Ankle PF / inversion Toe flexion and adduction |
|
|
Concussion grades
|
1 - no LOC, some confusion. Symptoms resolve in 15'. Athlete should return after 1 week of rest
2 - Confusion lasting longer than 15'. Poor concentration, retrograde amnesia. CT scan indicated if symptoms worsen. Return to play deferred until 2 weeks of rest and no symptoms on exertion. 3 - Any LOC. Emergency transport required for full neurological evaluation. Hospitalization may be warranted. Rest for 1 symptom free month. May result in coma. |
|
|
Ranchos Los Amigos Levels of Cognitive Functioning
|
I. No Response
II. Generalized Response - non-purposeful responses III. Localized Response - specific but inconsistent responses. May follow simple commands such as squeeze hand, open eyes. IV. Confused-Agitated - Heighted state of activity; bizarre and non-purposeful behavior. Limited attention V. Confused-Inappropriate - able to respond to simple commands; verbalization inappropriate and confabulatory VI. Confused-Appropriate - goal directed behavior present but dependent on external input or direction. Responses may be incorrect from memory deficit but are appropriate to the situation VII. Automatic-Appropriate - Goes through daily routine but often robot-like VIII. Purposeful-Appropriate - :) |
|
|
Anterograde amnesia
|
inability to create new memory. Usually last to recovery after comatose state
|
|
|
Post-traumatic amnesia
|
time between injury and when the patient is able to recall recent events. Patient does not recall the injury of events up until this point of recovery. Post-traumatic amnesia is used as an indicator of the extent of damage.
|
|
|
Retrograde amnesia
|
Inability to remember events prior to injury.
|
|
|
Glascow Coma Scale
|
8 or less - severe injury
9-12 - moderate injury 13-15 - mild injury EYE OPENING (E) Spontaneous - 4 To speech - 3 To pain - 2 Nil - 1 BEST MOTOR RESPONSE (M) Obeys commands - 6 Localizes pain - 5 Withdraws - 4 Abnormal flexion - 3 Extensor response - 2 Nil - 1 VERBAL RESPONSE (V) Oriented - 5 Confused conversation - 4 Inappropriate words - 3 Incomprehensible words - 2 Nil - 1 |
|
|
Alzheimer's Disease
|
Progressive deterioration to cerebral cortex
Acetylcholine transmission decreased Neurofibrillary tangles and amyloid plaques Medication given to inhibit acetylcholinesterase |
|
|
ALS
|
Chronic degenerative disease with UMN and LMN impairments
Weakness and muscle atrophy from anterior horn and cranial nerve cells (distal to proximal) Typical onset - 40-70 years of age |
|
|
Bell's palsy
|
Temporary Facial nerve paralysis
Commonly 15-45 years |
|
|
GBS
|
Guillain-Barre Syndrome
Temporary acute polyneuropathy Inflammation and demyelnation of peripheral nerves Autoimmune? Motor weakness distal to proximal, sensory impairment, respiratory paralysis. Often symmetrical Recovery - 3-12 months up to 1 year |
|
|
Multiple Sclerosis
|
Demyelination of brain and spinal cord
Symptoms vary based on location and extend of demyelination Highest incidence - 20-35 years 15 years from onset - 50% require wheelchair Most patients live for many years Suicide not uncommon |
|
|
Myasthenia Gravis
|
Autoimmune
Neuromuscular junction Symptoms range from mild to severe Extreme fatiguability and skeletal muscle weakness that can fluctuate within minutes or even an extended period. Ocular muscles are typically affected first Remissions and exacerbations Myasthenia gravis "crisis" - medical emergency involving respiratory muscles |
|
|
Parkinson's Disease
|
Degenerative disorder involving decreased DOPAMINE in corpus striatum and substantia nigra of basal ganglia
Parkinsonism - these symptoms as a secondary effect of another disease Initially - resting tremor Progresses to hypokinesia, difficulty starting and stopping movement (akinesia), festinating gait, cogwheel / lead pipe rigidity, "freezing", no facial expression Medical tx - dopamine replacement therapy (Levodopa, sinemet, madopar) |
|
|
Post-polio syndrome
|
Lower motor neuron pathology - anterior horn cell
Involves slow and progressive weakness, fatigue, muscle atrophy, pain and swallowing issues |
|
|
ATNR
|

Birth to 6 months
Head position - turned to one side -> Face side - extended Scalp side - flexed Spine curved toward face side |
|
|
STNR
|
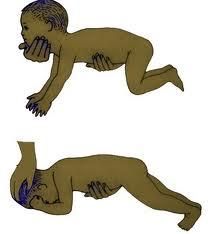
6-8 months
Head in flexion - arms flexed, legs extended Head in extension - arms extended, legs flexed |
|
|
Tonic Labyrinthine Reflex
|
Birth to 6 months
Based on position of labyrinth in inner ear (head position) In supine - body and extremities in extension In prone - body and extremities in flexion |
|
|
Galant reflex
|

2 months
Lateral flexion of trunk toward stimulus |
|
|
Palmar grasp
|
4 months
Pressure on ulnar side of hand - flexion of fingers Interferes with ability to voluntarily release objects |
|
|
Plantar grasp
|
3 months
Pressure on base of toes -> toe flexion Interferes with ability to stand with feet flat, balance, and wt shift |
|
|
Rooting reflex
|
9 months
Touch on cheek - turn head to same side with mouth open |
|
|
Moro reflex
|

5 months
Head drops into extension suddenly -> arms abduct, fingers open, then cross into adduction; cry |
|
|
Startle reflex
|
5 months
Loud, sudden noise -> similar to Moro response but elbows remain flexed and hands closed |
|
|
Positive support reflex
|

2 months
Weight placed on balls of feet when upright -> stiffening of leg and trunks into extension Interferes with standing, walking, balance reactions, and can lead to PF contracture |
|
|
Walking (stepping) reflex
|
2 months
Support upright with soles of feet on firm surface Reciprocal flexion/extension of legs Interferes with development of smooth, coordinated reciprocal gait |
|
|
Newborn to 1 month
|
Physiological flexion
Lifts head briefly Rolls partly to side from supine Reflex standing/walking Hands fisted Jerky arm movements Head lag on pull to sit |
|
|
2-3 months
|
Lifts head 90 degrees briefly
Chest up in prone with some weight through forearms ATNR influence is strong Legs kick Variable head lag in pull to sit Rolls prone to supine Needs full support to sit Grasp is reflexive |
|
|
4-5 months
|
Bears weight on extended forearms
Rolls from supine to SL Feet to mouth Sits alone for brief periods; head steady, turns head Grasps and releases toys |
|
|
6-7 months
|
Rolls from supine to prone
Lifts head in supine Sits up without assistance SIts independently Voluntary release of objects to transfer between hands May crawl backward |
|
|
8-9 months
|
Does not tolerate supine
Pulls to stand on furniture Crawls forward Cruises (walks along furniture) |
|
|
10-11 months
|
Stands without support briefly
Half-kneel Creeps on hands and feet (bear walk) Fine-pincer grasp developed |
|
|
12-15 months
|
Walks without support-fast, backward, sideways
Throws ball in sitting Creeps upstairs |
|
|
16-24 months
|
Walking upstairs - both feet on each step
Picks up toy from floor |
|
|
2 years
|
Rides tricycle
Walks backward and on tip-toe Runs on toes Descends stairs reciprically Catches ball |
|
|
3-4 years
|
Walks line, hops on one foot
Jumps Runs fast and avoids obstacles |
|
|
5-8 years
|
Skips
Hand preference is evident Prints well, beginning to write cursive Jump with rhythm (hopscotch) |
|
|
Arthrogryposis Multiplex Congenita
|
non-progressive
thought to occur during first trimester in utero involves fibrosis of muscles and structures within the joints leads to contractures, dislocation of joints, and muscle atrophy |
|
|
Cerebral Palsy
|

"umbrella term" used to describe movement disorders due to brain damage in utero, birth, or infancy
Non-progressive Can be caused by lack of oxygen, maternal infections, drug or alcohol abuse, prematurity, brain injury, etc Spastic - lesion in motor cortex of cerebrum; UMN Athetoid - lesion of basal ganglia; cerebellum/cerebellar pathways |
|
|
Down Syndrome
|

Trisomy 21 (genetic abnormality)
Risk increased with advanced maternal age Mental retardation, hypotonia, joint hypermobility, etc |
|
|
Duchenne Muscular Dystrophy
|
Progressive disorder caused by absence of a gene required to produce dystrophin and nebulin. Cell membranes weaken, myofibrils are destroyed, and contractility is lost.
Fat and connective tissue eventually replaces musle, and death occurs from cardiopulmonary failure prior to age 25, usually in the teenage years. X-linked recessive trait Child's mother is a silent carrier and only male offspring will manifest the disease Manifests between 2 and 5 years of age |
|
|
Prader-Willi Syndrome
|
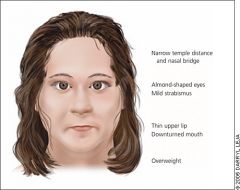
Genetic - partial deletion of chromosome 15
Small hands, feet, sex organs Hypotonia, almond-shaped eyes, obesity, constant desire for food. Coordination impairments, mental retardation |
|
|
Spina Bifida
|

Developmental abnormality due to insufficient closure of neural tube by 28th day of gestation.
Affects CNS, musculoskeletal, and urinary systems Spina Bifida Occulta - fusion of spinous process. Spinal cord and meninges remain in tact Spina Bifida Cystica - cyst-like protrusion - Meningocele - herniation of meninges and CSF into sac that protrudes through vertebral defect. Spinal cord remains in canal - Myelomeningocele - severe. Spinal cord extending through defect in vertebrae. May or may not be covered by skin PT involves family ed on positioning, handling, ROM/ther ex, skin care, adaptive equipment and orthotic/wheelchair prescription |
|
|
Spinal Muscular Atrophy
|
Progressive degeneration of anterior horn cells
Autosomal recessive Type 1 - occurs before month 2. rapid motor degeneration, life expectancy less than 1 year Type 2 - occurs 6 mon- 1 year with slower progression. Child can survive to adulthood Type 3 (Juvenile SMA) - Onset 4-17 years; typically survive into adulthood Progressive muscle atrophy, diminished or absent DTR, normal intelligence, in-tact sensation, end-stage respiratory compromise |