Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
66 Cards in this Set
- Front
- Back
|
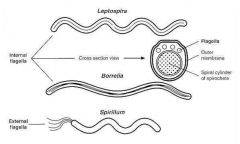
Describe leptospira
|
fine spiral bacteria of 0.2um in diameter by 6-20um length
Caused by spirochetes of the genus, Leptospira Spirochete, free-living Features of both gram + and gram – bacteria Total genome size: 4.8 Mb No plasmids Spiral, motile, obligate aerobes 6-20 um x 0.1-0.2 um |
|
|
Who gets leptospirosis?
|
Acute zooanthroponosis caused by pathogenic spirochetes of the genus Leptospira
Primarily a disease of mammals, but humans are infected occasionally through direct or indirect contact with animals A zoonotic disease with highly varied manifestations Most mammals are susceptible to infection |
|
|
clinical manifestations of leptospirosis
|
Clinical manifestations go from none to a severe, even lethal disease characterized by vasculitis, with pulmonary, hepatic, renal, and hemorrhagic manifestations
|
|
|
How is leptospira transfered
|
Infected mammals shed leptospires into urine for prolonged periods of time
A disease of the environment |
|
|
How is it lepto grown in the lab?
|
Grown in specialized culture medium- EMJH, Fletcher’s, Korthoff
|
|
|
How do you see leptospira?
|
Visualized by darkfield or phase contrast microscopy
|
|
|
Name the etiological agents of lepto
|
2 species
L. interrogans and L. biflexa Spiral, motile, obligate aerobes 6-20 m x 0.1-0.2 m > 210 serovars 23 serogroups Complex taxonomy Serovars not related to virulence |
|
|
Leptospira interrogans - describe it's microbiology
|
Flexible
Finelly coiled Gram - 6-12 m long 0.1 m wide Motile Aerobic LPS |
|
describe leptospira
|
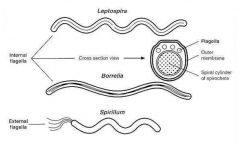
Thin, coiled, gram (-), aerobic, 6-20m long
Motile with hooked ends and paired axial flagella |
|
|
Taxonomy of Leptosiraceae
|
Order: Spirochaetales
Genus: Leptospira Classic taxonomy Basic taxon is serovar Single non-pathogenic species: L. biflexa Single pathogenic species: L. interrogans More than 25- pathogenic serovars within one species |
|
|
Typical reservoir hosts of common leptospiral serovars
|
Pigs -Pomona and Tarassovi
Cattle -Hardjo and Pomona Horses -Bratislava Dogs -Canicola Sheep- Hardjo Racoon- Grippotyphosa Rats - Icterohaemorrhagiae and Copenhageni - Largest Reservoir!! Mice - Ballum, Arborea and Bim Marsupials - Grippotyphosa Bats - Cynopteri and Wolffi |
|
|
Risk Factors for Leptospirosis
|
Occupational:
Farmers Abattoir workers Trappers Veterinarians Sewer Workers Rice field workers Military personnel Recreational: Freshwater swimming Canoeing, kayaking Household: Pets (dogs, rodents, hedgehogs …) Domesticated livestock Rainwater catchment Urban environment Domiciliary rodent infestation |
|
|
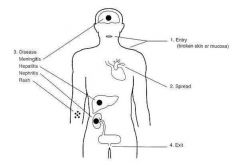
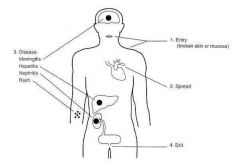
1) Entry - possible injestion
2) Spread - Rapid after entering lymphatics and blood stream 3) Disease - Tissue tropism not demonstraded Invasion facilitated by flagella and release of hyaluronidase |
|
|
Clinical presentations
|
Asymptomatic 5-15 %
Anicteric 90-95 % Weil syndrome - 5-10% |
|
|
Incubation period
|
Incubation 2-30 days
|
|
|
What is Weil Syndrome?
|
The disease was first described by Adolf Weil in 1886 when he reported an "acute infectious disease with enlargement of spleen, jaundice and nephritis".
|
|
|
Anicteric leptospirosis (Fort Bragg fever)
|
Fort Bragg fever
Anicteric leptospirosis, which is more common in children, and characterized by an abrupt 'toxic' state, with fever, shaking chills, headache, N&V and severe myalgias–especially of the legs, lethargy, dehydration, photophobia, orbital pain, generalized lymphadenopathy, and hepatosplenomegaly |
|
|
Icteric leptospirosis (Weil's syndrome)
|
Weil’s syndrome was characterized by intense jaundice, acute renal failure, skin ecchymoses and conjunctival suffusion, in addition to meningitis
|
|
|
Aseptic meningitis
|
fever, HA, sore throat, malaise, nausea, vomiting, stiff neck, nucal rigidity, acute confusion, paresis, transient paralysis
|
|
|
Epidemiology
|
Worldwide Tropics
Occupational disease -Garbage collectors -Butchers -Farm workers -Children -Domestic employees -Animal handlers Recreational risk in young male adults Rainy season, flooding, sewage |
|

What is this?
|
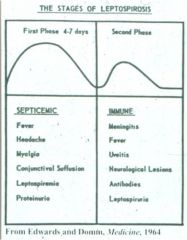
stages of lepto
|
|
|
Pathogenesis
|
Penetration through skin and mucosas; possibly by ingestion
Studies in mice suggest that capillary leak and hemorrhage result from LPS mediated disruption of vessel wall via intercallation of glycoprotein toxin |
|
|
Pathogenesis - first week
|
First week
Leptospira in blood and CSF Blood vessels, liver, kidney, muscles and lungs are affected early |
|
|
Pathogenesis
|
Penetration through skin and mucosas; possibly by ingestion
Studies in mice suggest that capillary leak and hemorrhage result from LPS mediated disruption of vessel wall via intercallation of glycoprotein toxin |
|
|
Pathogenesis - from second week on
|
From second week
Antibody raise, immunological damage LPS and TNF- |
|
|
Pathogenesis - first week
|
First week
Leptospira in blood and CSF Blood vessels, liver, kidney, muscles and lungs are affected early |
|
|
What is the Septicemic phase?
|
Septicemic phase
One to several days Fever, conjunctival suffusion, myalgias, bradycardia, (+ cultures) hypotension, dehydration Recovery 5d - 6w |
|
|
Pathogenesis - from second week on
|
From second week
Antibody raise, immunological damage LPS and TNF- |
|
|
Immune phase
|
Fever recurrence, rigors,
headaches, prostration, myositis (high CK), rash, mono or polyarthritis, organ manifestations Convalescence 6-12 w Jaundice and bilirubinemia out of proportion with hepatocellular damage is the usual finding in leptospirosis Significant jaundice + aminotransferases no more than 3-4 X normal + alkaline phosphatase as high as 10 X normal; the mechanism of the cholestasis in leptospirosis is not clear Second fever Severe paraspinal and calf tenderness Acalculous cholecystitis Guaiac positive stools Irritability and depression well into convelescent phase In severe or prolonged disease, renal damage will occur and the sediment is usually active. Non-oliguric hypokalemic renal failure as found in this case is characteristic. Progression to oliguric renal failure is predictive of higher mortality |
|
|
What is the Septicemic phase?
|
Septicemic phase
One to several days Fever, conjunctival suffusion, myalgias, bradycardia, (+ cultures) hypotension, dehydration Recovery 5d - 6w |
|
|
Weil Syndrome - from slides
|
Temp 40°C
Warm and flushed skin Jaundice Muscle tenderness Acute tubular necrosis and hypovolemia resulted in renal failure High CPK from skeletal muscle involvement |
|
|
Immune phase
|
Fever recurrence, rigors,
headaches, prostration, myositis (high CK), rash, mono or polyarthritis, organ manifestations Convalescence 6-12 w Jaundice and bilirubinemia out of proportion with hepatocellular damage is the usual finding in leptospirosis Significant jaundice + aminotransferases no more than 3-4 X normal + alkaline phosphatase as high as 10 X normal; the mechanism of the cholestasis in leptospirosis is not clear Second fever Severe paraspinal and calf tenderness Acalculous cholecystitis Guaiac positive stools Irritability and depression well into convelescent phase In severe or prolonged disease, renal damage will occur and the sediment is usually active. Non-oliguric hypokalemic renal failure as found in this case is characteristic. Progression to oliguric renal failure is predictive of higher mortality |
|
|
Neurologic manifestations
|
Headache, meningismus, meningitis
Mononuclear pleocytosis, protein elevation, normal glucose in CSF Occasional encephalitis Rarely Transverse myelitis, Guillain-Barré, cranial nerve paralysis |
|
|
Weil Syndrome - from slides
|
Temp 40°C
Warm and flushed skin Jaundice Muscle tenderness Acute tubular necrosis and hypovolemia resulted in renal failure High CPK from skeletal muscle involvement |
|
|
Icteric leptospirosis
|
Fever, jaundice and purpura
|
|
|
Neurologic manifestations
|
Headache, meningismus, meningitis
Mononuclear pleocytosis, protein elevation, normal glucose in CSF Occasional encephalitis Rarely Transverse myelitis, Guillain-Barré, cranial nerve paralysis |
|
|
Icteric leptospirosis
|
Fever, jaundice and purpura
|
|

what is this?
|

Conjunctival suffusion and hemorrhages, no conjunctivitis
|
|
|
Lumbar puncture aseptic meningitis
|
Lymphocytic pleocytosis, counts </= 500, mild protein elevation, normal glucose
|
|
|
Coagulation alterations
|
Thrombocytopenia
Abnormal bleeding and coagulation times Low factor V Increased fibrin split products DIC |
|
|
Pulmonary disease
|
Dry cough
Shortness of breath Hemoptisis Chest pain Radiological infiltrates Severe vascular injury can cause pulmonary hemorrhage |
|
|
Renal manifestations
|
Acute renal failure
Creatinine 2-8 mg/dl Not always related to disease severity Abnormal urinalysis 80-90% Leucocytes, hyaline, granular or hematic casts, hemoglobinuria Anuria is rare and poor prognostic sign |
|
|
Renal leptospirosis
|
Interstitial nephritis
Acute tubular necrosis* Impaired capillary permeability Hypovolemia Renal failure Urine is a reliable body fluid to study because leptospires are present from start to finish of Sxs. |
|
|
What is the cause of most leptospirosis associated deaths?
|
Renal failure has been the cause of most leptospirosis associated deaths
but hemodialysis and peritoneal dialysis have reduced mortality |
|
|
GI manifestations
|
Nonspecific
Nausea,vomiting, abdominal pain*, diarrhea, anorexia. Pancreatitis is rare Direct hyperbilirrubinemia Increased aminotransferases Elevated alkaline phosphatase Hypoalbuminemia |
|
|
Ocular manifestations
|
Ocular
-Subconjunctival hemorrhage* -Conjunctivitis, anterior uveitis |
|
|
General Manifiestations
|
General
-Pharyngitis -Parotitis -Adenomegaly -Splenomegaly -Arthritis -Myocarditis -Exanthema -Urticaria |
|
|
Diagnosis
|
Dark field direct examination
Cultures*, isolation is gold standard. Fletcher, Stuart, PLM-5 media (serum + 5FU) Animal inoculation Serology* PCR Blood, serum, urine, CSF, aqueous humor |
|
|
What is unique about patients with severe disease?
|
Patients with severe disease usually have >10,000 organisms per ml of blood or tissue
|
|
|
Isolation of Leptospira in culture is __and __
|
Isolation of Leptospira in culture is difficult and insensitive
|
|
|
Culture in special media in tubes held at __ for prolonged periods is necessary
|
Culture in special media in tubes held at 28-30°C for prolonged periods is necessary
|
|
|
__is only positive in the __of illness after which __becomes progressively more positive
|
Blood is only positive in the first week of illness after which urine becomes progressively more positive
|
|
|
__ are only visible and confirmed using__
|
Cultured leptospires are only visible and confirmed using dark-field microscopy
|
|
|
Diagnosis is most often __and __, __, or a commercially available __
|
Diagnosis is most often serological and retrospective [MAT], IgM ELISA, or a commercially available rapid dipstick test
|
|
|
__ diagnosis is effective, quantitative, and rapid compared to other techniques but remains a research tool
|
PCR-based diagnosis is effective, quantitative, and rapid compared to other techniques but remains a research tool
|
|
|
Differential diagnosis
|
Malaria*
Hepatitis* Dengue* and yellow fever Salmonella and brucella infections Hemorrhagic fevers Infectious mononucleosis Cholecystitis, cholangitis * top 3 |
|
|
Laboratory Diagnosis
|
Culture
Microagglutination test Enzyme-linked immunosorbent assay (ELISA) Molecular |
|
|
Culture - what is needed
|
Culture
Specimen transport, inoculation Specialized medium, 28-30 ºC incubation Microscopic examination of cultures |
|
|
What is the Microagglutination test looking for?
|
Microagglutination test
Lipopolysaccharide (LPS) |
|
|
What is the Enzyme-linked immunosorbent assay (ELISA) test looking for?
|
Enzyme-linked immunosorbent assay (ELISA)
IgM, IgG |
|
|
What does molecular testing do?
|
Molecular
PCR Real time PCR, quantification of leptospiremia Molecular typing methods for specific identification |
|
|
Treatment
|
Specific
Penicillin* or Ampicillin* or Ceftriaxone Doxicycline* Non-specific Mild to moderate forms Hydration and symptom relief Severe forms Life support in intensive care units |
|
|
Prognosis
|
Good in anicteric forms
In icteric forms, mortality, usually from acute renal failure or irreversible myocardial failure is 15-40 % Full recovery is expected within 6-12 weeks |
|
|
Traveller's Prophylaxis recs
|
Some travelers should be advised to take doxycycline 200mg. twice per week, we tend to treat individuals
|
|
|
Summary
|
Outbreak due to leptospirosis
High attack rate 10% had febrile jaundice Inconclusive zoonotic source IgM ELISA (Antigen=L. biflexa serovar Patoc) insensitive in this setting |
|
|
Prevention
|
Personal protection measures
Individuals exposed to single events with high risk of infection or visitors of endemic areas can be given prophylactic doses of doxycicline Environmental sanitation Control of reservoirs Animal vaccination |