![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
31 Cards in this Set
- Front
- Back
|
How does kidney disease affect drug absorption? |
Fluid retention in kidney disease with oedema of the bowel wall can lead to reduced absorption of drugs given orally
↓ due to vomiting |
|
|
How does kidney disease affect drug distribution? |
Hypoalbunimaemia? → protein binding of drugs may be affected → ↑ drug plasma conc.
Uraemia? → retained substances compete for binding sites with drugs (ask dad) → ↑ drug plasma conc. Fluid retention? → ↑ vol. of distribution |
|
|
How does kidney disease affect drug elimination and metabolism? |
Generally if metabolism/elimination is impaired → ↑ drug half-life and drug plasma conc. e.g. ↓ renal insulin metabolism → hypoglycaemia > Uraemia alters hepatic drug metabolism
> Renal elimination is important for water-soluble drugs - minimally hepatic metabolism |
|
|
Which drugs should be avoided in kidney disease? |
Drugs containing nitrogen, sodium, potassium and magnesium:
Penicillin and blood transfusions - potassium
Many antacids contain sodium and magnesium Soluble paracetamol - sodium |
|
|
Describe normal drug elimination in the kidneys. |
• Most drugs unless highly plasma protein bound freely filtered
• Most drugs esp. weak acids actively secreted into proximal tubule
• Lipid soluble drugs passively reabsorbed by diffusion across tubule - not much excreted in urine
• Weak acids more easily excreted in alkaline urine and vice versa |
|
|
Give examples of drugs where their elimination is significantly affected by loss of normal kidney function. |

Drugs like vancomycin and gentamicin are almost comletely excreted by the kidney
The kidneys are not involved in rifampicin excretion at all (all hepatic metabolism) (anuria = 0 kidney function) |
|
|
How do you account for decreased elimination of a drug such as vancomycin? |
• Modify dose - simply ↓ the dose • Loading dose - same loading dose but less frequently
• Monitoring - alter dose according to drug concentrations |
|
|
What factors alter kidney function. |
• Age - very young or old • Renal disease e.g. diabetes
• Renal damage |
|
|
What formula is used to calculate GFR for prescribing? |
Cockcroft-Gault formula (based on CrCl) |
|
|
Describe dose adjustment for renal impairment. |
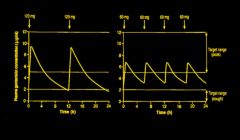
• ↓ dose → ↓ peak concentration
• ↓ dose interval → ↑ trough concentration
• Both → more uniform serum concentration |
|
|
Describe how drug protein binding is affected by renal impairment. |
Phenytoin - 90% bound to albumin
Only 10% is “free” and therapeutically active Hypoalbuninaemia → plasma levels too high → toxicity |
|
|
Give examples of drugs which have an altered sensitivity due to renal impairment. |
• Increased sensitivity > CNS depressants e.g. opioids → accumulation of metabolites + ↑ sensitivity → narcosis (reversed by naloxone) > antihypertensives • Reduced sensitivity > diuretics > urinary antibacterials |
|
|
Give examples of drugs that have reduced elimination in renal impairment. |
Aminoglycosides - gentamicin, vancomycin
Digoxin
Aciclovir |
|
|
When is dose adjustment needed for renal impairment?
Give examples of drugs that need dose adjustment in renal impairment. |
• Drug with at least 50% renal clearance • Drug with low therapeutic index
e.g. digoxin, aminoglycosides, metformin, ACE inhibitors, MTX |
|
|
What factors need to be considered when considering dose adjustment for renal failure? |
• Extent of renal impairment
• Extent of renal elimination
• Concentration-dependent toxicity
• Therapeutic index |
|
|
Why is the kidney particularly vulnerable to the toxic effects of drugs? |
Large blood flow
Drugs become concentrated in the renal medulla
and further concentrated in tubular cells |
|
|
Which drugs tend to cause acute tubular necrosis? |
Aminoglycosides
|
|
|
Which drugs tend to cause glomerulonephropathies? |
Gold salts
NSAIDs |
|
|
Which drugs tend to cause interstitial nephritis? |
Usually hypersensitivity reaction in acute interstitial nephritis
Antibiotics derived from penicillin
Allopurinol |
|
|
How do NSAIDs alter kidney physiology? |
Blood flow through kidney arterioles is maintained by vasodilator prostaglandins - NSAIDs inhibits COX → ↓ prostaglandins → ↓ renal blood flow and GFR |
|
|
What are adverse effects of NSAIDs on the kidney? |
Chronic use causes: > AKI due to ischaemia - don't give to CKD patients > Sodium retention (in body fluids - not hypernatraemia) - worsens oedema and HTN |
|
|
When can ACE inhibitors cause renal impairment and why does this happen? |
• Bilateral renal artery stenosis • Co-administered with NSAIDs or large volume diuretics • When dehydrated or septic Because of their mechanism of action (constriction of the efferent arteriole → maintains intraglomerular pressure) |
|
|
Describe the mechanism of action of the major types of diuretics. |
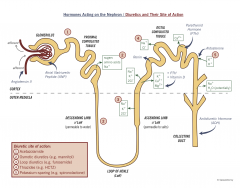
Loop diuretics block NKCC in TAL
Thiazide diuretics block NCC in cortical diluting segment of DT K⁺ sparing diuretics interfere with aldosterone action (dependent on type) in DT and CD |
|
|
Give examples of each of the major types of diuretic. |
Loop - Furosemide, Bumetanide Thiazide - Bendrofluazide K⁺ sparing - Spironolactone, Amiloride |
|
|
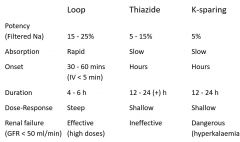
Describe the different pharmacologic properties of the major diuretic classes. |
|
|
|
Describe the differing mechanisms of action of Spironolactone and Amiloride. |
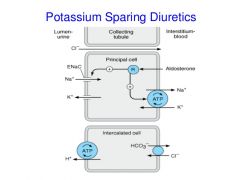
• Spironolactone - mineralocorticoid receptor antagonist • Amiloride – blocks ENaC in CD |
|
|
What are the general side effects of thiazide and loop diuretics? |
1) NON-SPECIFIC > GI upset (nausea, vomiting) > hypersensitivity reactions - skin rash, thrombocytopenia 2) METABOLIC EFFECTS > hypokalaemia, hyponatraemia > hypovolaemia → hypotension > urate retention → gout (rare) > exacerbate glucose intolerance |
|
|
What problems can you get as a result of hyperkalaemia and hypokalaemia? |
Both: Cardiac arrythmias Muscle weakness |
|
|
What are the specific adverse effects of loop diuretics? |
Ototoxicity (high doses) → deafness, NKCC found in ear Metabolic alkalosis |
|
|
Describe the adverse effects of lithium (antipsychotic) on the kidney. |
Long-term therapy - reabsorbed by cells in CD and inhibits the action of ADH → can cause nephrogenic diabetes insipidus |
|
|
Describe how trimethoprim (antibiotic) affects kidney function. |
causes ↑ serum creatinine which is interpreted as ↓ in eGFR - not a true ↓ in GFR |