![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
63 Cards in this Set
- Front
- Back
|
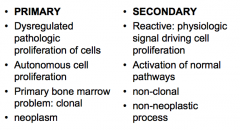
approach to increased cell count: primary vs secondary (4 points) |
|
|
|
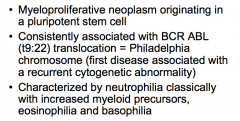
def'n of myeloproliferative neoplasm? |
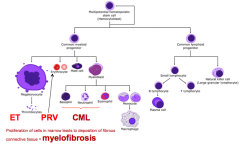
= too many mature myeloid cells |
|
|
note: myelofibrosis leads to extramedullary production in spleen, liver, LN's... |
d |
|
|
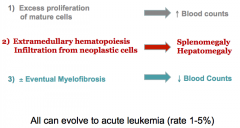
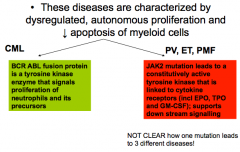
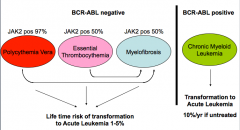
myeloproliferative neoplasms (MPN) pathophys? 3 and risk of transformation to... |
|
|
|
note: different ways to classify MPN... |
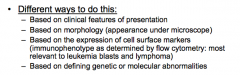
current disease classification based on molecular understanding of disease.. but clinical features stlil important |
|
|
significance of 1. BCR ABL mutation 2. JAK 2 mutation |
|
|
|
note MPN's that fall into each of the following categories 1. BCR-ABL negative vs. BCR-ABL positive 2. JAK2 pos vs. JAK2 indeterminate |
|
|
|
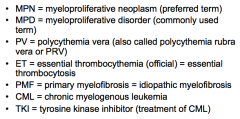
term glossary.. |
|
|
|
•60 yo man from the Middle East. Works as amechanic. He has hypertension and TypeII diabetes. His BMI is >30. He has a 40 pack year smoking history. He has been having intermittentheadaches. Tells me that his brothersometimes has blood “taken off” for this. He has a CBCd done. |
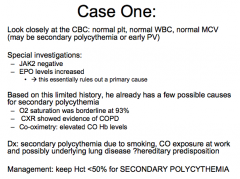
CBC shows isolated polycythemia |
|
|
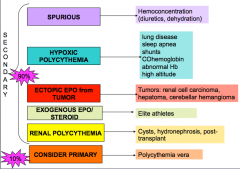
DDx of polycythemia 5 secondary 1 primary NB |
|
|
|
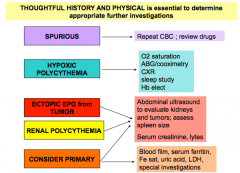
NB: investigations and workup of polycythemia |
|
|
|
NB: signs and Sx of PV 6 |
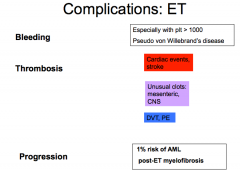
1. head: fullness, headaches, conjunctival injection 2. splenomegaly: early satiety 3. Erythromelalgia: burning, painful extrem 4. Joints: gout 5. Skin: pruritis that is worse after shower 6. Thrombosis (cardiac events, stroke, DVT, PE, unusual clots (mesenteric and CNS) note that weird clots are a red flag.. |
|
|
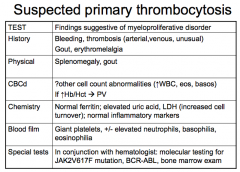
Investigations of suspected primary PV: History Physical CBC (2) Chemistry Blood Film Special tests |
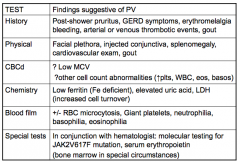
notes: dyspepsia from too much histamine --> hyperacidic microcytic as they tend to run out of building blocks in PV.. |
|
|
3 special tests in PV and the utility |
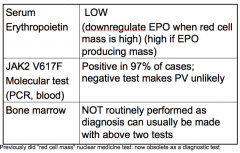
note: would expect EPO to be high if exogenous or ectopic production.. |
|
|
back to first case... what is his Dx and management |
|
|
|
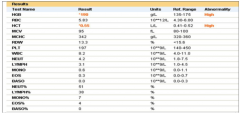
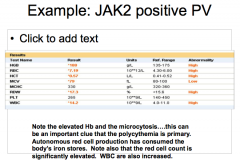
Example CBC of patient with JAK2 positive PV |
|
|
|
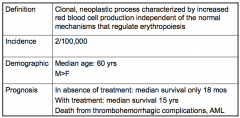
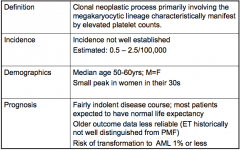
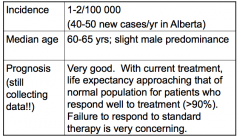
summary of polycythemia vera 1. definition 2. incidence 3. demographic 4. prognosis |
|
|
|
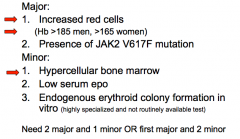
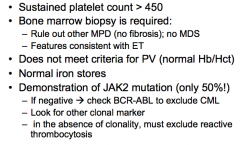
diagnostic criteria for PV 2 major 3 minor need 2 major and 1 minor OR first major and 2 minor |
|
|
|
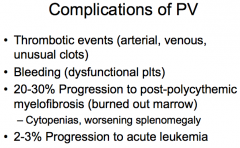
list complications of PV 4 |
|
|
|
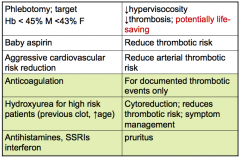
PV therapy 3 routine, 3 high risk/specific |
|
|
|
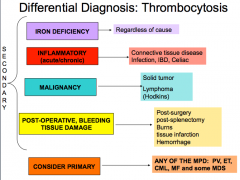
DDx of thrombocytosis (4 secondary, vs. primary causes 5) |
|
|
|
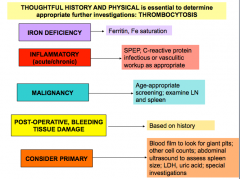
workup of thrombocytosis |
|
|
|
Suspected Primary Thrombocytosis: History Physical CBCd Chemistry Blood film Special Tests |
|
|
|
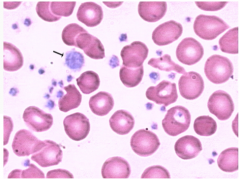
Thrombocytosis with giant platelets (arrow) Numerous platelets are noted in thepeipheralblood smear from a patient with CML. Giant platelets (arrow) are alsoappreciated.This is a giant platelet.. Andprobably too many pltfor this smear. |
|
|
Essential thrombocytopenia 1. definition 2. incidence 3. demographics 4. prognosis |
|
|
|
Diagnostic criteria for essential thrombocytosis note diagnoses to exclude... |
|
|
|
Complications of ET 1. bleeding? 2. thrombosis 3. risk of progression to... |
|
|
|
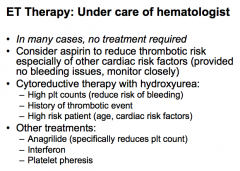
Tx of ET 1. tx to reduce thrombotic event.. 2. when to use cytoreductive therapy? 3. other tx? |
|
|
|
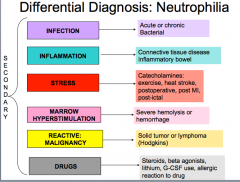
DDx of neutrophilia? 6 |
|
|
|
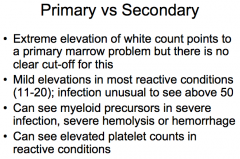
Primary MPD vs. 2ndary MPD |
|
|
|
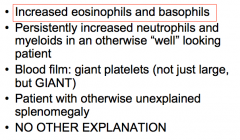
possible clues to a primary MPD CBC findings (2) Blood film Exam finding? |
|
|
|
Note: which MPDs have elevated neutrophil counts? |
all of them. PV, ET, MF, CML |
|
|
which MPD's have increased myeloads |
•Myeloidscan be seen in other MPD, but classically CML has the whole spectrum of myeloidprecursors (blasts, promyelocytes, myelocytes, metamyelocytes, bands, neuts) |
|
|
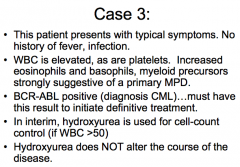
Early presentation of CML? CBC findings? |
•Early presentation of CML may not have asignificant component of myeloid precursors |
|
|
NB: if BCR ABL negative, which MPD is excluded |
CML |
|
|
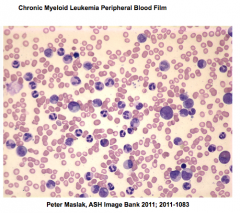
Peripheral blood smear shows granulocytosis withall stages of maturation. |
|
|
CML: 1. def'n 2. mutation 3. CBC findings |
|
|
|
CML: incidence, median age, prognosis |
|
|
|
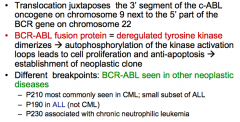
Philadelphia chromosome and the BCR ABL oncogene 1. def'n 2. result of the BCR ABL fusion protein |
|
|
|
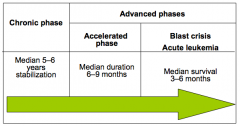
Natural History of CML 1. chronic phase (duration) 2. accelerated phase (duration) 3. Blast crisis (median survival) |
|
|
|
CML: % diagnosed in each stage? |
40% on routine lab tests and are asymptomatic 85-90% diagnosed in chronic phase 10-15% accelerated or blast phase |
|
|
typical Sx of CML |
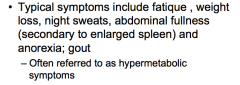
overall "hypermetabolic" |
|
|
Unusual presentations of CML... |
–Leukostasis: sluggish blood flow associatedwith very high wbc counts (>250)• |
|
|
CML: what is the treatment |
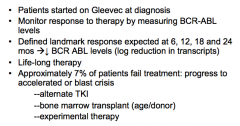
targeted therapy. very effective. Imatinib/Gleevac is a tyrosine kinase inhibitor. |
|
|
CML: treatment 1. how is response to therapy measured? 2. tracking the response? 3. do they ever stop the drug? 4. % of patients taht fail treatment? |
|
|
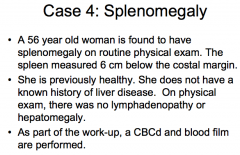
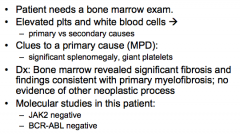
case 4 |
|
|
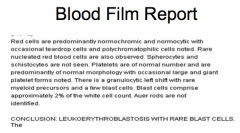
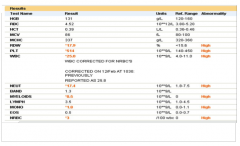
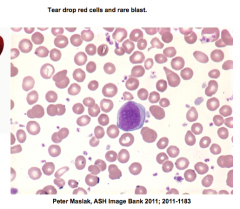
Case 4: blood film report |
this person needs a hematology consult |
|
|
Important findings in primary myelofibrosis (PMF) |
1. splenomegaly 2. Leucoerythroblastic blood film |
|
|
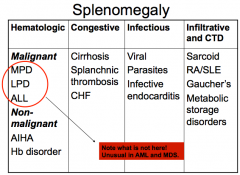
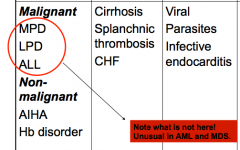
DDx of splenomegaly (4 big categories) |
|
|
|
hematologic causes of splenomegaly (SM) 1. malignant (3) 2. non malignant (2) |
|
|
|
congestive causes of SM 3 |
cirrhosis, splanchnic thrombosis CHF |
|
|
Infectious causes of SM 3 |
1. viral 2. parasite 3. Infective endocarditis |
|
|
Infiltrative cause of SM 4 |
1. sarcoid 2. RA/SLE 3. Gaucher's 4. metabolic storage disorders |
|
|
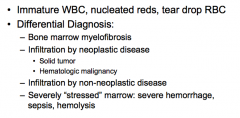
1. def'n of a leucoerythroblastic blood film 2. DDx 4 |
|
|
|
workup of case 4 .. |
|
|
|
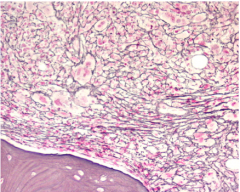
marrow fibrosis in primary myelofibrosis (reticulin stain) |
|
|
primary myelofibrosis def'n features phases (2) |
features: fibrosis, SM phases: proliferative and fibrotic |
|
|
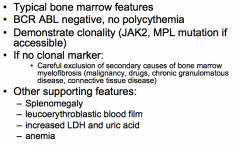
Diagnostic criteria for PMF 1. marrow features 2. genetic/molecular/CBC findings 3. diagnoses to exclude 4. other supporting features 4 |
|
|
|
Myelofibrosis 1. typical age? 2. prevalence |
1. older patient (60s-70s) 2. Least common of the MPD |
|
|
early and late presentation of MPD |
|
|
|
complications of Myelofibrosis (8) |
|
|
|
Prognosis Myelofibrosis? |
variable median survival is 5 years for patients who are anemic patients with normal cell counts have median survival up to 15 y |
|
|
Tx of Myelofibrosis |
|