![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
144 Cards in this Set
- Front
- Back
|
Which of the following regarding Antihypertensives/HTN is incorrect: 1. BP = CO x PVR 2. Endothelin constricts blood vessels 3. Inheritability of HTN is ~50% 4. With every increase in 20mmHg systolic - cardiovascular disease risk doubles 5. HTN is defined as BP > 140/90 |
3. Inheritability of HTN is ~50% - incorrect = 30% |
|
|
Effect of NO on blood vessels? |
Vasodilation |
|
|
What is the effect of activation of carotid (stretch) baroreceptors? |
Inhibition of central SNS output via the tractus solitarius |
|
|
What are the main classes of anti-hypertensives? |
1. Diuretics 2. Sympathoplegics 3. Direct Vasodilators 4. ACEI/ARBs |
|
|
Which of the following are incorrect: 1. Diuretics reduce BP by ~10-15mmHg 2. ACEI reduced BP by <10mmHg 3. Clonidine MOA is Alpha 2 agonist - central inhibition of SNS 4. Methyldopa is a centrally acting antihypertensive used in pregnancy 5. Prazocin is also an alpha agonist |
5. Prazocin is also an alpha agonist - incorrect - alpha1 blocker |
|
|
Name the centrally acting sympathoplegic antihypertensives? |
Clonidine - alpha 2 partial agonist - binds to receptors in the medulla to decrease SNS and increase PSNS outflow Methyldopa |
|
|
ADRs clonidine? |
Dry mouth Sedation Depression Rapid withdrawal can cause a life threatening hypertensive crisis |
|
|
How do BB mediate their antihypertensive effects? |
1. B1 - heart - negatively chronotropic and negatively inotropic - reduced CO 2. Decrease peripheral resistance - presynaptic Beta receptors to reduce SNS vasoconstrictor activity 3. B1 - inhibit renin secretion |
|
|
ADRs Beta blockers |
Bradycardia Asthma - exacerbation Worsen PVD and diabetes (b2 blockade of insulin secretion) Withdrawal - tachycardia, nervousness, angina fatigue, insomnia, unpleasant dreams impaired exercise tolerance erectile dysfunction |
|
|
Metoprolol acts on what receptors> |
B1 selective |
|
|
Atenolol acts on which receptors |
B1 selective |
|
|
B1 selective beta blockers |
Metoprolol Atenolol Bisoprolol Nebivolol |
|
|
Non- selective beta blockers |
Propanolol - beta 1/2 |
|
|
Beta/alpha blockers |
Labetalol B>A Carvedilol B=A |
|
|
Difference between nebivolol and other B1 selective beta blockers? |
The D isomer has vasodilating properties that are not alpha mediated --> possibly due to increased endothelial NO release via induction of endothelial nitric oxide synthase |
|
|
Metabolism of bisoprolol |
Liver |
|
|
Metabolism of bisoprolol |
Liver |
|
|
Metabolism of metoprolol |
CYP2D6
Also metabolises opioids including Codiene, antipsychotics, SSRIs, TCAs, class 1 antiarrhythmics |
|
|
Metabolism of bisoprolol |
Liver cyp2d6 |
|
|
Mechanism of action of ESMOLOL? |
beta 1 selective beta blocker
Short half life due to hydrolysis by plasma esterases
Requires constant IV infusion |
|
|
MOA of prazosin? |
Alpha 1 blocker - reduce dilating in both capacitance and resistance vessels
By being selective it prevents the reflex central alpha 2 mediated increase in SNS outflow |
|
|
MOA of prazosin? |
Alpha 1 blocker - reduce dilating in both capacitance and resistance vessels
By being selective it prevents the reflex central alpha 2 mediated increase in SNS outflow |
|
|
ADRs of prazosin |
Cause Na and water retention --> should be given with a diuretic and beta blocker (baroreceptor activation and SNS activation)
Beneficial in BPH
Dizziness, palpitations, headache
Reflex tachycardia |
|
|
Name common vasodilators and MOA |
Oral - HTN Hydralazine (increased NO) Minoxidil (opening K channels and hyperpolarization )
IV - hypertensive crisis Nitroprusside (increased NO)
Nitrates (angina)(increased NO) + calcium channel blockers (reduced Ca influx) |
|
|
Which vasodilators relax veins and arteries ? |
Nitroprusside Nitrates |
|
|
Side effects of beta blockers |
dizziness tiredness blurred vision cold hands and feet slow heartbeat diarrhoea and nausea
insomnia (sleep disturbance) loss of libido (sex drive) depression impotence |
|
|
Which vasodilators increase NO ? |
Nitroprusside Hydralazine Nitrates |
|
|
What is the problem with Hydralazine as an antihypertensive? |
Tachyphylaxis
Rapid tolerance to antihypertensive effects
But good in combination esp nitrates in heart failure |
|
|
Metabolism of Hydralazine ?
ADRs? |
Metabolism- Liver
ADRs - headache, nausea, anorexia, palpitations, sweating, flushing
Reflex tachycardia + SNS effects
Peripheral neuropathy + lupus + renal impairment |
|
|
MOA of minoxidil? |
Opening of k channels and hyperpolarization of smooth muscle - relaxation and peripheral vasodilation (arterioles)
Associated with reflex SNS stimulation and Na/water retention |
|
|
MOA of minoxidil? |
Opening of k channels and hyperpolarization of smooth muscle - relaxation and peripheral vasodilation (arterioles)
Associated with reflex SNS stimulation and Na/water retention |
|
|
ADRs of minoxidil ? |
Tachycardia, palpitations, angina, oedema
Headaches, sweating,
hypertrichosis --> topical ROGAINE |
|
|
MOA of nitroprusside?
Indications ? |
Arterial and vein dilator -- reduces venous return and after load
Increased NO --> Activation of guanylyl cyclase --> increased cGMP --> relaxes smooth muscle
Indications - hypertensive emergencies and severe heart failure |
|
|
Toxicity of Nitroprusside? |
Accumulation of course cyanide, metabolic acidosis, arrhythmias, excessive hypotension
This tante toxicity = weakness, disorientation, psychosis, muscle spasms, convulsions |
|
|
Dihydropyridines?
Effects? |
Nifedipine, lercardipine, felodipine, nimodipine
Selective vasodilators with minimal cardiac depressant effects |
|
|
Dihydropyridines?
Effects? |
Nifedipine, lercardipine, felodipine, nimodipine
Selective vasodilators with minimal cardiac depressant effects |
|
|
The strongest cardiac depressant CCB ? |
Verapamil >> diltiazem >>>> dihydropyridine |
|
|
Function of ACE? |
1. Hydrolyses ATI --> ATII --> vasoconstriction + aldosterone secretion 2. Inactivate bradykinin --> which usually increases prostaglandins, causes vasodilation, decreased PVR, decreased BP |
|
|
ACEI used in autonomic dysreflexia? |
captopril IV |
|
|
How do ACEI reduce HTN? Other benefits? |
Mainly by reducing TPR but unlike vasodilators - do not activate SNS responses - good for renal (stabilise diabetic nephropathy), good for heart failure and AMI |
|
|
Elimination of ACEI? |
Mainly RENAL - all the ones we use in aus |
|
|
ADRS of ACEI |
Severe hypotension - in those who are hypovolaemic Acute renal failure Hyperkalaemia Dry cough Angioedema Altered tast, rash, drug fever CI - Pregnancy - 2/3rd trimesters - fetal hypotension, anuria and renal failure, 1st - ?teratogen? |
|
|
What are some drugs that cause HTN? |
OCP Sympathomimetic decongestants NSAIDs Herbal meds - some |
|
|
What are non-pharmacological methods of reducing BP? |
Weight loss - will normalise BP in 75% of those who are overweight with mild-moderate HTN Na restriction 70-100meq/day |
|
|
T/F As Thiazides adversely affect the lipid profile and glucose tolerance - they are thought to be worse at reducing CV risk. |
Incorrect - large clinical trial demonstrated that CHLORTHLIDONE was as effective at reducing IHD and AMI than other first line agents. and superior than amlodipine at reducing heart failure and superior to lisinopril in preventing stroke. |
|
|
What is the most common cause of hypertensive emergencies? |
Someone with chronic hypertension who suddenly stops taking his/her medications |
|
|
Examples of hypertensive emergencies? |
HTN associated with: - vascular damage - malignant htn - haemodynamic changes - heart failure, stroke, aortic dissection - Encephalopathy - severe headache, mental confusion, blurred vision, N/V, focal neuro --> leads to convulsions, stupor, coma and death |
|
|
Which of the following are correct? 1. Glucose is the favoured energy substrate for the myocardium 2. O2 requirement increases with increased HR, contractility, afterload or ventricular volume. 3. Prinzmetal angina can be reversed with CCB and nitrates 4. Unstable angina is - angina at rest or increase in frequency/intensity/duration in a person with previous angina 5. Prinzmetal angina can be cause significant myocardial ischemia |
1. Glucose is the favoured energy substrate for the myocardium - incorrect - fatty acids |
|
|
Which of the following are not a determinant of myocardial oxygen consumption? Wall stress - intraventricular pressure, ventricular radius (volume), wall thickness Dromotropy Heart rate Contractility |
Dromotropy |
|
|
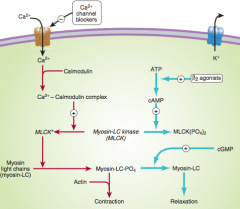
Which of the following are incorrect? 1. Nitroprusside is a vasodilator that acts via increasing NO --> guanylyl cyclase --> increase cGMP --> dephosphorylation of MLC --> no myosin/actin interaction. 2. CCB reduce intracellular calcium and hence prevent activation of MLCK and phosphorylation of Myosin 3. Minoxidil works via membrane stabilisation via opening of K channels 4. cAMP increases vascular smooth muscle tone 5. Coronary blood flow is directly proportional to the perfusion pressure (Aortic systolic pressure) and the duration of systole |
4. cAMP increases vascular smooth muscle tone - incorrect --> causes inactivation of MLCK and relaxation 5. Coronary blood flow is directly proportional to the perfusion pressure (Aortic systolic pressure) - incorrect -- DIASTOLIC PRESSURE and duration of DIASTOLE |
|
|
Which of the following are incorrect: 1. The limiting factor for coronary perfusion during tachycardia is the duration of diastole 2. Increasing cGMP inhibits vascular SM contraction 3. B2 agonists cause vasodilation via increasing cAMP and are commonly used for this purpose in angina 4. Most pathways inhibiting SM contraction end up affecting MLCK in some way |
3. B2 agonists cause vasodilation via increasing cAMP and are commonly used for this purpose in angina - incorrect - correct MOA but UNCOMMONLY used due to cardiac stimulation via B1 |
|
|
MOA of Nitrates and nitroprusside |
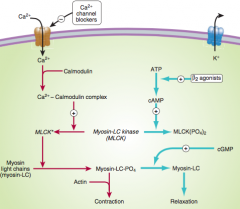
vasodilators that acts via increasing NO --> activating guanylyl cyclase --> increase cGMP --> dephosphorylation of MLC --> prevents phosphorylation of myosin --> no myosin/actin interaction. |
|
|
MOA of Calcium channel blockers |
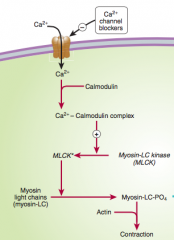
CCB reduce intracellular calcium This usually binds to calmodulin which then activates MLCK --> which causes phosphorylation of Myosin to allow Myosin/actin coupling This is thus preventing and SM relaxation occurs |
|
|
What are the 4 mechanisms of reducing vascular tone? |
1. Increasing cGMP - fascilitates dephosphorylation of MLC - nitrates 2. Decreasing intracellular Ca2+ - prevents activation of MLCK - CCB 3. Stabilising the membrane - ie opening K channels 4. Increasing cAMP - increases inactivation of MLCK - B2 agonists (not used for this purpose due to cardiac stimulation |
|
|
What is the role of MLCK in the contraction of smooth muscle? |
|
|
|
What are the 3 main groups of drugs used to treat angina? diuretics nitrates BB Vasodilators CCB |
CBB Nitrates BB These all act by decreasing oxygen demand of the myocardium by reducing HB, ventricular volume, BP, contractility |
|
|
Which of the following are incorrect regarding nitrates? 1. Inactivation is in the liver via nitrate reductase 2. Nitrates only vasodilate arteries 3. PO bioavailability is low due to high first pass metabolism ~ 10-20% 4. MOA is as a NO donor via an enzyme in endothelium ALDH2 --> results in increased cGMP 5. The preferred GTN route is SL |
2. Nitrates only vasodilate arteries - incorrect - all vascular smooth muscle including venous |
|
|
How to nitrates help reduce angina? |
Venous dilation - increased capacitance - reduced venous return - reduced preload - reduced stretch - reduced myocardial volume work Arterial dilation - reduced TPR - reduced afterload - reduced pressure work of the myocardium Vasodilate the epicardial coronary vessels (relax vasospasm) Both result in reduced oxygen demand |
|
|
ADRs of nitrates? |
Orthostatic hypotension - due to venous pooling Syncope Headache SNS - tachycardia and positive inotropy Na/water retention Reduced platelet aggregation Tachyphylaxis CI - raised ICP |
|
|
? which vitamin is used in cyanide poisoning? |
Vit B12 |
|
|
MOA of sildenafil |
Inhibits phsophodiesterase - which usually breaksdown cGMP Hence increase cGMP --> dephosphorylation of myosin light chains --> relaxation of SM --> filling of corpora cavenosa --> erection |
|
|
MOA of nicorandil |
NO donor and open K channels |
|
|
Verapamil blocks what type of calcium channels ? |
L type (long lasting type) Ca1.1-1.4 Found in cardiac, skeletal, smooth muscle, neurons, endocrine and bones Note limited effect on skeletal muscle as these use SR source of Ca and require little influx of Ca |
|
|
Which of the following regarding CCB are incorrect? 1. Block L type calcium channels 2. Have high first past effect and are highly metabolised 3. High plasma protein binding 4. Drugs block the channel via a binding site on the inside of the plasma membrane similar to LA and Na channels 5. The effects include SM relaxation, reduced contractility, decrease SA rate, reduced AV nodal conduction |
All correct |
|
|
Benefit of nimodipine? |
partially selective for cerebral vessels used in cerebral vasospasm common following SAH |
|
|
ADRs of CCB |
Cardiac - depression, bradycardia, AV block, Cardiac arrest, heart failure Short acting dihydropyridines increase AMI Minor - flushing, dizziness, nausea, constipation, peripheral oedema Can worsen acute heart failure |
|
|
Indications of CCB |
Dihydropyridines - HTN, Raynauds, angina Verapamil, diltiazem - angina, HTN, arrhythmias |
|
|
Which beta blockers are vasodilators? |
Carvedilol - alpha 1 effects nebivilol - via NO |
|
|
T/F BB are usually better than CCB in patients with stable angina with respect to symptomatic relief and long term outcomes. |
True |
|
|
Contraindication to beta blockers? |
Asthma severe bradycardia atrioventricular blockade tachybrady syndrome severe unstable left ventricular failure |
|
|
MOA of Ivabradine Use?> |
Na funny current blocker Reduces cardiac rate by inhibiting the hyperpolarisation - activated Na channel in the SA node Anti anginal |
|
|
Main risk factors for PVD? |
hyperlipidaemia HTN Obseity Smoking diabetes |
|
|
which of the following are incorrect: 1. 5 yr mortality of heart failure is 50% 2. |
b |
|
|
Agents that improve survival in heart failure? |
ACEI ARBs BB - selected Aldosterone antagonists Hydralazine + nitrate combo |
|
|
Name drugs commonly used in acute vs chronic heart failure |
ACUTE - Bipyridines (milrinone), natriuetic peptide CHRONIC - Aldosterone antagonists, ACEI, ARB, Glycosides BOTH - Diuretics, BB, vasodilators |
|
|
Calcium initiator for myocyte contraction is from ? |
Stimulator Ca from initial extracellular influx but main influx of Ca is from the SR via activation of the ryanodine receptors (Ca gated) |
|
|
MOA of digoxin? |
Inhibits Na/K ATPase This in turn increases the Na concentration within the cell and and inhibits the function of the Na/Ca exchanger which pumps Ca out of the cell into the ECF. Resulting in increased cytosolic Ca and increased cardiac contractility |
|
|
Causes of high output heart failure? |
hyperthyroidism, beri beri, anaemia, arteriovenous shunts, pagets, pregnancy |
|
|
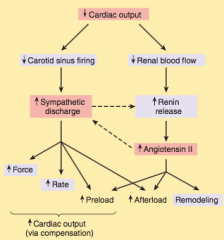
Normal compensation with low cardiac output |
|
|
|
Half life of digoxin? |
35-40 hrs |
|
|
MOA of milrinone? |
Phosphodiesterase 3 inhibitor PDE3
Increased cAMP - increased contractility and vasodilation
For acute heart failure Iv infusion |
|
|
Side effects of digoxin? |
Anorexia, nausea, vomiting, diarrhea
Junctional rhythms, bigeminy, second degree heart block, tachycardias and VF |
|
|
Selective beta 1 agonist? |
Dobutamine |
|
|
MOA and indication of bosentan? |
MOA- inhibitor of endothelin
Pulmonary hypertension |
|
|
MOA and indication of bosentan? |
MOA- inhibitor of endothelin
Pulmonary hypertension |
|
|
Beta blockers with mortality benefit in heart failure? |
Nebivolol Carvedilol Bisoprolol Metoprolol |
|
|
Therapy for patients with risk factors for heart failure? |
Risk factor modification Obesity, HTN, DM, lipids... |
|
|
Therapy for patients with risk factors for heart failure? |
Risk factor modification Obesity, HTN, DM, lipids... |
|
|
Management of NYHA class 1 heart failure ? |
Treat risk factors plus
ACEI/ARB Beta blocker Diuretic |
|
|
Management of NYHA class 2/3 heart failure ? |
Risk factors, ACEI, BB, diuretic
And Aldosterone antagonist, digoxin, CRT, Hydralazine + nitrate
CRT = cardiac resynchronisation therapy |
|
|
Therapy for patients with risk factors for heart failure? |
Risk factor modification Obesity, HTN, DM, lipids... |
|
|
Management of NYHA class 1 heart failure ? |
Treat risk factors plus
ACEI/ARB Beta blocker Diuretic |
|
|
Management of NYHA class 2/3 heart failure ? |
Risk factors, ACEI, BB, diuretic
And Aldosterone antagonist, digoxin, CRT, Hydralazine + nitrate
CRT = cardiac resynchronisation therapy |
|
|
Management of NYHA class 4 heart failure ?
Severe symptoms at rest |
Heart transplant or LVAD |
|
|
Indication for CRT |
Normal sinus rhythm with broad QRS - grade 2/3 heart failure
Improves mortality with left ventricular or biventeicular pacing |
|
|
Indication for digoxin? |
Af and heart failure |
|
|
Which of the following is incorrect: 1. 80% with an AMI will have an arrhythmia 2. 25% on digoxin will have an arrhythmia 3. AV nodal conduction is slow ~0.15s 4. Intracellular K = 10-15, ECF = 140mmol/L 5. Activation of the ventricles occurs in <0.1s |
4. Intracellular K = 10-15, ECF = 140mmol/L - incorrect - these values are true for Na not K K intracellular = 140, ECF = 4 mmol/L |
|
|
True/ false Increasing extracellular K levels reduces the membrane potential in myocytes and reduces AP duration. |
true This reduces the concentration gradient and reduces movement of K out of the cell -- ie + charge stays within and the cell becomes LESS negative |
|
|
Equation used to estimate membrane potential? |
Goldman-hodgkin-katz equation |
|
|
What is the effect of hyperkalaemia on pacemaker cardiac cells? |
SLOW or stop the pacemaker function - slow conduction, decrease pacemaker rate and decrease pacemaker arrhythmogenesis but in myocytes it acts to reduce the threshold to depolarisation and hence make then hyperexcitable. -- paradoxical effects where as hypokaelaemia leads to ectopic pacemakers |
|
|
Describe the effect of hypokalaemia in |
prolongedaction potential duration, increased pacemaker rate, andincreased pacemaker arrhythmogenesis. |
|
|
Which of the following are incorrect? 1. Hypokalaemia predisposes to torsades in patients taking sotalol and quinidine (K channel blocking agents) 2. VGSC are inactivated by the rapid closure of the h gate 3. There are different K channels in the SA node vs the myocyte/purkinje fibers 4. ACh increases the slope of phase 4 pacemaker potentials hence reducing pacemaker rate |
4. ACh increases the slope of phase 4 pacemaker potentials hence reducing pacemaker rate - incorrect --- decreases the slope |
|
|
Name the 2 main/broad mechanisms for the development of arrhythmias. |
1. Abnormal pacemaker activity / ectopic focus 2. Abnormal propagation - blockade or circuits |
|
|
Name the 4 main pharmacological methods for reducing arrhythmias. |
(1) sodium channel blockade, (2)blockade of sympathetic autonomic effects in the heart, (3) prolongation of the effective refractory period, and (4) calcium channel blockade. |
|
|
Describe the main classes of anti-arrhythmics with example. |
1. Class 1 - Na channel blockade --> subclasses: - 1A - Prolong AP duration - intermediate kinetics - procainamide + quinidine - 1B - Shorten AP duration - rapid kinetics - lignocaine - 1C - Minimal effects on APD but slow kinetics - flecanide 2. Class 2 - Sympatholytic --> reduce Beta adrenergic stimulation - beta blockers 3. Class 3 - Prolongation of AP duration --> blockade of the rapid component of the delayed rectifier - K current --> amiodarone, sotalol 4. Class 4 - Ca Current blockade --> slows conduction in SA and AV nodes -->Verapamil, diltiazem |
|
|
Which of the following are incorrect regarding anti-arrhythmics? 1. Amiodarone falls into all 4 classes but its main effect is class 3 2. Class 1C include lidocaine 3. Quinidine and procainamide are examples of class 1A 4. The only drugs affecting the Ca channel are verapamil and diltiazem 5. Class 1 drugs have local anaesthetic action and block Na channels |
2. Class 1c include lidocaine - incorrect lidocaine is class 1B 1C = flecanide 4. The only drugs affecting the Ca channel are verapamil and diltiazem - incorrect - also amiodarone, adenosine |
|
|
Which of the following are incorrect regarding amiodarone: 1. It has no effect on the QT interval 2. It causes Na channel blockage mainly in depolarised cells and causes Ca channel blockade 3. It increases refractory period in all cells 4. It inhibits pacemaker activity and is a sympatholytic agent 5. It is useful in both supraventricular and ventricular arrhythmias |
1. It has no effect on the QT interval - incorrect -- ++++ prolongation of QT |
|
|
Which of the following are incorrect regarding lidocaine? 1. It mainly affects blockade of Na channels in depolarised cells and increases the refractory period in depolarised cells 2. It inhibits pacemaker activity and is a sympatholytic agent 3. It blocks Na channels in activated and inactivated channels 4. It has a half life of ~1-2 hrs 5. It is very effective in supraventricular tachycardias in AMI |
2. It inhibits pacemaker activity and is a sympatholytic agent - incorrect - no sympatholytic activity 5. It is very effective in supraventricular tachycardias - incorrect - helpful in ventricular tachycardias only (in AMI) |
|
|
ADRS of lignocaine? |
Lidocaine is one of the least cardiotoxic sodium channel blockers. Proarrhythmic --> SA nodearrest, worsening of impaired conduction, and ventricular arrhyth-mias, uncommon. large doses --> hypotension. Most common --> are neurologic: paresthesias, tremor, nausea ofcentral origin, lightheadedness, hearing disturbances, slurred speech,seizuresI. |
|
|
Indications for lignocaine in cardiac conditions? |
Lidocaine is the agent of choice for termination of ventriculartachycardia in the setting of acute ischemia. |
|
|
MOA flecanide? Class? Indications? |
MOA - Class 1C anti-arrhythmic - Na channel blocker + K channel blocker Indication - Used for supraventricular tachycardias in patients with normal hearts. Good PO absorption, 20hr T1/2 |
|
|
Anti arrhythmic classes |
Some = Sodium channel blockers block = beta blockers potassium = prolongs the action potential via potassium or Na blockade channels = calcium blockers |
|
|
ADRs amiodarone |
symptomatic bradycardia + heart block in patients with pre-exisiting sinus or AV node disease Pulmonary fibrosis 1% hepatitis gray-blue skin Prolong QT - torsades photodermatitis visual halo optic neuritis Hypo/hyperthyroidism |
|
|
Metabolism of amiodarone |
CYP3A4 to inactive metabolite Induced by rifampicin ... reduced effect Inhibited by cimetidine ... increased effect |
|
|
Indications of amiodarone |
Low doses - AF Prevent recurrent ventricular tachycardia in combination with ICD to prevent recurrent defibrillation |
|
|
MOA of sotalol? Bioavailability, excretion, metabolism and half life |
Beta adrenergic - class 2 - L isomer AP prolonging effects - Class 3 - both L and D isomer Bioavailability 100% - excretion kidneys unchanged, no metabolism, T1/2 = 12h |
|
|
ADRs sotalol |
Dose related increase in torsade |
|
|
Indications for sotalol? |
AF Ventricular arrhythmias SVT in kids |
|
|
Indications for verapamil? |
Angina SVT - second line after adenosine in patients with NORMAL hearts (no heart failure, AV/SA node dysfunction) Rate control AF/flutter |
|
|
MOA of adenosine? |
Activation of K channel and inhibition of Ca channel Results in marked hyperpolarization and suppression of calcium-dependentaction potentials. When given as a bolus dose, adenosine directlyinhibits AV nodal conduction and increases the AV nodal refractory period but has lesser effects on the SA node |
|
|
Indication for adenosine |
SVT |
|
|
Function of Na channel blockade? |
slows conduction velocity and pacemaker rate |
|
|
Substances that promote platelet aggregation ? |
ADP TXA2 5HT Collagen vWF |
|
|
Initial binding of platelets is due to ? |
exposure of collagen and vWF |
|
|
Function of TXA2 in clotting? |
potent vasoconstrictor and platelet activator |
|
|
Which of the following are incorrect regarding clotting: 1. 5HT --> platelet activation and vasoconstriction 2. Platelet activation is via a confirmational change in IIb/IIIa receptor allowing for fibrinogen binding 3. White thrombi = platelet rich - in areas of high flow rate and high shear forces - ie arteries 4. Thrombin (IIa) cleaves fibrinogen to fibrin 5. Thrombin activates protein C |
2. Platelet activation is via a confirmational change in IIb/IIIa receptor allowing for fibrinogen binding --> incorrect order Platelet activation from ADP, TXA2, 5HT --> leads to conformational change |
|
|
Clotting cascade targets of: Warfarin Heparin |
Warfarin - 2 (thrombin), 7, 9, 10, protein C/S - prevents synthesis via blocking vitamin K Heparin - Xa + IIa |
|
|
Which of the following are incorrect: 1. Haemophila A - IX, Haemophila B - VIII 2. Plasmin is a protease that degrades fibrin, which is activated by t-PA 3. Indirect thrombin inhibitors include heparin, LMWH, fondaparinux 4. Indirect thrombin inhibitors work via potentiation of anti-thrombin effects, which inhibits thrombin (IIa), IXa + Xa 5. LMWH works via anti-thrombin but is more specific for Factor Xa than thrombin |
1. Haemophila A - IX, Haemophila B - VIII - incorrect - the other way around |
|
|
Which of the following are incorrect? 1. Heparin is monitored via aPTT levels, where as LMWH does not usually require monitoring 2. Measuring of LMWH can be done via anti-Xa units 3. The most common complication of HITS is arterial thrombosis 4. Warfarin may cause skin necrosis 5. HITS is relatively uncommon in pregnant females and is less with LMWH vs UFH |
3. The most common complication of HITS is arterial thrombosis - incorrect - most common is venous thrombosis but occlusion of arteries does occur |
|
|
ADRs of heparin use? |
Haemorrhage - increased in elderly women and renal failure Long term use - osteoporosis and fractures Reversible alopecia Allergies HITS - 1-4% >7day Rx |
|
|
Contraindications of heparin? |
Active bleeding HITS Allergy Haemophilia Significant thrombocytopaenia Purpura severe HTN ICH IE Active TB Ulcers of GIT Threatened abortion Visceral carcinoma Advanced hepatic or renal disease |
|
|
Which of the following are incorrect? 1. Dabigatran is an indirect thrombin inhibitor 2. Reversal of heparin is via protamine 3. Rivaroxaban and apixaban are a PO direct Xa inhibitor 4. Rivaroxaban does not require monitoring 5. Direct thrombin inhibitors include lepirudin and bivalirudin |
1. Dabigatran is an indirect thrombin inhibitor - incorrect - it is an oral direct thrombin inhibitor with predictable effects. Does not require monitoring |
|
|
MOA dabigatran? T1/2 Excretion? Indication |
Po direct thrombin inhibitor T1/2 12-17 hrs Excretion - renal No monitoring --> used for non-valvular AF |
|
|
Benefits of Xa and IIa inhibitors over warfarin? |
1. No monitoring 2. Not affected by diet and many drugs like warfarin 3. Warfarin - narrow therapeutic window Although - NO reversal - yet |
|
|
Which of the following are incorrect regarding warfarin: 1. Long half life 36 hrs 2. High protein binding and hence low Vd 3. Good PO bioavailability ~100% 4. Works well in most situations including cancer induced thrombosis 5. Teratogen |
4. Works well in most situations including cancer induced thrombosis - incorrect - this may be one of the most common reasons for warfarin resistance - advanced cancer - especially GIT |
|
|
Which of the following is incorrect regarding warfarin? 1. Amiodarone, cimetidine, disulfram and metronidazole increase the PT 2. Vit K and rifampin increase the PT 3. Aspirin, cephalosporins and heparin increase the PT 4. Hyperthyroidism augments warfarin action 5. Reversal is via Vit K, FFP, prothrombin complex |
2. Vit K and rifampin increase the PT - incorrect - decrease the PT - rifampin induces metabolism to inactive form |
|
|
Indications for thrombolysis? |
AMI PE with haemodynamic instability Severe DVT - ie SVC blockage Ascending thrombophlebitis with severe LL oedema CVA Peripheral vascular disease - intra-arterial |
|
|
MOA aspirin |
irreversible acetylation of COX thus reduced TXA2 reduced plt aggregation |
|
|
MOA clopidogrel? other drugs using this mechanism? |
Irreversibly inhibit ADP receptor on platelets Ticlopidine, prasugrel |
|
|
Which of the following are incorrect regarding antiplatelet agents? 1. Ticlopidine is associated with Leukopaenia 1% + TTP 2. The effect of clopidogrel is generally equal between patient subgroups 3. With 300mg of clopidogrel 80% of platelet function will be inhibited within 5hrs 4. Effects are usually 7-10 days in duration 5. Clopidogrel is a prodrug requiring activation via CYP2C19 |
2. The effect of clopidogrel is generally equal between patient subgroups - incorrect - due to the requirement of activation - a subset of the population have a mutation in the CYP2C19 and are poor metabolisers and have reduced antiplatelet action |
|
|
Metabolism of clopidogrel? |
ACTIVATION via CYP2C19 Prodrug CYP2C19 is inhibited by omeprazole ... use with caution |
|
|
Prasugrel is more effective in IHD/AMI than clopidogrel. Given this information what has stopped it surpassing clopidogrel as a mainstay of antiplatelet therapy? |
Increased bleeding in comparison CI - TIA and stroke due to bleeding risk It is also good because there is no prodrug /CYP dependence for activation with prasugrel |
|
|
MOA abciximab ? Indication? |
Chimeric monoclonal antibodies to IIb/IIIa complex on platelets Indication - used in PCI |
|
|
MOA dipyridamole? Indication |
Vasodilator that also inhibit platelet function via inhibiting adenosine uptake and cGMP phosphodiesterase activity Only helpful when in combination with aspirin (ASASANTIN) Mainly for TIA/CVA - secondary prevention |