![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
187 Cards in this Set
- Front
- Back
|
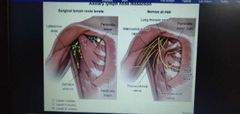
Axillary LN schema? |
|
|
|
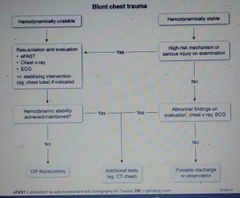
Algorithm of blunt chest trauma? |
|
|
|
Rx of CRC in pts with Mets confined to liver? |
Surg resection of both primary tumor & liver met. |
|
|
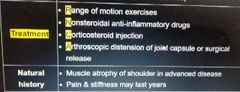
Rx of adhesive capsulitis? Natural hx? |
|
|
|
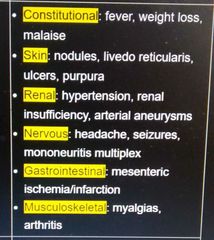
Px of PAN? |
|
|
|
Dx of PAN? |
|
|
|
Rx of abdominal compartment syn? |
|
|
|
Rx of an avulsed permanent tooth? |
1- until reimplantation=> tooth stored in cold milk, saliva or tooth culture media 2- tooth & socket gently rinsed with NS 3- Tooth handled by crown, placed in socket & splinted to adjacent teeth 4- discharged with ppx Abx eg doxy |
|
|
Rx of priapism? |
1- aspiration of corpora cavernosa 2- intracavernous injection of phenylephrine |
|
|
Management of traumatic brain injury? |
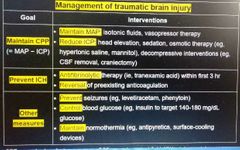
|
|
|
Components of breast conserving therapy? |
1- partial mastectomy aka lumpectomy with neg lateral margins (re excised until margins are negitive) 2- SNLN Bx => ALND if ≥3 nodes positive 3- radiation therapy to eradicate any remaining tumor |
|
|
Modified radical mastectomy? |
1- whole mastectomy 2- ALND |
|
|
Rx of snake bite? |

|
|
|
Cardiovascular CI to preg? |
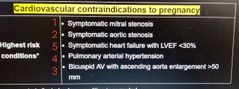
|
|
|
Criteria used for sepsis evaluation in ED? |
qSOFA score 1- RR >22/min 2- SBP ≤100 mmhg 3- confusion ≥2 shows septic |
|
|
Rx of sepsis in ED? |
1- blood culture 2- broad spectrum abx within 1 hr 3- aggressive fluid resuscitation within 3 hr 4- vasopressor NE => after >3L of IVF |
|
|
Empiric Abx used in sepsis? |
1- pip tazo/ meropenem/ cefepime PLUS 2- vanc |
|
|
1- Px of dialysis catheter associated bloodstream infections? 2- Rx? |
1- sepsis without any localizing signs 2- Abx=> vanc + ceftazidime IVF catheter removal |
|
|
Rfs for colon ca? |
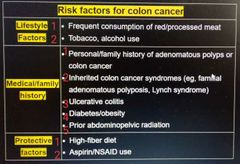
Frequently=daily |
|
|
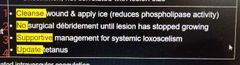
Rx of brown recluse spider? |
|
|
|
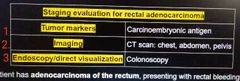
Staging evaluation of rectal adenocarcinoma? |
|
|
|
Rx of empyema? |
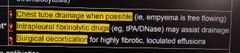
4- abx |
|
|
Rx of post hip dislocation? |
W/I 6 hrs to Dec risk of osteonecrosis of femoral head 1- dislocation without fx=> closed reduction 2- dislocation with fx=> open reduction |
|
|
CRC px if in 1- R colon 2- L colon 3- rectum |
1- occult bleeding + Fe def anemia 2- hematochezia + crampy/colicky abd pain+ change in bowel habits 3- hematochezia + narrow stools+ tenesmus+ sensation of mass in rectum |
|
|
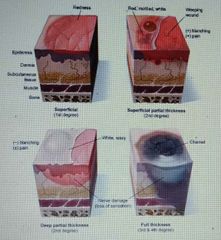
Degrees of burns? |
|
|
|
Rx of burns? |
1- superficial=> wound care (wash daily, apply moisturizer) 2- partial thickness=> gentle debridement with NS 3- full thickness => complete surg excision followed by skin grafting |
|
|
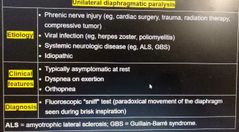
1- U/L diaphragmatic paralysis causes? 2- Px? 3- Dx? |
|
|
|
Clinical scenario for AVN of humeral head? |
Shoulder joint dislocation PLUS proximal humeral fx Px=> pain with abduction |
|
|
Axillary N injured during ant shoulder dislocation Px? |
deltoid & teres minor weakness => pain & weakness of abduction |
|
|
Diff between rotator Cuff injury & axillary N injury? |
Axillary N injury also causes sensory loss over lateral shoulder |
|
|
Fall on outstretched hand. Associated fxs? |

|
|
|
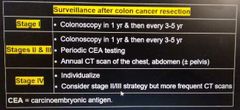
Surveillance after colon ca resection? |
|
|
|
Stages of colon cancer? |
1=> only involves mucosa & sub mucosa 2=> muscular & serosal layer 3=> LN involvement |
|
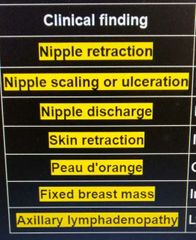
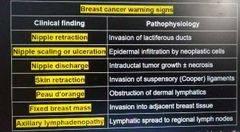
Breast cancer warning signs? |
|
|
|
Intraductal papilloma px? |
U/L bloody discharge + no mass |
|
|
Rx of lung abscess? |

|
|
|
Clinda not 1st line for lung abscess due to? |
Inc risk of c diff infection |
|
|
Bronchiolitis obliterans px? |
Lung transplant pt develops: 1- progressive dyspnea & non productive cough 2- obstructive pattern on PFTs |
|
|
Px of pyogenic liver abscess? |
1- fever + RUQ pain + hepatomegaly 2- Inc WBCs + Inc liver enzymes esp ALP & bili |
|
|
Dx of liver abscess? Rx? |
1- CT scan of abd, US 2- Blood culture, IV Abx, abscess drainage |
|
|
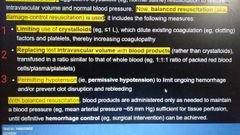
Components of balanced resuscitation/ damage control resuscitation? |
|
|
|
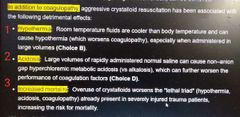
S/Es of aggressive crystalloid resuscitation? |
|
|
|
Main muscles responsible for 1- foot eversion 2- foot inversion |
1- peroneus muscles 2- tibialis ant & post muscles |
|
|
Can a pt with complete Achilles tendon rupture have normal plantar flexion? |
Yes due to plantaris, flexor hallucis longus & digitorum longus as they directly insert on foot (not via Achilles) |
|
|
Test used to id complete Achilles tendon rupture? |
Thompson aka calf squeeze test Squeeze calf=> no passive plantar flexion= complete Achilles tendon rupture |
|
|
Dx of tarsal tunnel syn? Rx? |
Positive Tinel test=> tapping in post medial malleolar area=> produces pain |
|
|
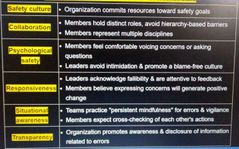
Features of effective teams in health care? |
|
|
|
1- Technique used by high reliability organizatios to improve Psychological safety ? 2- Other examples? |
1-Team safety debriefings 2-A) teamwork simulation with teams practicing communication skills B) Development of evaluation metrics rewarding members who id errors & safety risks |
|
|
Rx of burn associated infections? |
1- local wound infection ie no sepsis=> cefazolin, clindamycin 2- sepsis=> piptazo/ meropenem Plus vanc |
|
|
Li enhanced physiological tremors vs Li toxicity tremors? |
Enhanced=> symmetric, limited to hands & upper limbs Toxicity=> irregular coarse tremors involving multiple parts of body |
|
|
Pathophys of Li associated tremors? |
Fe accumulation in substantia nigra |
|
|
CT scan in eclampsia? |
White matter edema |
|
|
Electrolyte abnormality associated with amphetamine intoxication? |
Hyponatremia possibly serotonin induced |
|
|
Amphetamine intoxication can be confirmed by? |
Urine drug testing |
|
|
Rx of recurrent cystitis in females? |

|
|
|
Wu of presbycusis? |
1- careful hx of hearing changes 2- whispered voice test 3- for confirmation=> audiometric testing |
|
|
Gender Id? Gender expression? Gender variance? |
1- internal sense of being male, female 2- how a person expresses gender to outside world 3- when id/expression varies from social norms |
|
|
Gender dysphoria? |
Disagreement between gender id & assigned sex by birth |
|
|
1- Wt gain in preg on basis of pre preg BMI? 2- Associated calories in pts with normal wt? |
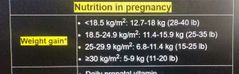
2nd trimester=> Inc calorie intake by 350 kcal/day 3 trimester=> Inc calorie intake by 450 kcal/day |
|
|
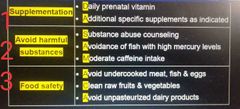
Supplementation in preg? Harmful substances? Food safety? |
|
|
|
Indications for C section during 1st stage of labour? |
1- arrest of labor 2- category 3 FHR tracing |
|
|
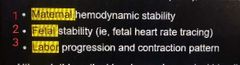
Pts with intrapartum bleeding evaluated with? |
|
|
|
Tocolytic use other than delaying delivery? |
Indicated for FHR abnormality caused by uterine tachysystole ie >5 contractions/Mon |
|
|
Causes of 2° PPH? |
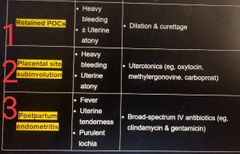
2° PPH=> >24 Hrs after delivery |
|
|
Retained placenta vs retained POC px? |
Retained placenta=> immediate PPH Retained POC=> late PPH |
|
|
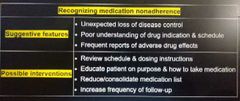
Recognizing med non-adherence? |
|
|
|
Typical feature of med discontinuation? |
dz worsening after years of good control |
|
|
Med discontinuation suspected. Nbsim? |
Non judgemental inquiry into use of med, focusing on when, how & how often do they use |
|
|
Insulinoma typical age of onset? |
> 40 |
|
|
Typical feature of concealed placental abruption? |
Severe focal pain at location of placenta=> progresses to diffuse uterine tenderness |
|
|
Pathophys of placental abruption? |
Maternal vasoconstrictors=> cross into placenta => placental vasocons & ischemia=> necrosis & hemorrhage at UP interface=> detachment of placenta=> Inc intrauterine pressure=> uterine irritability => high frequency contractions |
|
|
MS risk associated with preg? |
1- preg protective for MS 2- INC risk in post partum period |
|
|
Tb screening should be considered in? |
1- close contact with known Tb 2- travel from endemic area 3- exposed to high risk setting homeless shelter, prisons |
|
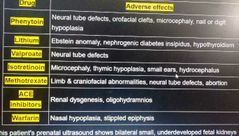
Teratogenicity of ? |
|
|
|
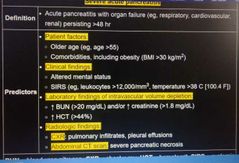
SIRS criteria? |

|
|
|
Severe acute panc definition? Predictors? |
|
|
|
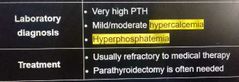
Labs in tertiary PTH? Rx? |
|
|
|
1- Acromioclavicular joint sprain pathophys? 2- P/E? 3- XRAY? |
1- direct trauma to superior or lateral shoulder 2- pain over AC joint & with addiction of arm across torso 3- can assess degree of sprain & concomitant clavicular or humeral fx |
|
|
Heme dzs associated with priapism? |
1- scd 2- Heme cancers eg CML 3- thalassemia 4- MM |
|
|
Sx of Inc abd pain/sepsis/ unstable vitals 7-10 days after acute panc. 1- Dx? 2- Wu? |
1- Infected panc necrosis 2- CT scan of abd=> gas within panc necrotic collection |
|
|
1- Alternative to 1:1:1 blood components transfusion in hemorrhagic shock? 2- adjunctive therapy? |
1- whole Blood 2-A tranexamic acid wi 3 hrs B Topical hemostatic agents=> kaolin impregnated sponge, fibrin sealant dressing |
|
|
Cryoprecipitate is considered when? |
Fibrinogen <100 |
|
|
1- Acute lung transplant rejection px? 2- WU? 3- Rx? |
1- wi 6 mon of transplant Progressive dyspnea+ cough w/ low grade fever+ CXR =perihilar opacities & interstitial edema 2- BAL & lung bx to rule out infection 3- high dose glucocorticoids |
|
|
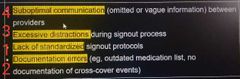
Root causes of errors related to transfers of care? |
|
|
|
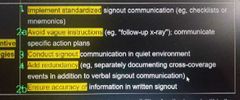
Preventive strategies for Root causes of errors related to transfers of care? |
|
|
|
Rx of auricular hematoma? Complications? |
|
|
|
Complications of glenohumeral joint (shoulder) dislocation? |
4- axillary N injury |
|
|
A- Rfs for associated injuries in shoulder dislocation? B- Nbsim? |
A 1- >40 2- first time dislocation 3- traumatic mechanism eg fall on outstretched hand B- x-ray to rule out fx |
|
|
Mc fxs associated with shoulder dislocation? |
1- Hill-sachs defect=> avulsion fx of posterolat humeral head 2- Bankart lesions=> glenoid labrum disruption |
|
|
Mc fxs associated with shoulder dislocation? |
1- Hill-sachs defect=> avulsion fx of posterolat humeral head 2- Bankart lesions=> glenoid labrum disruption |
|
|
Rx of shoulder dislocation? |
1- no fx/ Hill-sachs/ Bankart=> closed reduction 2- if associated humeral neck fx=> open surg repair to Dec risk of AVN |
|
|
Rx of shoulder dislocation? |
1- no fx/ Hill-sachs/ Bankart=> closed reduction 2- if associated humeral neck fx=> open surg repair to Dec risk of AVN |
|
|
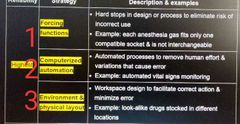
Human factors engineering strategies with highest reliability? |
|
|
|
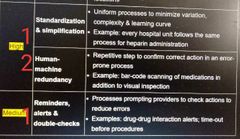
Human factors engineering strategies with high & medium reliability? |
|
|
|
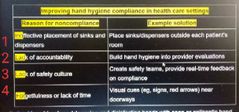
Reasons for hand hygiene non-compliance & their solutions? |
|
|
|
1- Optimal hand hygiene in hospital setting? 2- if expo to spores eg infect diarr, c diff/ soiled? 3- Can Dec hosp acquired infections upto? |
1- cleansing & disinfecting hands with soap or antiseptic hand rub (preferred) until dry (~20 sec) 2- washed thoroughly with soap & water ~20 sec 3- up to 70% |
|

>2500 m ascent wi days. 1- Dx? 2- Other features/ how to diff it from PNA? |
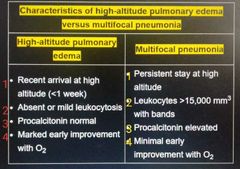
1- high altitude pul edema 2- |
|
|
Pathophys of high altitude pul edema? |
1- Normally=>Hypoxia at Inc altitudes=> vasoconstriction 2- In HAPE=> genetic predisposition unevenly distributed hypoxic vasocon=> expo of less vasocons pul capillaries to high perfusion pressure=> disruption of alveolar -capillary interface=> b/l pul edema |
|
|
CKD associated Tb risk? Associated finding related to PPD? |
1- 6 to 50 fold Inc in reactivation 2- PPD is FN due to immunocompromise |
|
|
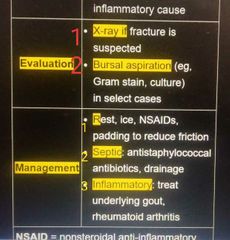
Rx of olecranon bursitis? |
|
|
|
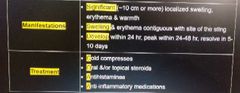
Px of local large reactions? Rx? |
|
|
|
Type of rxns in response to a sting? |
1- wheal & flare rxns 2- large local rxns 3- systemic rxns (anaphylaxis like) |
|
|
1- Mononeuritis multiplex? 2- Mcly triggered by? |
1- neuropathy of ≥2 non-contiguous peripheral nerves 2- underlying vasculitis esp PAN |
|
|
Antibody associated with PAN? Wu? |
1- not typically associated 2- tissue bx |
|
|
Triggers of GBS? |
1- GIT infection 2- URTI 3- Acute HIV infection |
|
|
1- Px of hereditary hemochromatosis associated arthropathy? 2- x-ray? 3- Rx? |
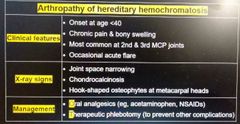
|
|
|
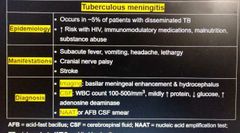
1- epidemic of Tb meningitis 2- px? 3- dx? |
|
|
|
Tb meningitis px over, |
Weeks |
|
|
1- CAP px in immunosuppred? 2- finding on CXR 3- Alternative? |
1- septic + sx localizing infection to lungs eg hypoxia+ crackles 2- normal 3- HRCT=> can id subtle pul infiltrates |
|
|
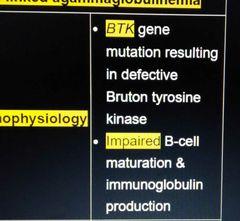
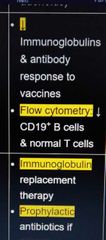
Pathophys of X linked agammaglobulinemia? |
|
|
|
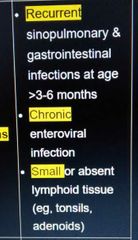
Px of X linked agammaglobulinemia? |
|
|
|
1- Labs of X linked agammaglobulinemia? 2- Rx? |
|
|
|
H influenzae type b infection in a fully immunized child. Dx? |
X linked agammaglobulinemia |
|
|
Acute distal symmetric polyneuropathy raises concern for? |
1- toxins 2- medication SEs |
|
|
Meds associated with distal symmetric polyneuropathy? |
1- MTZ 2- FQs 3- dapsone 4- amiodarone 5- digoxin |
|
|
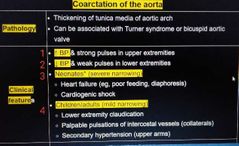
1- Pathophys of coarctation of aorta? 2- Px? |
|
|
|
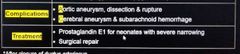
1- Complications of coarctation of aorta? 2- Rx? |
|
|
|
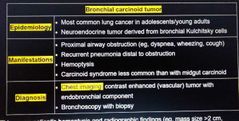
1- Bronchial carcinoid epidemiology? 2- px? 3- dx? |
|
|
|
Mc lung CA in young non-smokers? |
Bronchial carcinoid tumors |
|
|
1- Patient with which risk factor need to be started on earlier screening for CRC? 2- Screening method? |
A 1- abd-pelvic radiation 2- UC 3- Hereditary ca syn=> FAP, Lynch 4- Personal/ fhx of adenomatous polyps, colon ca B - at earlier age 30-40 Colonoscopy is preferred. Alt FOBT, fecal DNA testing |
|
|
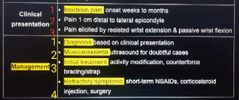
1- Px of lateral epicondylitis? 2- dx? 3- Rx? |
|
|
|
Main muscles affected in lateral epicondylitis? |
Conjoined tendons of extensor carpi radialis brevis & extensor digitorum at lateral epicondyle of humerus=> max pain 1cm distal to lateral epicondyle |
|
|
Causes of neonatal sepsis? Px? Dx? Rx? |
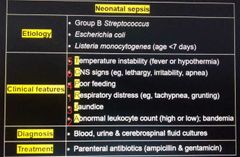
Acyclovir often added to cover HSV RAJPT C |
|
|
Neonates with sepsis are often brought in for? |
LIP 1- lethargy 2- irritability 3- poor feeding |
|

Finding? Dx? |
1- epidural fluid collection with rim enhancement 2- epidural abscess |
|
|
Management of colles fx? |
1- check neurovascular compromise 2- if compromised (Dec radial pulse/ Dec median N sensation) => immediate close reduction 3- if compromise improves=> wrist splinting with Ortho consult If doesn't improve=> emergent orthopedic consultation |
|
|
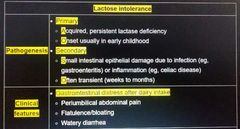
Lactose intolerance pathogen? Px? |
|
|
|
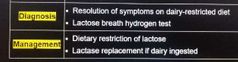
Dx of lactose intolerance? Rx? |
|
|
|
Strategies to improve health care communication? |
SCITT 1- standardized handoff 2- closed loop communication 3- interdisciplinary rounds 4- team Huddles & debriefings 5- team based training |
|
|
Standardized hand off description? Benefits? |
|
|
|
Closed loop communication description?Benefits? |
|
|
|
Interdisciplinary rounds description?Benefits? |
|
|
|
Team Huddles & debriefings description?Benefits? |
|
|
|
Team based training description?Benefits? |
|
|
|
1- Primary goal in management of drowning? 2- methods? |
1- correction of hypoxia 2- supplemental O² 3- not responding to O2 & can protect airway=> NPPV eg CPAP 4- not responding to O2 & can't protect airway (somnolent)=> endotracheal intubation with mechanical ventilation 5- bronchodilators to Rx bronchospasm |
|
|
Characteristics of physiological thelarche? |
1- normal in girls ≥8 2- often tender,breast buds posterior to nipple 3- can U/L in early puberty |
|
|
Rx of molluscum contagiosum 1- in children 2- in adults |
1- reassurance 2- |
|
|
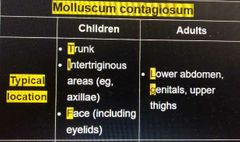
Typical location of Molluscum contagiosum lesions. 1- children 2- adults? |
|
|
|
Genital molluscum contagiosum in children is due to? |
Auto inoculation |
|
|
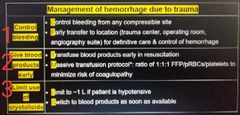
Management of hemorrhage due to trauma? |
|
|
|
Massive transfusion protocol? |
Massive transfusion is Required if ≥2 are positive & they should be given in 1:1:1 =FFP:pRBCs: Platelets 1- SBP ≤90 2- Pulse ≥120 3- positive FAST 4- penetrating mechanism of injury |
|
|
Time needed for type & cross-matching blood? |
>20 min |
|
|
Type of blood group that is given in hemorrhagic shock without type & cross matching? |
1- females of reproductive age=> Gp O, Rh D neg (to dec risk of HDN) 2- In females beyond reproductive age & Males=> either can be used Gp O, Rh D neg, Gp O, Rh D posi |
|
|
Chronic enteroviral meningitis+ recurrent PNA by encapsulated organisms+ Recurrent diarrheal illness. Dx? |
Bruton agammaglobulinemia |
|
|
Weber syn? |
Occlusion of PCA => Midbrain infarction=> ch by CN 3 dysfunction |
|
|
Drowning/ cardiac arrest=> Cushing reflex. Mechanism? |
Drowning/ cardiac arrest=> Hypoxic-ischemic brain injury=> neuronal cell death wi minutes=> widespread necrosis=> cerebral edema=> Inc ICP & compresses small arterioles=> Dec blood flow |
|
|
1- Cushing reflex prognostic sign? 2- it shows? |
1- poor prognostic sign 2- cerebral herniation is imminent |
|
|
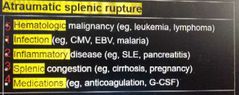
Rfs for atraumatic spleen rupture? |
|
|
|
1- Alarm sx of IBS? 2- NBSIM? |
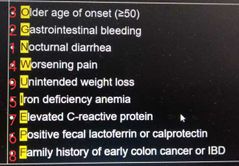
1- NGO WIPE FU 2- colonoscopy |
|
|
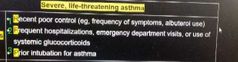
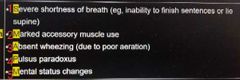
Rfs for severe life threatening asthma? |
|
|
|
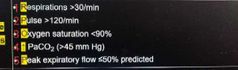
Objective measures in severe life threatening asthma? |
|
|
|
Exam findings in severe life threatening asthma? |
|
|
|
1- Pathophys of congenital dacryostenosis? 2- px? |
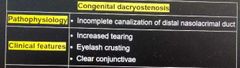
|
|
|
1- Rx of congenital dacryostenosis? 2- complications? |
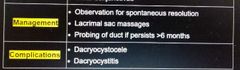
|
|
|
VACTERL screening? CHARGE? |
For both 1- Echo 2- Renal US Above plus these For VACTERL 3- contrast enema for anal atresia 4- limb radiographs |
|
|
Microcephaly definition? |
1- >2 SD below mean 2- <2 percentile for age |
|
|
Benign familial microcephaly? |
Genetically small head circumference that typically occurs in an infant who has normal height & weight & has a parent with a similarly small head |
|
|
1- Features suggestive of benign microcephaly ? 2- NBSIM? |
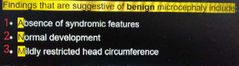
2- measure parental head circumferences |
|
|
Microcephaly+ early closure of fontanelle. Dx? |
Underlying genetic disorder |
|
|
1- Hypertrophic CM in infants of diabetic mothers pathogen? 2- px? 3- imaging? 4- Rx? 5- prognosis? |
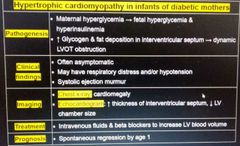
|
|
|
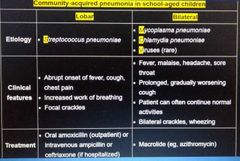
1- Causes 2- px 3- Rx of community acquired PNA in school age children 1- if lobar 2- if B/L |
|
|
|
Typical age of onset of CVID? |
1- adolescence (around puberty) 2- early adulthood 20-40 |
|
|
Clinical features suggesting Dec likelihood of MI despite Inc troponins? |
1- mild troponins elevation in context of CKD => Dec clearance of troponins 2- hx of chronically Inc troponins in prev hospitalizations 3- absence of clinical signs or findings suggestive of myocard ischemia eg ECG changes, new murmur |
|
|
1- Rfs for hypoglycemia in insulin therapy? 2- px? |
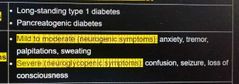
Pts with dec glucagon response eg in pancreatogenic diabetes => rapid, severe hypoglycemia with little warning |
|
|
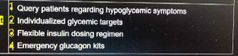
Rx of hypoglycemia in insulin therapy? |
|
|
|
Metabolic abnormalities associated with hypovolemic shock? |
1- hypernatremia/ hyponatremia 2- hyperkalemia 3- metabolic acidosis |
|
|
Progressive ECG changes in hyperkalemia? |
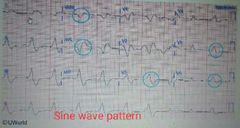
Peaked T waves=> loss of P waves=> widened QRS=> sine wave pattern => asystole |
|
|
NSAIDs effect on CHF? |
Often exacerbates it due to Na retention |
|
|
CXR infiltrate of PNA due to Bacteria/virus VS that of CHF? |
1- CXR infil of PNA=> Takes several wks to months to resolve despite clinical improvement after Abx 2- CXR infil of CHF resolves rapidly after diuretic therapy |
|
|
RTA typical px? |
1- Non-anion gap metabolic acidosis 2- FTT |
|
|
Typical associations of RTA? |
Type 1=> often a genetic DO & commonly associated with nephrolithiasis Type 2=> commonly component of fanconi Type 4=> obstructive uropathy & Aldo Insufficiency are common in children |
|
|
Pathophys of variable deceleration? |
UC Compression & Occlusion of umbilical vessels=> Inc in fetal SVR & BP => reflexive rapid Dec in FHR ie variable deceleration |
|
|
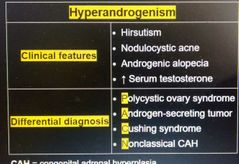
1- Cf s of hyerandrogenism? 2- DD? |
|
|
|
Dx criteria of PCOS? |
2 of following 3 : 1- clinical or lab evidence of hyerandrogenism 2- menstrual irregularities 3- PCOS on US |
|
|
Normal fetal activity in 3rd trimester? Ie >28 wks |
≥10 movements in 2 hrs |
|
|
Proteinuria definitions considered in preeclampsia? |
1- ≥300 mg/24 hr OR 2- protein/Cr ratio ≥0.3 OR 3- dipstick ≥1+ |
|
|
Communication failure between physicians during pt handoff results in? |
1- Medical errors 2- adverse pt outcomes |
|
|
Rx of medical errors due communication failure between physicians during handoff? |
Implementing a sign out checklist |
|
|
Essential components of an effective sign out checklist? |
1- DNR/ don't intubate status 2- hospital course & recent events 3- current condition & anticipatory info |
|
|
Tobacco smoking Dec risk of which gyne ca? |
Endometrial ca |
|
|
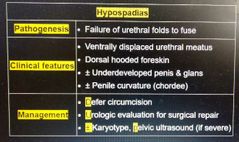
1- Hypospadias px? 2- Rx? |
|
|
|
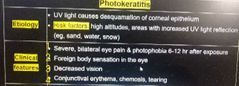
1- Photokeratitis rfs? 2- px? |
|
|
|
1- Dx of Photokeratitis? 2- Rx? 3- prevention? |
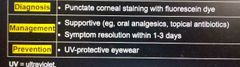
|
|
|
Eye conditions associated with damage caused by UV light ? |
1- Photokeratitis 2- pterygium 3- cataracts |
|
|
Hyphema? |
After trauma 1- pain 2- vision loss 3- blood in anterior chamber |
|
|
Ischemic colitis is a common complication of ? |
Vascular surgery eg aortic aneurysm repair |
|
|
Px of microscopic colitis? Triggers Dx? Rx? |
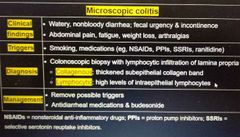
|