Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
400 Cards in this Set
- Front
- Back
- 3rd side (hint)
|
What are the 3 types of nervous systems disorders?
|
neurological
psychological psychiatric |
|
|
|
What is the major input-output structure for the limbs and trunk?
|
spinal cord
|
|
|
|
What is in the gray matter of the spina cord?
|
neuronal cell bodies, dendrites, and synapses
|
|
|
|
Sensory regions occupy the ___ horn?
|
dorsal
|
|
|
|
Motor regions occupy the ___ horn?
|
ventral
|
|
|
|
What is in the white matter?
|
numerous tracts that carry ascending sensory info and descending motor signals
|
|
|
|
Motor neurons cell bodies lie in the ____ and they send axons through the ___?
|
Ventral horn
ventral roots |
|
|
|
Sensory neurons cell bodies lie in the ____ and their axons ___?
|
dorsal root ganglia
branch- one branch enters the spinal cord, another branch goes to the periphery via the dorsal root, spinal nerve, and peripheral nerve |
|
|
|
What are the principal constituents of the brain?
|
cerebrum
cerebellum brainstem |
|
|
|
The forebrain subdivides into what structures?
|
telencephalon
diencephalon |
|
|
|
The hindbrain subdivides into what structures?
|
metacephalon
myelencephalon |
|
|
|
The cerebrum comes from what embryonic structure of the brain?
|
forebrain
|
|
|
|
What makes up the cerebrum?
|
cerebral cortex
subcortical structures- basal ganglia, thalamus, and hypothalamus |
|
|
|
Cerebral cortex:
Derived from what embryonic structure? Fxn? |
-forebrain
-motor control, sensory perception, cognition, emotion |
|
|
|
Basal ganglia:
Derived from what embryonic structure? Fxn? |
forebrain
motor control, cognitive processing |
|
|
|
Thalamus:
Part of brain? Fxn? |
-forebrain/ cerebrum
-gateway to cerebral cortex |
|
|
|
Hypothalamus:
Derived from what embryonic structure? Fxn? |
forebrain
homeostasis |
|
|
|
Midbrain is made up of what?
|
superior colliculus
inferior colliculus midnrain tegmentum |
|
|
|
superior colliculus
Part of Brain? Fxn? |
midbrain
eye movements |
|
|
|
inferior colliculus
Part of Brain? Fxn? |
midbrain
hearing |
|
|
|
midbrain tegmentum
Fxn? |
motor control
signaling pain |
|
|
|
Hindbrain includes what?
|
medulla oblongata
cerebellum pons |
|
|
|
Medulla oblongata:
part of brain? Fxn? |
hindbrain
regulates viscera |
|
|
|
Cerebellum
part of brain? Fxn? |
hindbrain
coordination of movement |
|
|
|
pons
part of brain? Fxn? |
hindbrain
relay from cerebral cortex to cerebellum |
|
|
|
What are the axes for specifying directions in the CNS different in the brain and spinal cord?
|
b/c there are flexures that bend it forward (cephalic, cervical) and then backward (pontine)
|
|
|
|
What are the 3 main functional systems of the nervous system?
|
snesory
motor autonomic (sensory & motor for visceral organs) |
|
|
|
what is the dominant structure of the human brain?
|
cerebral cortex
|
|
|
|
What part of the brain is responsible for many aspects of higher brain fxn?
|
cerebral cortex
|
|
|
|
What are the major functional modalities of the cortical sheet?
|
senses, movement, cognition, and emotion
|
|
|
|
The nervous system forms out of the ___?
|
embryonic ectoderm?
|
|
|
|
What are the 3 main steps of brain development?
|
1. nervous sytem froms from embryonic ectoderm
2. proliferation of cells in neural tubes leads to hind, mid, and forebrain 3. Nervous system bends/flexes to accommodate human position |
|
|
|
How does ecotderm become the neural tube? What is happening at the same time?
|
Ectoderm folds forming neural grove, which then becomes the neural tube
Neural crest cells migrate to form dorsal root ganglia and some of the adrenal gland |
|
|
|
Parts of hindbrain, and what they develop into?
|
Myelencephalon= medulla
Metencephalon= pons and cerebellum |
|
|
|
Parts of midbrain, and what they develop into?
|
Mesencephalon= midbrain
|
|
|
|
Parts of forebrain, and what they develop into?
|
diencephalon= thalamus, hypothalamus, retina
Telencephalon= cortex |
|
|
|
Cervical flexure?
|
bends ventrally= caudal to hindbrain
|
|
|
|
Pontine flexure?
|
bends dorally @ level of pons
|
|
|
|
Cephalic flexure?
|
bends ventrally at level of midprain
|
|
|
|
General fxn: Cerebellum
|
mediates coordinated movement
|
|
|
|
General fxn: Medulla
|
mediates basic bodily fxns, like breathing
|
|
|
|
General fxn: Pons
|
bridge between cerebrum and cerebellum
|
|
|
|
General fxn: Midbrain
|
sensory and motor
|
|
|
|
General fxn: Thalamus
|
gateway for sensory stimuli to enter cortex
|
|
|
|
General fxn: Hypothalamus
|
collection of nuclei that mediate thirst, hunger, and other critical drives
|
|
|
|
General fxn: Corpus callosum
|
main connection btwn left and right hemispheres
|
|
|
|
General fxn: bsal ganglia
|
involved in movement
|
|
|
|
rostral
|
toward the nose
|
|
|
|
caudal
|
toward the tail
|
|
|
|
dorsal
|
toward the top of the skulll
|
|
|
|
Ventral
|
towards the bottom of the skull or ventebral column
|
|
|

Name
Origin Distribution |
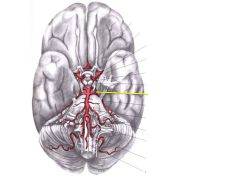
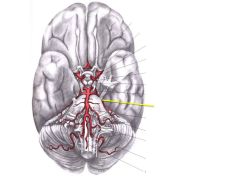
Anterior Communicating Artery
Anterior cerebral circal of willis |
|
|

Name
Origin Distribution |
Anterior Cerebral Artery (ACA)
Internal carotid medial surfaces of the brain (w/ in longitudinal fissure i.e. cingulate cortex) |
|
|

Name
Origin Distribution Gives rise to? |
Middle Cerebral artery
Internal carotid lateral surface of brain-temporal, parietal, frontal Lenticulostraite perforating arteries- supplies basal ganglia Anterior choroidal artery-supplies choroid plexus w/ in lateral ventricles, hippocampus, and amygdala |
|
|

Name
Origin Gives rise to? |
Internal Carotid
common carotid Rise to: Middle cerebral artery Anterior Cerebral Artery Ant./post communicating arteries |
|
|

Name
Origin Distribution |
Anterior Choroidal Artery
Middle Cerebral Artery hippocampus, amygdala,choroid plexus w/ in the lateral ventricles |
|
|

Name
Origin Distribution |
Posterior Communicating Artery
Internal Carotid Artery circle of willis: connects posterior cerebral artery to internal carotid/middle cerebral/anterior cerebral |
|
|
Name
Origin Distribution Rise to? |
Posterior Cerebral Artery
Basilar Artery Occipital lobe Posterior choroidal Artery |
|
|
Name
Origin Distribution |
Superior Cerebellar Artery
Basilar Artery 3rd of 3 vessels to supply the cerebellum |
|
|

Name
Origin Distribution |
Anterior Inferior Cerebellar Artery (AICA)
Basilar A. 2nd of 3 vessles to supply cerebellum |
|
|

Name
Origin Gives rise to? |
Basilar A.
joining of verterbal arteries AICA, Pontine Artery, Superior Cerebellar A., PICA |
|
|

Name
Origin Distribution |
Posterior Inferior Cerebellar Artery
Verterbral Artery 1st of 3 vessels to supply the cerebellum |
|
|

Name
Origin Distribution Rise to? |
Vertebral
Subclavian a. Major blood supply to brain Anterior Spinal Artery, PICA |
|
|

Name
Origin Distribution |
Anterior Spinal Artery
Vertebral Artery Ventral 2/3 of spinal cord |
|
|

Number 3
Name Origin Distribution |
Pontine Artery
Basilar A. Pons |
|
|
|
Lenticulsotriate perforating artery:
-origin -distribution -fact |
middle cerebral artery
supplies basal ganglia suscpeptible to stroke |
|
|

Nerve, #
Function |
Olfactory, I
|
smell info from olfactory epithelium/olfactory bulb to olfactory cortex
|
|

Nerve, #
Function |
Optic, II
visual info from the retina to higher brain levels |
|
|
Nerve, #
Function |
Occulomotor, III
innervates 4 extraoccular muscles: superior, medial, inferior rectus, and infererior oblique pupil light reflex |
|
|

Nerve, #
Function |
Trochlear Nerve, IV
innervates superior oblique (only cranial nerve to protrude from the dorsum of the brainstem) |
|
|

Nerve, #
Function |
Facial nerve, CN V
motor- muscles of mastication sensory- to face V1= opthalmic V2= maxillary V3= mandibular |
|
|

Nerve, #
Function |
Abducens 6
lateral rectus extraoccular muscle |
|
|

Nerve, #
Function |
facial, 7
motor- muscles of the face sensory- taste from ant. 2/3 of tongue |
|
|

Nerve, #
Function |
Vestibulocochlear nerve
hearing and vestibular info from inner ear to brainstem |
|
|

Nerve, #
Function |
Glossopharyngeal nerve, IX
sesory from the pharynx to the CNS taste from post. 1/3 of tongue |
|
|

Nerve, #
Function |
Vagus, X
muscles- palate, pharynx, larynx parasympathetics structure to structures down to the transverse colon |
|
|

Nerve, #
Function |
Accessory, XI
trapezius, scm |
|
|

Nerve, #
Function |
hypoglossal, XII
innervation to the tongue |
|
|
|
Describe CSF flow
|
1. made in choroid plexus of lateral ventricles
2. flows into 3rd ventricle via the foramen of monro 3. flows into 4th ventricle via cerebral aqueduct 4. exits into subaracnoid space via the medial foramen of magendie and the lateral foramen of luschka 5. bathes brain until it is passed into venous drainage via the arachnoid granules |
|
|
|
What are the properties of axons that slow it down?
|
resistive shunt (leakage)
capacitive shunt (stretch) |
|
|
|
What does the resistive shunt do to neuron signals?
|
decrease in amplitude as they travel down the axon's length
|
|
|
|
Signal decay from resistive shut is proportional to?
|
resistivity of the membrane/resistivity of the intracellular fluid
|
|
|
|
A high membrane resistance does what to the signal?
|
limits decay (keeps signal inside the axon)
|
|
|
|
A low intracellular resistance does what to the signal?
|
decreases decay (signal wants to travel inside the axon- less leakage)
|
|
|
|
What causes capacitive shunt?
|
the fact that axons are "stretchy" and can store charge on their membrane
|
|
|
|
What happens to signals due to capacitive shunt?
|
they get smeared out and run down in amplitude as the travel down the axons length?
|
|
|
|
What are ways to over come CAPACITIVE shunt?
|
low intracellular resistance (want to travel inside)
low membrane capacitance (want to travel inside) low signal frequency (time to reach peak) |
|
|
|
How has the nervous system dealt w/ resistive and capacitive limitiation? How doe these works?
|
Large diameter axons- both:
Limits rundown: less resistance (somehow also has capacitive effect) Increased coduction velocity Myelination- both: Limits run down: incr. membrane resistance (dec resistive shunt); dec. membrane capacitannce (dec. capacitive shunt) Increases Conduction Velocity |
|
|
|
What myelinates nerves in the PNS?
|
schwann cells
|
|
|
|
What myelinates nerves in the CNS?
|
oligodendrocytes
|
|
|
|
What is the goal of action potentials?
|
active regeneration of the electrical signal along the way
|
|
|
|
What drives action potentials?
|
ion channels w/ in the neuron's plsama membrane, allowing for the flow of ions
|
|
|
|
Equilibrium potential:
Ca Na Cl K |
Ca: 120
Na: 35 Cl: -70 K:-90 |
|
|
|
What is reverse potential?
|
equilibrium potential w/ more than one ion
|
|
|
|
What happens to a membrane's potential when it is different than the potential of an ion whose channel opens?
When it is the same? |
membrane potential is driven to equilibrium potential of ion
you are clamping the cell at that voltage, making it difficult for the cell's membrane potential to change |
|
|
|
What is more important for changing membrane potential: channel opening or ion concentration?
Exception? |
channel opening (takes a relatively small amount of ions for change)
exception= Ca (kept at low levels inside the cell) |
|
|
|
Properties of ion channels:
|
Gating: close or open due to voltage/ligands
Inactivation- ion can't pass through leak: neither gating or inactivation |
|
|
|
Inactivation/gating trumps inactivation/gating
|
inactivation trumps gating
|
|
|
|
Voltage gated Na channels
gating: inactivation mechanism?: |
opens when positive
yes |
|
|
|
Voltage gated K channel 2.1
gating: inactivation mechanism?: |
opens when positive
no |
|
|
|
Voltage gated K channel 4.1
gating: inactivation mechanism? |
more positive
yes |
|
|
|
HERG channel
gating: inactivation mechanism?: |
opens when positive
yes- faster! |
|
|
|
Inwardly reactifying K channel (Kir)
gating: inactivation mechanism?: |
close when more positive
unknown |
|
|
|
Ca-activated K channel
gating: inactivation mechanism?: |
open when intracellular Ca increases
unknown |
|
|
|
Describe the sequence of action potential generation.
|
1. signal deppolarizes
2. depolarization turns off Kir channels- no K out- faster depol 3. At threshold, Na channels open- potential spikes 4. spike shut off by 1.)inactivating Na channels, opening voltage K channels (K flows out, goes towards potential of K) 5. voltage K channels close slowly- undershoot of potential (corrected by K leaking back into cell) 6. Inactivation of Na channels is removed (end of absolute refractory period) 7. Relative refractory period as it is recovering from undershoot- AP can be produced but initial stimulation must be more intense |
|
|
|
How are ion channels selective for a particular ion?
|
Multiple pores- favorable for 1 type of ion
Like to sit in pores, but like-charge repulsion counterbalances to keep them from getting stuck in pores When an extra ion comes along, it can push into a pore, pushing out another ion at no energy cost |
|
|
|
How does voltage-gating occur?
|
Channels have helices covered w/ positive charges
Depol. allows positive charges to come into the cell= repulsion= shift of helix= opens channel |
|
|
|
How do voltage-gated channels become leaky?
|
Helices should be lined w/ positive charges, pockets should be lined w/ negative charges to ensure helices fit well
Mutating positive charges on helices= doesn't fit as well= ions are allowed to pass |
|
|
|
What is the stucture of electrical synapses?
|
6 connexins form one connexon
2 connexons form 1 gap junction |
|
|
|
Favorable properties of electrical synapses?
|
fast
can synchronize activty (rythm generating cells, neuroendocrine cells) |
|
|
|
A postsynaptic response is only seen when...?
|
presynaptic cell is stimulated to threshold
Threshold= point @ which presynaptic voltage-gated Na channels open, allowing AP generation, and signal to be passed to postsynaptic cell |
|
|
|
Electically blocking Ca entry into the presynaptic cell:
-how? -results? |
how: voltage clamping the cell @ Ca's equilibrium potential
Results: prevents electrical signals from being passed to the postsynaptic cell |
|
|
|
What must be present around the presynaptic nerve terminal when the action potential invades in order for a postsynaptic response to be elicited?
|
Ca
|
|
|
|
What did the experiment with MEPPs find?
|
MEPPs occur in integers, which means...
Presynaptic sells has "n" nt quanta each w/ the same probability "p" of being releases |
|
|
|
In the pns n is ___ and p is ___; which means that ___ statistics are used
|
very large
very small poisson statistics |
|
|
|
In the CNS, n is ___, and p is ___, because of varying ___ levels.
|
very low
not the same for each varying Ca levels Therefore its hard to apply quantal analysis |
|
|
|
What happens to the membrane capacitance of the presynatpic cell every time a quantal release is detected in the postsynaptic cell? why?
|
membrane cpacitance of presynaptic increase
due to fusion of the nt vessicles to the presynaptic axon terminal |
|
|
|
3 facts learned from nt experiments?
|
synpatic transmisioon:
1. triggered by AP invading presynaptic axon terminal 2. depends on Ca influx into the presynaptic cell 3. is quantal in nature |
|
|
|
Give the full story of nt:
|
1. stimulate presynaptic= AP
2. AP to axon terminal= opens voltage Ca chennels 3. Ca into axon terminal= fusion of nt quanta to plasma mebrane 4. Nt released onto postsynaptic neuron 5. Nt binding to receptors= excitatory potential in postsynaptic neuron 6. potential reaches threshold= opens voltage Na channels= AP= continued propagation of signal |
|
|
|
3 things that can happen to nt that is released from a presynaptic cell
|
degraded by enzyme
reuptaken bind to a postsynaptic receptor an elicit a response |
|
|
|
2 ways the neurotransmitters can be reuptaken?
|
direct- presynaptic cell reuptakes
indirect- glial cells reuptake and transfer back to presynaptic |
|
|
|
How does nt vessicle fussion occur?
|
Ca binds to protein called synaptotagmin (v-SNARE) on nt vesicle
Synaptogmin binds to SNAP-25 and synataxin (t-snares) forming SNARE complex Vesicle fusion then occurs |
|
|
|
ionotropic receptor?
|
ion channels that open when nt binds
fast |
|
|
|
metabotropic receptors?
|
g-protein coupled receptors that stimulate a G protein to open a nearby ion channel when activated by a G protein
slow |
|
|
|
What determines wheher a nt is excitatory or inhibitory?
|
nt receptors, not the nt itself
|
|
|
|
Ach:
location? types of receptors? |
@ neuromuscular jx
ionotropic= nicotnic ACh receptors (nAChR) metabotropic= muscarinic ACh recptors (mAChR) |
|
|
|
How do the nicotinic ACh receptors work?
|
ionotropic
non-selectively allow k and Na ions to pass when bound by ACh ACh binds= hydrophobic residues in core move= ions allowed through Have reverse potential between K and Na (-15 mV) |
|
|
|
What is the major excitatory nt of the nervous system?
|
gluatamate
|
|
|
|
What type of receptors does glutamate have?
|
ionotropic= AMPA, Kainate, NMDA
metabotropic= metabotropic glutamate receptors (mGluRs) |
|
|
|
AMPA recptors?
|
ionotropic glutamate receptors
Fast non-selectively allow K and Na through like kainate receptors |
|
|
|
Kainate receptors
|
onotropic glutamate receptors
Fast non-selectively allow K and Na through like ampa receptors |
|
|
|
NMDA receptors?
|
ionotropic glutamate receptors
slow allow K, Na, and Ca thru Have MG ion blocking ion flow @ hyperpolarized potentials, so they need gluatamate bound and cell in depolarized state to be opened |
|
|
|
What is the major inhibitory nt in the brain?
What type(s) of receptors does it have? |
GABA
ionotropic and metabotropic |
|
|
|
How can GABA cause inhibition?
|
1. Drive membrane potential toward Cl= can't reach AP threshold
2. Shortens length constant= signal decays a lot along end of axon= less spatial summation (less signals from different parts of neurons coming together= less likely to reach AP threshold 3. shortens time constant= little smearing out of electrical signal in time= less temporal summation ( signals from different times can add up)= less likely to reach AP threshold |
|
|
|
What is the major inhibitory nt in the spinal cord?
|
glycine
|
|
|

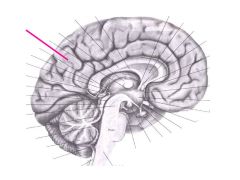
fxn?
|
Pons
connection point for communications between cerebrum and cerebellum |
|
|

fxn?
|
cerebral peduncle
a bunle of axons transmitting info from motor cortex to spina cords (in medulla=pyramids) |
|
|

fxn?
|
medulla
the most caudal part of the brain stem controls basic functions like breathing |
|
|

describe
|
4th ventricle
CSF-filled cavity at the level of the cerbellum |
|
|

fxn
|
midbrain
motor vision (superior colliculus) hearing (inferior colliculus) |
|
|

fxn
|
cerebral aqueduct
connects 3rd and 4th ventricles |
|
|

fxn
|
thalamus
gateway for sensory info from periphery to enter cortex |
|
|

fxn
|
hypothalamus
basic drives- hunger, thrist, anger, etc. pituitary comes off of it |
|
|

fxn?
|
cerebellum
coordinated movements |
|
|

fxn
|
corpus callosum
what matter that is the major connection from one brain hemisphere to another |
|
|

fxn
|
fornix
carries info from hippocampus to mammilary bodies involved in learning and memory |
|
|

fxn
|
temporal lobe
learning and memory |
|
|
fxn
|
parietal lobe
bodily sensation and attention |
|
|

fxn
|
occipital lobe
vision |
|
|

fxn
|
insula
cortex at very bottom of lateral sulcus emotion |
|
|
fxn
|
longitidunial fissure
divides L and R hemispheres |
|
|

fxn?
|
lateral suclus
separates temporal and parietal lobes |
|
|

fxn
relationships? |
central sulcus
separates frontal and parietal lobes motor cortex= anterior (in frontal lobe) somatosensory cotex= posterior (in paritetal lobe) |
|
|

fxn
|
cingulate sulcus
superior to cingulate gyrus, which is involved in emotion |
|
|

fxn
|
calcarine sulcus
cortex on either side of sulcus involved in vision |
|
|

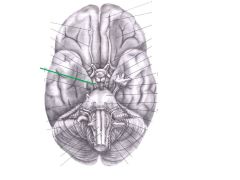
|
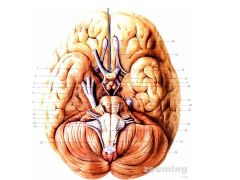
olfactory bulb
|
|
|
|
optic chiasm
|
|
|

|
optic tract
|
|
|

|
hypophysis (pituitary gland)
|
|
|

|
cerebral peduncle
|
|
|

|
pons
|
|
|

|
middle cerebellar peduncle
|
|
|

|
medulla
|
|
|

|
medullary pyramid
|
|
|

|
cerebellum
|
|
|

|
corpus callosum
|
|
|

fxn
|
anterior commisure
fxn- links limbic structures in medial temporal lobe and vental part of frontal lobe |
|
|

|
caudate nucleus (basal ganglia)
|
|
|

|
putamen
|
|
|

fxn
|
internal capsule
fxn- carries axons btwn cortex and subcortical structures (thalamus, brainstem, spinal cord) |
|
|

fxn
|
globus pallidus
fxn: pathway for output from stratium to thalamus |
|
|

|
accumbens nucleus
|
|
|

|
accumbens nucleus
|
|
|

fxn
|
amygdala (basal ganglia)
limbic system emotion/affective behavior |
|
|

|
globus pallidus
|
|
|

|
lateral ventricle
|
|
|

fxn
|
thalamus
fxn: input sensory/motor to localized parts of cerebral cortex |
|
|

|
internal capsule
|
|
|

|
thalamus
|
|
|

|
internal capsule
|
|
|

|
puntamen
|
|
|
|
cerebral punducle
|
|
|

|
substantia nigra
dopamine containing cells that can cause Parkinson's when damaged |
|
|

|
red nucleus
|
|
|

fxn
|
hippocampus
memory processing |
|
|

fxn
|
chorid plexus
secretes CSF into ventricles |
|
|

|
parahippocampal gyrus
|
|
|

|
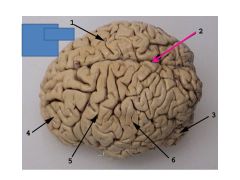
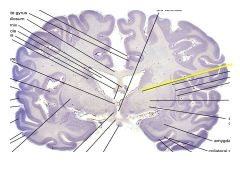
1= body of corpus callosum
2= choroid plexus 3= lateral ventricle |
|
|

|
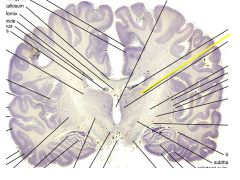
1= head of caudate nucleus
2= capsule 3= puntamen 4= septum pelucidum 5= genu of corpus callosum |
|
|

|
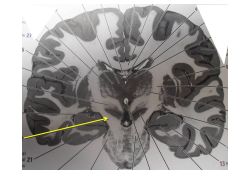
1= thalamus
2= lateral ventricle 3= genu of corpus callosum 4= caudate nucleus 5= putamen |
|
|

|
1= chroid plexus
2= lateral ventricle 3=thalamus 4= puntamen |
|
|

|
1= hippocampus
2= globus pallidus 3=puntamen |
|
|

|
1= lateral ventricle
2= hippocampus 3= red nucleus 4= substantia nigra |
|
|

|
cerebral punducle
|
|
|
|
Where is the fornix and what does it do?
|
between the lateral ventricles
Carries info from hipocampi to mamillary bodies |
|
|
|
what makes up the striatum?
|
the caudate, the nucleus accumbens, and the putamen
|
|
|
|
If the caudate and the putamen are not connected, which structure is missing?
|
the nucleus accumbens
|
|
|
|
What 2 major tracts connects the hemispheres?
|
corpus collosum, anterior commisure
|
|
|
|
if you can see the third ventricle, you can see what?
|
the thalamus
|
|
|
|
__ sits on top of the internal capsule, __ & __ sit below the internal capsule
|
thalamus
putamen, globus pallidus |
|
|
|
If you can see the ____ then you can't see the amygdala
|
hippocampus
|
|
|
|
What 2 structures identify the midbrain?
|
cerebral aqueduct btwn 3rd and 4th ventricles
cerebral peduncles (continuation of internal capsule |
|
|
|
what separates the internal capsule from the cerebral punducles?
what is their typical shape? What are the they target of? |
lateral geniculae nuclei
layered, peak shape, target of the optic tract |
|
|
|
What makes the wall of the third ventricle?
the roof? |
thalamus
fornix |
|
|
|
Describe the development of the optic cup and the formaption of the eye from it
|
diencephalon-> optic vesicle-> invaginates-> optic cup-> inner layer= neural retina, outer layer= pigment epithelium of retina-> outer edge both layers combine -> secretory epithelium over ciliary body; epithelum on the back of the iris
|
|
|
|
describe the development of the lens
|
lens placode induced in surface ectoderm>> invaginates>> pinches off>> forms lens vesicle>> cells inside form lens fibers>> lens epithelium forms
|
|
|
|
Describe the development of the cornea?
|
forms in front of lens from a combination of surface epithelium and underlying mesoderm
mesoderm condenses into pigmented vascular layer, chorid, and dense sclara |
|
|
|
choroid is comparable to __?
dense sclera is continous w/ ___? |
pia/arachnoid around brain
dura mater |
|
|
|
Describe the path of aqueous humor
|
ciliary epithelium-> posterior chamber-> anterior chamber-> reabsorbed thru trabecular meshwork -> through schlemm's canal-> aqueous veins
|
|
|
|
What happens when there is excessive secretion of aqueous humor or blackage of its outflow?
|
increased intraocular pressure= glaucoma
|
|
|
|
3 criteria to be considered a nt?
|
1. present in presynaptic terminal
2. released when presynaptic terminal is stimulated 3. must have postsynaptic receptors |
|
|
|
amino acid nt?
|
glutamate, GABA, glycine
|
|
|
|
catecholamine nt?
|
dopamine, norepi, epi
|
|
|
|
Small molecule vs. Peptide nt:
synthesis |
small- at synaptic terminal
peptide- in cell body as precursor protein |
|
|
|
Small molecule vs. Peptide nt:
vessicle? |
S: small, clear or large dense
P: large, dense only |
|
|
|
Small molecule vs. Peptide nt:
frequency stimulation |
S: low
P: high |
|
|
|
Small molecule vs. Peptide nt:
release location? |
S: apex of synaptic terminal
P: sides of synaptic terminal |
|
|
|
Small molecule vs. Peptide nt:
Receptor affinity/concentration |
S: low affinity, high concentrations
P: high affinity, low concentrations |
|
|
|
Small molecule vs. Peptide nt:
duration of action? |
S: short
P: long |
|
|
|
Small molecule vs. Peptide nt:
inactivation/reuptake? |
S: fast inactivation/reuptake
P: slow inactivation/no reuptake |
|
|
|
Small molecule vs. Peptide nt:
location of effects |
S: short range
P: long range |
|
|
|
major transmitter of neuromuscular jxn?
|
ACh
|
|
|
|
how is ACh formed?
|
acetyl CoA + choline joined by choline acetyl transferase (ChAT)
|
|
|
|
What degrades ACh?
|
acetylcholinesterase into acetate and choline (choline reuptaken)
|
|
|
|
Dopamine binds to what type of receptors?
|
metabotropic
|
|
|
|
How is dopamine synthesized?
|
Tryrosine--(tyrosine hydroxylase)--L-DOPA--(DOPA decarboxylase)-- dopamine
|
|
|
|
How is dopamine reuptaken?
|
DAT
|
|
|
|
What effect does cocaine have on nt?
|
block DAT- prevents dopamine reuptake
block NET- prevents NE reuptake block- SERT-prevents serotonin reuptake |
|
|
|
What affect does amphetamine have?
|
similar structure as dopamine
Can be reuptaken by DAT and into dopamine containing vessicle Dopamine forced out of vessicles into cytoplasm Cytoplasmic dopamine gets pumped out into the synapse by reverse transport thru DAT Same for NET and SERT huge release of dopamine |
|
|
|
What happens to the synapse w/ chronic use?
|
less presynaptic vessicles
less postsynaptic receptors |
|
|
|
NE binds to what types of receptors?
|
metabotropic
|
|
|
|
How is NE synthesized?
|
from dopamine by dopamine b-hydroxylase
|
|
|
|
how is Ne reuptaken?
|
by NET
|
|
|
|
How does ectasy (MDMA) work?
|
similar structure as serotonin
Can be reuptaken by SERT and into serotonin containing vessicle Serotonin forced out of vessicles into cytoplasm Cytoplasmic serotonin gets pumped out into the synapse by reverse transport thru SERT |
|
|
|
How are peptide nt synthesized?
|
Prohormones have sequence signals that send them to the ER to be packaged into vesicles
Vesicles are transported down the axon lenth while prophormone is cleaved at dibasic signals If glycine is made, it has to amidated once dibasic cleaving is turn off |
|
|
|
features of non-convential nt?
|
1. can pass thru membanres
2. doesn't need a receptor 3. short lived |
|
|
|
Examples of non-conventional nt?
|
CO
Endocannabinoids NO |
|
|
|
What is THC?
|
the active substance in marijuana that mimics the body's natural endocannabinoids
|
|
|
|
How does NO pathway work?
|
1. Glutamate activates nMDA receptors
2. NMDA receptors allow Ca inside 3. Ca activates NO synthase 4. NO synthase converts arginine to NO 5. NO activates guanylyl cyclase 6. guanylyl cyclase increases levels of cGMP 7. cGmP effects glial cells and the presynaptic cell |
|
|
|
What type of receptors are GPCRs?
|
metabotropic receptors
|
|
|
|
What are the GPCR motifs?
|
trafficking motifs- bring to plasma mebrane
interaction motifs - allow to interact w/ other proteins (i.e Homer) |
|
|
|
What is Homer and how does it work?
|
Linker protein for glutamate GPCR (mGluR)
1. holds receptor close to ER calcium stores 2. holds receptor close to NMDA receptors |
|
|
|
Why is dimer formation important for GPCRs?
Example |
It can:
1. make receptor fxnl 2. change ligand binding 3. change signaling cascade 4 change trafficking GABAb receptor is a dimer of R1 (binds GABA) and R2( traffics to membrane) |
|
|
|
Mechanisms of receptor desensitization?
|
1. phosphorylation
2. sequestration/downregulation of receptor (B-arrestin internalizes receptor) 3. RGS proteins- enhase GTPase activity of Galpha subunit of G proteins |
|
|
|
What do plasma membrane transporters use to reuptake neurotransmitters?
|
ionic gradients
|
|
|
|
When do plasma membrane transporters undergo reverse transport?
|
if too much substrate builds up where it is not supposed to
|
|
|
|
Which is faster, plasma membrane transporter or degradation enzyme?
|
plasma membrane trasmitter
|
|
|
|
Which are faster carrying ions: channels or transporters?
|
channels
|
|
|
|
2 classes of plasma membrane transporters? describe
|
Na,Cl-dependent
-many different nt. -on presynaptic cell - uses na symport (except SERT-K antiport) -alternatic access conformation change- extracellular/intracellular Na,K dependent membrane transmitters -EAAT- glutamate transporters -on glial cells/ post-synaptic cells -2 hairpin loops that fo 1/2 way into lipid bilayer -Na,K antitransporter, Cl tranport in also |
|
|
|
2 types of vesicular transporters? descibe
|
SLC 17 transporter
- transport glutamate -use H+ (inside)and Cl- gradient CLC18/32 transporters -many different forms for different nt -use H+ gradient |
|
|
|
What is volume transmission?
|
a nt spilling out of the synaptic cleft and activating far away receptors (on soma or other parts of the dendrite_
|
|
|
|
low-affinity,high capacity plasma membrane transporters:
-describe -features? |
features: are not blocked by SSRIs, and negate the therapuetic effect of SSRIs by reuptaing serotonin from the synaptic cleft
Oct- on glia, reuptake dopamie, ne, serotonin PMAT- on neurons, reuptake dopamine and serotonin |
|
|
|
How does gene expression make diverse brain structures despite the limited number of genes?
|
-varying spatial gradeints
-varying time gradients -varying compinatorial pairs |
|
|
|
Describe the Spemann Man gold experiment
|
1. taking blastopore lip from one embryo and transplanting it to another causes recipeint embryo to have 2 heads
2. both heads derived from recipient embryo, but CHEMICALS secrete from transplant cause the nearby tissue to be patterned into a head |
|
|
|
how did patterning of gene expression lead to the development of the nervous system
|
Patterning-->turns ectodermal cells into neural plate--> neural plate folds over itself to create neural tube
|
|
|
|
rhombencephalon?
|
hindbrain
|
|
|
|
mesencephalon?
|
midbrain
|
|
|
|
proencephalon?
|
forebrain
|
|
|
|
What causes holoprosencephaly?
|
mutations in the morpogenic sonic hedgehog (SHH) or the transcription factor six3
brain doesn't develop into 2 hemispheres |
|
|
|
Describe how SHH works in the ventral spinal cord progenitors
|
SHH levels are high --> nkx2.2 gene is turned ON AND Pax 6 gene is turned OFF --> progenitor turns into a motor neuron
|
|
|
|
What happens if SHH is knocked out?
|
certain genes, i.e. Dbx are expressed
This dorsalizes the spinal cord- genes that would only be expressed in the dorsal spinal cord go unckeced |
|
|
|
What is the SHH receptor, what happens if it has a defect?
|
Receptor= Patched
Defect could lead to unchecked neural expansion in the cerebellum producing tumors (medulloblastomas) |
|
|
|
When do neurons finish differentiating?
|
before birth
|
|
|
|
When do astrocytes finish differentiating?
|
shortly after birth
|
|
|
|
When do oligodendrocytes finish differentiating?
|
long after birth
|
|
|
|
Name 2 places where neural progenitor cells remain the brain thru adulthood?
|
subventricular zone
subgranular layer of the hippocampus |
|
|
|
Excitatory neurons use ?? to get to the right place in the nervous system?
|
radial migration
|
|
|
|
Describe neural migration
|
1. neurons born near the ventricle (ventricular zone)
2. migrate radially out toward the pial surface from the bulk of the cortex a. climb radial glia that stretch from ventricular zone to pial surface b. guided by reelin- tells them where to stop c. older neurons, that are in deeper cortex layers, are used as stepping stoes for newer born neurons to get into more superficial layers |
|
|
|
mutations of reelin causes?
mutations of reelin receptor causes? |
norman roberts syndrome- smooth brain
VLDLR-associated cerebellar hypolasia |
|
|
|
Inhibitory neurons use ??? to migrate to where they need to be
|
tangential migration
migrate parallel to the surface of the brain |
|
|
|
Describe spinal cord development
|
1. ventricular zone: layer of progenitor cells surrounding CSF-filled canal
3. cells migrate out forming primitive gray mater w/ alar plate (dorsal horm) and basal plate (ventral horn) 4. sulcus limitans separates alar and basal plates 5. ventarl portion = floor plate; dorsal portion= roof plate that is made of ependymal cells that line the central canal and overly the pia mater (has no neural tissue) 6. The interomediolateral nucleus is contained in spinal levels T1-L2 and gives rise to the body's preganglionic fibers |
|
|
|
define sensory transduction?
|
converting sensory stimuli to electrical signals
|
|
|
|
What is the first location of visual processing?
|
retinal- neural tissue lining the back of the eye, done by the photoreceptors
|
|
|
|
rhodopsin is a photopigment for which photoreceptor? most sensitive to what color light?
|
Rods
green light |
|
|
|
cone opsins are most sensitive to what color light?
|
red
green blue |
|
|
|
The phototransduction cascade is what type of mechanism?
Describe |
metabotropic mechanism
1. rhodopsin/cone opsin absorbs a photon of light 2. 11-cis retinal is converted to all-trans retinal 3. rhodopsin/cone opsin confirmation change 4. transducin (g protein ) is activated 5. alpha subunit of transducin activates phosphodiesterase 6. phosphodiesterase breaks down cGMP (which is consituitively made in the cell) 7. low cGmP lvels close cyclic nucelotided gated channels (cation channels) 8. cell is hyperpolarized (light has turned into an electrical signal) |
|
|
|
How is the photoresponse tuned off?
|
1. light stimulus is shutt off
2. kinase phosphorylates rhodopsin/cone opsin (1/6 sites) 3. B- arrestin internalizes phosphorylated protein 4. all-trans retianal is removed, regenerated into 11--cis retinal, and put back in 5. rhodopsin/cone opsin then transported back to the membranous disks of the photoreceptor;s outer segment (original location |
|
|
|
Which is more sensitive to light, why?
|
rods are more sensitive b/c:
1.spontaneous isomerization of 11-cis to all-trans retinal occurs more often in cone opsin 2. cones have different isoforms of some of the phototransduction machinery (different functional properties) |
|
|
|
light adaptation?
|
photoreceptors make themselves less sensitive to light so they can respond to the brighter parts of the 7 orders of magnitude of possible light stimuli w/ out being saturated (can only operate over about 2 orders of magnitude)
|
|
|
|
dark adaptation?
|
photoreceptors make themselves more sensitive to light, allowing themselves to respond to the dimmer light stimuli
|
|
|
|
adaptation to light involves what ion? which photoreceptors are best at adapting?
|
Ca
cones |
|
|
|
What 2 senses use metabotropic sensory transduction?
why is this type of sensory tranduction beneficial? |
Vision, smell
it can amplify the signal |
|
|
|
what senses use ionototropic sensory transduction?
why is this type of sensory transduction beneficial? |
hearing
it is very fast |
|
|
|
Olfactory transduction is what type of sensory transduction?
Describe |
metabotropic
1. odorant activates odorant receptor 2. odorant receptor acitaves Golf (g protein) 3. alpha subulit of Golf activates adenylate cyclase 4. more cAMPs is produces 5. more cAMP= opens more cyclic nucleotide gate channels (cation channels) 6. cell depolarizes in response to odorant |
|
|
|
What are the 4 types of somatosensation?
|
fine touch- texture vibration
pain/temperature proprioception- unconcious pereception of where our limbs/muscles are in space visceral sensation- unconcious perception of stimuli affecting visceral organs |
|
|
|
Fine touch:
-define -receptors? -where signals travel |
-conscious perception of touch
-mechanoreceptors: hair follicle, merkel disks, meissner corpuscle, pacinan corpuscle, ruffini endings -travel in the dorsal colum/medial lemniscal systme (DCML) |
|
|
|
Pain temperature somatosensation:
-receptors where does signal travel? |
nocireceptors (free nerve endings)= pain
thermoreceptors= temp Signal travels from the receptors mainly in the spinothalamic tract of the anterolateral system |
|
|
|
Proprioreception
-define -receptors -where signals travel |
unconcious perception of where our muscles/limbs are in space
proprioreceptors signals carried from proprioreceptors to the cerebellum via the spinocerebellar tract |
|
|
|
Visceral sensation
-define -receptors -where signals travel |
-unconcious perception of stimuli affecting visceral organs
-interorecpetors: stretch, baro, chemo, and flow receptors -signals travel w/ (not in) sympathetic fibers back to effector centers in the brain |
|
|
|
what is referred pain?
|
when visceral sensations are consciously perceived
|
|
|
|
What do mechanoreceptors do?
Properties? |
mediate fine touch
1. have speicialized external structures to detect different stimuli 2. show adaptation- reduced response to repeated stimuli 3. have a receptive field- region of sensory space that will ccause the cell to fire when stimulated |
|
|
|
Smaller receptive feild = higher/lower sensory resolution?
Is sensory resolution higher in the trunk or the fingers? |
higher
higher in the fingers |
|
|
|
Hair follicle receptor:
-fxn -location -adaptation -receptive field size |
fxn: hair bending
location: deep adaptation: fast field size: small |
|
|
|
Merkel Disk
-fxn -location -adaptation -receptive field size |
fxn: steady skin indentation
location: superficial adaptation: slow receptive field size: small |
|
|
|
meissner's corpuscle
-fxn -location -adaptation -receptive field size |
fxn: low freq. vibration/flutter
location: superficial adaptation: fast receptive field size: small |
|
|
|
pacinian corpuscle:
-fxn -location -adaptation -receptive field size |
fxn: high freq. vibration
location: deep adaptation: fast receptive field size: large |
|
|
|
ruffini ending
-fxn -location -adaptation -receptive field size |
fxn: steady brush against the skin
loaction: deep adaptation: slow receptive field size: large |
|
|
|
Proprioreceptive info travels in what type of fibers? describe
|
Aaphla fibers
-large -heavy myelination-fastest |
|
|
|
Fine touch info travels in what type of fibers? describe
|
Abeta fibers
-medium medium myelinzation- 2nd fastest |
|
|
|
Pain/temperature info travel in what type of fibers?
|
Adelta fibers
-small small myelination- 3rd fastes or C fibers -smallest diameter, no myelination-slowest |
|
|
|
Why bother w/ slow fibers?
|
save space in nervous system (small)
more resistant to damage |
|
|
|
Pathway of fine touch from the body
|
1. mechanoreceptors send info to soma of sensory neuron in the dorsal root ganglion
2. neuron sens info into dorsal horn of the spinal cord. 3. It proceeds up to the medulla as part of the dorsal column 4. Once in the medulla it synapses on one of the 2 dorsal column nuclei 5. The cells in the dorsal column nuclei corss over to the contralateral side as the arcuate fibers and ascend as white matter tract called the medial lemniscus 6.The proccesses making up the medial lemniscus synapse on cells in the ventral posterior lateral nucleus of the thalamus 7. VPL proccesses join the internal capsule and travel up to synapse in the primary somatosensory cortex |
|
|
|
Differences in the lower body vs. upper body fine touch
|
in the dorsal column:
-gracile tract-info from the lower (lumbar and sacral) body, runs in medial part of dorsal column - cuneate tract- from upper body (thoracic and cervical), runs in lateral part of spinal cord In dorsal column nuclei (in medulla): gracile and cuneate nucleus, medial and lateral |
|
|
|
Pathway of Pain and temperature from the body
|
1. nociceptors/thermoreceptors send info the sensory neuron in dorsal root ganglia
2. neuron sends another process into the spinal cord (lissauer's tract= entrance into spinal cord) 3. proccesses synapse on a cell w/ in the dorsal horn (substantia gelantiosa/nucleus proprius cells) 4. This cell has its process cross to the contralateral side of the spinal cord and proceeds up as the spinothalamic (aka anterolateral) tract 5.This process synapses on cells in the ventral posterior lateral nucleus of the thalamus 6. VPL cells processes join the internal capsule and travel up synapse in the primary somatosensory cortex (SI) |
|
|
|
Pathway of fine touch from face
|
1. info to trigeminal ganglion
2. neurons sends info into pons and synapses on cells in the principal trigeminal nucleus 3. these cells send processes that cross over to the contralateral side and ascend in the medial lemniscus- some processes don't cross and stay ipsilateral 4. These processes synapse on cells in the ventral posterior medial nucleus of the thalamus 5. The VPM cell processes join the internal capsule and travel up to synapse in the primary somatosensory cortex (s1) |
|
|
|
Pathway of pain/temperature from face
|
1. trigeminal ganglion receives info
2. sends info at the level of the pons 3. descends to synapse on cells w/ in the spinal trigeminal nucleus (in medulla) 4. Cels send processes that cross over to the contralateral side and ascend 5. These processes synapse on cells in the ventral posterior medial nucleus of the thalamus 6. VPM cell processes join the internal capsule and trave up to synapse in the primary somatosensory cortex (s1) |
|
|
|
Pathway Proprioreception from the body
|
1. MUSCLES send info to dorsal root ganglion
2. neuron sends another process into the spinal cord 3. enters spianl cord via the dorsal horn 4. synapses on cells in clarke's nucleus (nucleus dorsalis) in spinal levels T1-L2 5. Cells in Clarke's nucleus send processes to the cerebellum via the spinocerebellar tract (do not cross the midline) |
|
|
|
Proprioreception from the face
|
1. Muscle sends information to the trigenimal mesenphalic nucleus (unique b/c it is w/ in the main neuroaxis)
2. That's all we need to know :) |
|
|
|
Medial lemniscus in the medulla?
|
oritented vertically:
legs-bottom arms- above |
|
|
|
medial mlemniscus in pons?
|
laying down
head, arms, legs |
|
|
|
Somatosensory cortex orientation?
|
medial to lateral:
leg, arm, face |
|
|
|
Where is the primary somatosensory cortex loacated? what is another name for it?
|
behind the central sulcus
S1, postcentral gyrus |
|
|
|
4 arease of the primary somatosensory cortex
|
3a- simple proprioception, lession = defect in fine movements
3b- simple sensation (touch, pain, temp), lesion= dfects in these senses 1- complex sensation= same as 3b w/ more info (direction, orientation dependent, or large fields), lesions cause defects in these senses 2- complex sensation + prorioception, lesions= deficits in task require fine touch and position sense (ie.e maneuver a hand through a tight space) |
|
|
|
Secondary somatosensory cortes?
-input from? -other info |
input-S1 and thalamus
-1st for bilateral stimuli -alter firing properties by attentional state |
|
|
|
intraparietal sulcus
|
complex somatosensory processing
|
|
|
|
area 5
|
recieves info from S2
complex somatosensory processing |
|
|
|
area 7
|
integrates somatosensory and visual info
analyzes spatial properties of things you see |
|
|
|
When do fine touch and pain information cross?
|
fine touch- crosses in the medulla
pain/temperature- crosses immediately after it enters the spinal cord |
|
|
|
Peripheral nerve cut/crush
|
lose fine touch And pain/temp over the distribution of the peripheral nerve
peripheral nerves contain multiple roots= multiple dermatomes |
|
|
|
peripheral nerve metabolic injury
|
metabolic injury= systemic= affects all nerves= bilateral presentation
loss of fine touch and pain/temp; long nerves (i.e. those at tips of hands and feet) most susceptible= stocking-glove deficit distribution |
|
|
|
Dorsal root lesion
|
lose fine touch AND pain/temp ipsilaterally in the affected dermatome (overlap makes fine touch less affected)
|
|
|
|
Central cord lesion
cause results |
from syringomyelia- cyst forming in central canal of spinal cord
damages the pain/temperature info crossing over from both sides of the body on at level of lession areas above and below are ok b/c their info crossed over at higher/lower parts of spinal cord and is running in the spinothalamic tract which is lateral, not in the center |
|
|
|
Dorsal colum lesion
|
ipsilateral fine touch loss from the lesion on down (crossing doesn't happen until the medulla)
|
|
|
|
anterolateral system lession
|
contralateral pain/temp loss from lesion down ( crossing occurs right away in spinal cord)
|
|
|
|
hemitransection of the spinal cord
|
dorsal colum and anterolateral lesion
ipsilateral fine touch loss from lesion on down AND contralateral pain/temp loss from the lesion on down called Brown-sequard syndrome |
|
|
|
complete spinal cord transection
|
complete bilateral sensory loss from the lesion on down
|
|
|
|
complete lesion to half of thalamus
|
complete sensory loss to the entire contralateral half of organism, except the face, b/c the face projects to both sides of the thalamus
|
|
|
|
lesions to s1
|
varies by location (trapeze artists orientaton over the surface of s1)
always contralateral sensory loss to thaat part of the body (all fibers have crossed) |
|
|
|
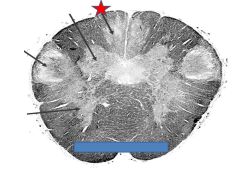
characteristic arrangement of cells w/ in ventral horn?
lateral,medial, dorsal, ventral |
lateral cells- distal musculature
medial cells- proximal musculature dorsal cells-innervate flexors ventral cells-innervate extensors |
|
|
|
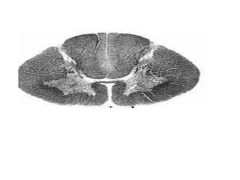
which laers of spinal cord have prominent dorsal and ventral horns? why?
|
cervical and lumbosacral
cervical-sensory lumbosacral-supplies arms and legs arms and legs require a lot of sensory and motor innervation |
|
|
|
List the sections in the order of most to least white matter
|
cervical, thoracic, lumbar, sacral
|
|
|

Identify?
Fxn? |
Ventral posterior latera nucleus
Rine touch and pain/temperature from body |
|
|

Identify?
Fxn? |
Ventral posterior medial nucleus
Rine touch and pain/temperature from face |
|
|

General
identify |
Post. thalamus
Medial geniculate nucleus |
|
|

general
Identify |
Post. thalamus
Lateral geniculate nucleus |
|
|

Identify fxn
|
Venral posterior lateral nucleus
Mediates fine touch and pain/temp sensation from body |
|
|

Identify
Fxn |
Ventral posterior lateral nucleus
Mediates fine touch and pain/temp sensation from face |
|
|
general
Identify |
Anterior thalamus
Ventrolateral thalamus-same spot as VPL just more anteriorly |
|
|

What is the mcc of siderblastic anemia?
|
1) decreased B6
2) INH therapy |
|
|

Identify?
|
Betz cells- give rise to long axons that innervate motor neurons initiating movement
|
|
|

Identify?
|
Somatosensory cotex cortical layer V- sparse b/c layer 5 is mostly efferent, and only motor (not somatosensory) needs efferent fibers
|
|
|

Identify?
|
Somatosensory cotex cortical layer IV- prominent b/c layer 4 is mostly afferent, and somatosensory gets tons of incoming sensory info (much more than motor cotex)
|
|
|

Identify?
Type of neurons |
Ventral horn
Neurons invovled in motor-innervation of muscle |
|
|
|
cervical
|
|
|

|
thoracic
|
|
|

|
lumbar
|
|
|

|
sacral
|
|
|

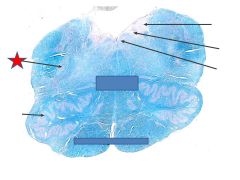
Section of spinal cord/ specific
Fxn? |
Thoracic spinal cord
Lissauer’s tract: entrance of small diameter pain/temp fibers into spinal cord |
|
|

Section of spinal cord/ specific
Fxn? |
Thoracic spinal cord
Intermediolateral nucleus (IML) Gives rise to preganglionic neurons of the sympahtetic nervous system Extends from T1-L2 (thoracic spinal cord) |
|
|

Section of spinal cord/ specific
Fxn |
Thoracic spinal cord
Dorsal colum Made of axons carrying fine touch info up to the medulla, where they will synapse on the dorsal column nuclei |
|
|

Section of spinal cord/ specific
Fxn? |
Thorasic spinal cord
Ventral funiculus- fibers running in ventral part of spinal cord including vestibulospinal tract involved in balance |
|
|

Section of spinal cord/ specific
Fxn? |
Thoracic spinal cord
Lateral funiculus Fiber tracts running in lateral part of spinal cord, includes: Spinothalamic tract- carries pain/temp info to VPL of thalamus Corticospinal tract Spinocerebellar tract- carries proprioceptive info up to the cerebellum |
|
|

Section of spinal cord/ specific
Fxn? |
Thoracic spinal cord
Clarke’s nucleus/nucleus dorsalis Where info from muscles to DRG synapse in spinal cord |
|
|

Section of spinal cord/ specific
Fxn? |
Thoracic spinal cord
Gracile fascilus, cuneate fasciculus |
|
|

Section of spinal cord/ specific
Fxn? |
Thoracic spinal cord
Spinothalamic tract |
|
|

Section of spinal cord/ specific
Fxn? |
Thoracic spinal cord
Corticospinal tract |
|
|

Section of spinal cord/ specific
Fxn? |
Thoracic spinal cord
spinocerebral tract |
|
|
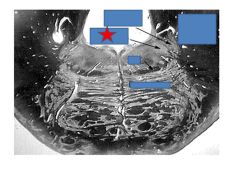
General
Identify Fxn |
Caudal/closed medulla
Gracile nucleus-receives fine touch info from lower body via dorsal column; fibers cross into medial meniscus and ascend to VPL |
|
|

General
Identify Fxn |
Caudal/closed medulla
Cudate nucleus-receives fine touch info fromupperbody via dorsal column; fibers cross into medial meniscus and ascend to VPL |
|
|

General
Identify Fxn |
Caudal/closed medulla
Trigeminal spinal nucleus-receives pain/temp info from face; fibers cross and ascend to VPL |
|
|

General
Identify Fxn |
Caudal/closed medulla
Accessory nucleus-gives rise to accesory nerve (trapezius, SCM) |
|
|
General
Identify Fxn |
Rostral/open medulla
Trigeminal spinal nucleus-receives pain/temp info from face; fibers cross and ascend to VPL |
|
|

General
Identify Fxn |
Rostral/open medulla
Medial lemniscus- fiber tract projecting from dorsal column nuclei to VPL (vertical orientation) |
|
|

General
Identify Fxn |
Rostral/open medulla
Dorsal nucleus of X- gives rise to parasympathetic neurons above transverse colon |
|
|

General
Identify Fxn |
Rostral/open medulla
Nucleus of solitary tract-reveives taste info from CN 7, and autonomic info from CN 9 and 10 (carotid/aortic bodies) |
|
|

General
Identify Fxn |
Rostral/open medulla
Corticospinal tract- carries axons from motor cortex which go to innervate motor neurons in ventral horn- allows muscle movement |
|
|

General
Identify Fxn |
Rostral/open medulla
Inferior olivar nucleus- info to cerebellum, coordinated movement |
|
|

General
Identify Fxn |
Rostral/open medulla
Medial lemniscus- fiber tract projecting from dorsal column nuclei to VPL (vertical orientation) |
|
|

General
Identify Fxn |
Caudal pons
Medial lemniscus- fiber tract projecting from dorsal column nuclei to VPL (starts horizontal orientation) |
|
|

General
Identify Fxn |
Caudal pons
Facial nucleus- gives rise to facial nerve 7, innervates muscle of the face |
|
|

General
Identify Fxn |
Rostral pons
Medial lemniscus- fiber tract projecting from dorsal column nuclei to VPL (starts horizontal orientation) |
|
|
General
Identify Fxn |
Rostral pons
Trigeminal motor mucleus- innervates muscles of mastication |
|
|

General
Identify Fxn |
Rostral pons
Trigeminal principal mucleus- receives touch info from the face, projects bilaterall to VPM, duplicating sensory info so lesion doesn’t knock out both sides |
|
|

General
Identify Fxn |
Caudal midbrain
Substantia nigra- dopamine cells, loss= parkinson’s disease |
|
|

General
Identify Fxn |
Caudal midbrain
Ceerebral peduncle= continuation of corticospinal tract (motor neurons) |
|
|
|
General
Identify Fxn |
Caudal midbrain
Periaqueductal gray- surround cerebral aqueduct, modulates sensitivity to pain |
|
|

General
Identify Fxn |
Caudal midbrain
Periaqueductal gray- surround cerebral aqueduct, modulates sensitivity to pain |
|
|

General
Identify Fxn |
rostral midbrain
Periaqueductal gray- surround cerebral aqueduct, modulates sensitivity to pain |
|
|

General
Identify Fxn |
rostral midbrain
Cerebral peduncle= continuation of corticospinal tract (motor neurons) |
|
|

General
Identify Fxn |
rostral midbrain
Substantia nigra- dopamine cells, loss= parkinson’s disease |
|
|

Identify, fxn
|
Corpus callosum
White matter tract allowing cross-talk between the two brain hemispheres. |
|
|

Identify, fxn
|
Caudate- basal ganglia, motor control,
|
|
|

Identify, fxn
|
putamen- basal ganglia, motor control,
|
|
|

Identify, fxn
|
Nucleus accumbens- reward system
|
|
|

Identify, fxn
|
Globus pallidus-basal ganglia, motor control, lots of myelinated axons
|
|
|
Identify, fxn
|
Internal capusle-in/output, carries corticospinal tract
|
|
|

Identify, fxn
|
Anterior commisure- minor communication btwn brian hemispheres
|
|
|

Identify, fxn
|
Amygdala-emotion
|
|
|

Identify, fxn
|
Thalamus- 3 nuclei that releay sensory info to cortex
|
|
|

Identify, fxn
|
Cerebral peduncle- continuation of internal capsule, carries corticospinal tract
|
|
|
|
Identify, fxn
|
Substantia nigra- contains dopamine releasing cells
|
|
|

Identify, fxn
|
Substantia nigra- contains dopamine releasing cells
|
|
|

Identify , fxn
|
Red nucleus-works w/ cerebellum for motor coordination
|
|
|

Identify, fxn
|
Hippocampus-learning and memory
|
|
|

Identify, fxn
|
Parahippocampal gyri
|
|
|

Identify
|
putamen
|
|
|

Identify
|
Caudate nucleus
|
|
|

Identify
|
thalamus
|
|
|

Identify, fxn
|
Chroid plexus- generates CSF
|
|
|

Identify, fxn
|
Calcarine sulcus- home to primary visual cortex
|
|