Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
57 Cards in this Set
- Front
- Back
|
Meninges 3 connective tissue layers
|
1. Pia mater- (vascular) closely covers brain
2. arachnoid- (non-vasc) 3. Dura matar- outer layer and dense |
|
|
3 meningial spaces
|
1. subarachnoid- terminates atthe second sacral level and consist of CSF
2. Subdural; - in cranium it carries veins - in spinal cord; potential space 3. Epidural: - cranium; potential space, with meningeal aa and vv - spinal cord, it contains fatty areolar tissue, lymphatics and venous plexuses (LA injection causing paravertebral or saddle nerve block) |
|
|
Meningial Pathologies
|
- meningial tumours
- subdural & epidural hematomas - meningitis |
|
|
Meningiomas
|
- benign, well circumscribed, slow growing
- 15% of intracranial tumours - 90% supratentorial |
|
|
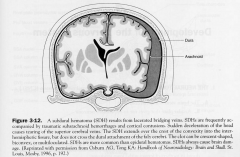
Subdural Hematoma
|
- laceration of superior cerebral vv.
|
|
|
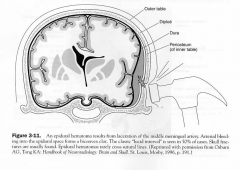
Epidural Hematoma
|
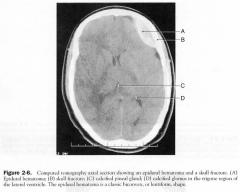
- laceration of middle meningeal aa.
- they may cross dural attachments - CT: biconvex or lentiform shape - anterior, middle or posterior meningeal aa. |
|
|
Meningitis
|
inflammation of pia-arachnoid arewas of brain and/or spinal cord
|
|
|
CSF Flows
|
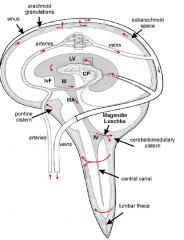
- made @ choroid plexuses of ventricles
- exits @ 4th - circualtes subarachnoid space - enter super sagittal sinus through arachnoid granulations |
|
|
Bacterial Meningitis Sx
|
- fever, headache, nuchal rigidity (neck stiffness, cant flex the neck) and Kernig's sign (patient supine, examiner flexes the hip but cant extend the knee without causing pain)
- cranial nerve palsies and hydrocephalus |
|
|
Common Causes of Bactrial Meningitis
|
- NEWBORN: GBStrep & E.Coli
- YOUNG CHILDREN: HiB - YOUNG ADULTS: N.meningitidis - OLDER ADULTS: S.pneumoniae |
|
|
CSF Finding sin Bacterial Meningitis
|
1. LOTS of PMN leukocytes
2. Dec. G 3. Inc. Protein |
|
|
Viral Meningitis (aka aseptic meningitis)
Sx |
- fever, headache, nuchal rigidity and kernigs sign
|
|
|
Viral Meningitis Common Causes
|
mumps
echovirus coxsackie virus EBV HSV-2 |
|
|
Viral CSF
|
1. LOTS of PMN leukocytes
2. Normal G 3. Moderately Inc. Protein |
|
|
Choroid Plexus
|
- lateral, 3rd & 4th ventricles
- modified ependymal cells secrete the CSF and tight junctions form the blood-CSF barrier |
|
|
Pathway through Ventricles
|
1. 2 lateral ventrical
2. connect to 3rd via interventricular foraina of monro 3. 3rd V between the diencephalon 4. Connects to 4th via the cerebral aqueduct (no chorid here and blockage cause hydrocephalus) 5. 4th V communicates with subarachnoid space with 3 outlets a. foramen of magendie (median aperture) b. 2x foramina of luschka (lateral aspects) - then to cerebellomedullary cistern - downwards and around spinal cord - anteriorly and upwards into the pontine and interpeduncular cisterns - upwards and posteriorly, around the cerebellum and into the cistern posterior to the midbrain |
|
|
Hydrocephalus
- 5 types |
dilation of V due to blockage of CSF flow
1. Noncommunicating Hydrocephalus (within) 2. Communicating; within the subarachnoid (adhesions from meningitis) or no obstruction just lack of absorption 3. Normal pressure; when CSF isnt abs by arachnoid villi (triad; progressive dementia, ataxic gait, urinary incontinence; wacky, wobbly and wet) 4. Hydrocephalus ex vacuo; due to a loss of cells in the caudate nucleus (eg HD) 5. Pseudotumor cerebri; benign redults from INC. resistance to CSF outflow at the arachnoid villi. Occurs in obese young women |
|
|
CSF-
Function |
-colourless, acellular
1. supports CNS and protects against concussive injury 2. transport of hormones 3. Removes metabolic waste 4. buoyancy (red. effective brain weight to 50g) |
|
|
CSF formed & abs.
|
@ chroid plexus (80% some by ependyma cells of brain); choriod is found all over ventricle sysem except anterior and posterior horns of LV (500ml/day) when we only have 150ml at one point
@ arachnoid villi in super sagittal sinus (connect SAS with venous lumen). It is pressure & volume dependent (unlike production) |
|
|
CSF Composition
|
COLOUR: clear
1. mononuclear cells less than 5/uL 2. RBC indicates subarachnoid hemorrhage 3. G; 50-75mg/dl 4. Protein: 15-45mg/dl 5. CSF pressure; lateral recumbent position 80-180mmH2O differs from plasma in having excess Na, Mg and little K, Ca |
|
|
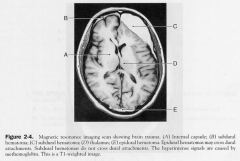
Brain Herniations
|
1. Transtentorial (uncal) herniation
2. Transforaminal (tonsillar) herniation; through foramen magnum 3. Subfalcial herniation; below falx cerebri |
|
|
Subdural Hematoma
|
|
|
|
EDH
|
|
|
|
Where do the cerebral blood vessels at the brain surfeace travel?
|
Sub-arachnoid space
|
|
|
Cistern
|
space between the aracnoid and pia matar, esp around the brainstem
(i) cerebellomedullary (cisterna magna): space between inferior surface of cerebellum and dorsal surface of medulla. (ii) pontine: space around anterior surface of pons: continuous caudally with cerebellomedullary (iii) interpeduncular: between cerebral peduncles, which contains Circle of Willis (iv) superior cistern (cistern of great cerebral vein of Galen): a radiological landmark above midbrain. Occupies interval between splenium of corpus callosum and superior surface of cerebellum. Contains great cerebral vein of Galen and pineal gland and continues rostrally into transverse fissure. Cistern ambiens: group around midbrain encircling it |
|
|
Dural Venous sinuses
|
form between the 2 dural layers
|
|
|
3 dural folds in the brain
|
1. falx cerebri
2. falx cerebelli 3. tentorium cerebelli |
|
|
Subarachnoid Bleeds
|
- most common (aneruysms)
- blood in Sas mixes with CSF coating the pia with RBCs - With time the RBCs die and release Hb which vasoconstricts the aa. and may cause a stroke |
|
|
Lateral ventricle Componenets
|
i) anterior horn (frontal lobe)
(ii) body: in frontal and parietal lobes, extending posteriorly to splenium of corpus callosum. (iii) posterior horn: projecting into occipital lobe. (iv) inferior horn: curving down and forward into temporal lobe. (v) collateral trigone: region near splenium of corpus callosum where body and posterior and inferior horns meet |
|
|
The 3rd ventricle continuity is broken by?
|
inter thalamic adhesions
|
|
|
CSF production per day
|
500mL
replaced 4 x a day - no feedback system limiting its production |
|
|
BBB function
|
- maintain electrolyte levels
- control entry of particular substrates (eg, glucose) - protect from circulating hormones (eg, systemic neurotransmitters) - remove waste products - exclude toxins |
|
|
Astrocytes cover ___% of blood vessel surface
|
85
|
|
|
3 barriers of the BBB
|
1. Arachnoid: tight junctions, passively keeps out hydrophillic substances
2. Choroid Plexus: choriod epithelium regulate things that leave chorioid capillaries not allowing direct acess to the CSF 3. Cerebral Non-fenestrated Capillaries therefore; only LMW or lipid soluble substances can diffuse across |
|
|
3 types of spina bifida
|
1. Spina bifida Cystica; myelomeningocele
- form a sac that protrudes leaking CSF, teethered cord, hydrocephalus LEAKS! 2. OCCULTA: mildest form occuring in 10% of pop. where the arch of a single vertebra is open (L5 or S1) 3. CYSTICA- meningocele: same as occulta but several vertebra involved, thus protusion with a fluid filled sac - normal spinal cord and no leakage CAN SHINE A LIGHT THROUGH IT |
|
|
Causes of INC. ICP
|
(1) Mass: expanding mass that is replacing and/or compressing brain; eg abscess, tumours
(2) Oedema: brain oedema may develop from tumour/abscess mass and/or pus. (3) Blood Volume: excessive vasodilation (4) Cerebrospinal Fluid: impaired absorption or excessive secretion rate. |
|
|
MEchanism of CSF secretion
|
passive and active
- carbonic anhydrase drives Cl and water secretions into plasma and CSF |
|
|
The Biggests 3 differences between CSF and plasma composition
|
1. CSF has 99% water content vs 93%
2. Lower protein 3. Higher Cl |
|
|
Name the 3 main dural venous sinuses?
|
1. SSS
2. Straight sinus 3. Transverse Sinus |
|
|
Davson's Equation
|
CSF absorption depends on
Abs= Pressure of CSF - (P SSS + 3mmHg) / R CSF normal pressure 7-15cmCSF or 5-12mmHg - erect (vs supine) |
|
|
CSF Ix
|
1. radiology and ventricular size
2. Lumbar puncture (l4-5) 3. CSF infusion studies (measure baseline pressure then insert more fluid and measure pressures again) 4. |
|
|
How to perform an LP?
|
@ L4-5
in line with the Iliac crest |
|
|
Different colous of CSF
|
1. xanthochromic (breakdown of blood)
2. Turbid (lots of protein) 3. Blood stained (haemorrage or a **** job) |
|
|
Aetiology of Hydrocephalus INFANT
|
Newborn
Congenital • Aqueduct stenosis • Communicating • Myelomeningoceles Acquired • IVH of Prematurity • Meningitis |
|
|
Aetiology of Hydrocephalus ADULT
|
Adults
Meningitis Haemorrhage – SAH Tumour Surgery Aqueduct stenosis - LOVA Idiopathic – NPH |
|
|
High, Normal and Low CSF pressures
|
High Pressure
Acute, obstructive Normal NPH, LOVA, chronic, arrested Low Infection, haemorrhage – rare cases |
|
|
Sx of Acute Hydrocephalus
|
Headache, nausea and vomiting
Lethargy, drowsiness, stupor and coma |
|
|
Signs of acute hydrocephalus
|
Papilledema, Diplopia
Setting sun sign False localising signs – 6th nerve signs Decreased level of consciousness |
|
|
Munro-Kellie Doctrine
|
Cranium is a rigid sphere
Filled to capacity with Brain CSF Blood These are non-compressible (nearly) “An increase in volume of one of these components or the introduction of a mass lesion must be accompanied by a decrease in volume of the other components” |
|
|
Normal Pressure Hydrocephalus Triad
|
Gait disturbance (short, shuffling, magnetc, broad based; like PK without tremor)
Dementia Urinary incontinence Idiopathic: Condition of the elderly Secondary: Trauma, SAH, meningitis |
|
|
Chiari II Malformation
|
- tonsils a pulled down into the spinal cord due to teethering
- myelomeningocele assoc. with Chiari II |
|
|
Tx of Hydrocephalus
|
1. third ventriculostomy
2. CSF Shunting; valve regulated Ventriculo – peritoneal Ventriculo – pleural Ventriculo - atrial Lumbo – peritoneal etc |
|
|
Pseudotumor Cerebri
|
aka
Idiopathic intracranial hypertension benign intracranial HT DEFINITION: Increased intracranial pressure in the absence of a mass lesion or hydrocephalus young overweight females of childbearing age AFFECTED S&S Increase ICP Headache Blurred vision / restricted vision Papilledema Blindness |
|
|
Pseudotumor Cerebri Tx
|
Acetazolamide
Lumbar Punctures Optic Nerve Sheath Fenetrations (to protect their eyes from the papioedema) CSF Shunting Bilateral Subtemporal decompressions (making a little more room in the cranial cavity) Venous sinus stenting (by stenting tehe venouse pressure is lowered therefore lowering the required CSF pressures) |
|
|
Normal the CSF pressure needs to be __________ than the ________ pressure
|
CSF and venous
|
|
|
Definition of Hydrocephalus ex-vacuo
|
Hydrocephalus ex-vacuo: What is termed "hydrocephalus ex-vacuo" occurs when there is damage to the brain caused by stroke or injury, and there may be an actual shrinkage of brain substance. Although there is more CSF than usual, the CSF pressure itself is normal in hydrocephalus ex-vacuo.
Hydrocephalus is an abnormal buildup of cerebrospinal fluid (CSF) in the ventricles of the brain. The fluid is most often under increased pressure and that pressure can compress and damage the brain. |
|
|
Chorois plexus Locations
|
Choroid plexus is present in all components of the ventricular system except for the cerebral aqueduct, frontal horn of the lateral ventricle,[1] and occipital horn of the lateral ventricle.[1]
Choroid plexus It is found in the superior part of the inferior horn of the lateral ventricles. It follows up along this boundary, continuous with the inferior of the body of the lateral ventricles. It passes into the interventricular foramen, and is present at the top of the third ventricle. There is also choroid plexus in the fourth ventricle, in the section closest to the bottom half of the cerebellum. |