![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
25 Cards in this Set
- Front
- Back

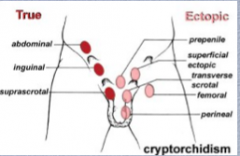
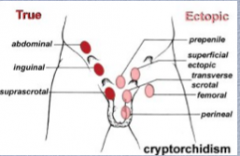
What is shown here?
What percent of boys? What age commonly?
What percent unilateral/bilateral?
What is the pathogenesis?
What are the two phases of development and what occurs in each? What phase does this defect most commonly occur in? |
|
|
|
|
|
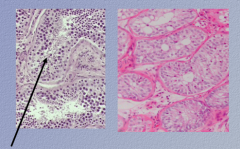
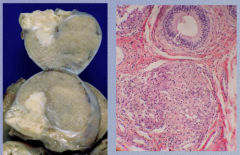
Which is normal, which is cryptorchid with total absence of spermatogenesis?
What are two complications of cryptorchidism?
Decreased spermatogenesis in ______ testes in unilateral cryptorchidism. Systemic mechanism, poorly understood (not just “______testis”)
|
Inguinal testis is susceptible to trauma Sterility
Decreased spermatogenesis in BOTH testes in unilateral cryptorchidism |
|

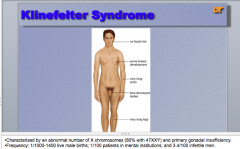
What are some physical signs of Klinefelter Syndrome?
What genotype do 80% have? Are the gonads functional?
What is the frequency? |
|
|
|
•Klinefelter Syndrome:
Clinical: |
•Clinical: |
|
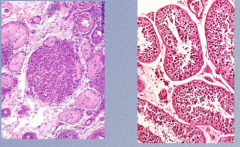
Normal on right
This testicular biopsy is from an adult male with history of normal semen volume and severe oligospermia. He had small firm testes and body habitus suggestive of Klinefelter’s syndrome. The biopsy shows small hyalinized seminiferous tubules and pseudo-adenomatous clusters of Leydig cells. What is the condition? |
Klinefelter syndrome |
|
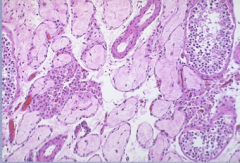
How would you describe the testicular tubules here? What is the most common infectious cause for this finding? |
Focal atrophy
Mumps orchitis |
|
|
Mumps infection post puberty may be complicated by ______ in a fourth to a ______ of cases. In general, the orchitis is ______ (bilateral or unilateral) and patchy so that sterility following ______ is uncommon. Other infectious agents associated with orchitis may include echovirus, lymphocytic ______ virus, influenza virus, ______virus, and arboviruses. In contrast, ______ is a more frequent cause for scrotal pain and swelling in adult males and is most likely to be the result of a ______ disease such as Chlamydia trachomatis or ______ in younger males or gram negative bacteria from urinary tract infection of ______ males. Disseminated tuberculosis may occasionally involve the ______. |
Mumps infection post puberty may be complicated by orchitis in a fourth to a third of cases. In general, the orchitis is unilateral and patchy so that sterility following infection is uncommon. Other infectious agents associated with orchitis may include echovirus, lymphocytic choriomeningitis virus, influenza virus, Coxsackie virus, and arboviruses. In contrast, epididymitis is a more frequent cause for scrotal pain and swelling in adult males and is most likely to be the result of a sexually transmissible disease such as Chlamydia trachomatis or Neisseria gonorrheae in younger males or gram negative bacteria from urinary tract infection of older males. Disseminated tuberculosis may occasionally involve the epididymis. |
|
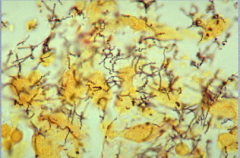
What is shown here? Which phase? What is the pathway of infection of this phase. Contrast this with gonorrhea. |
Tertiary syphilis (spirochetes) Testis => then epididymis
Gonorrhea => retrograde from urethra to the prostate => seminal vesicles => epididymis => prostate |
|
What is the disease shown in the testes here? How does it spread? |
Typically, tuberculosis spreads retrograde from the prostate to the epididymis, then to the testis. The left panel shows involvement of both the epididymis and the testis; microscopically, a granuloma is seen in the epididymis. It is a very young granuloma, so typical caseation is not yet seen. |
|
What is this? |
Testis = granulomatous orchitis |
|
|
Idiopathic granulomatous orchitis is an uncommon ______ testicular lesion that follows a gram ______ urinary tract infection in the majority of cases. It is most prevalent in the ___ and ___ decades. Testicular involvement is usually diffuse but may also present as a localized ______ lesion and may simulate a testicular ______. The epididymis and ______ may also be involved. A related process is autoimmune ______, which is clinically described as rapid onset testicular enlargement in ______ aged men which may be associated with a febrile illness. Histology shows ______ without organisms. An autoimmune etiology is proposed. |
Idiopathic granulomatous orchitis is an uncommon inflammatory testicular lesion that follows a gram negative urinary tract infection in the majority of cases. It is most prevalent in the 5th and 6th decades. Testicular involvement is usually diffuse but may also present as a localized nodular lesion and may simulate a testicular neoplasm. The epididymis and spermatic cord may also be involved. A related process is autoimmune orchitis, which is clinically described as rapid onset testicular enlargement in middle aged men which may be associated with a febrile illness. Histology shows granulomas without organisms. An autoimmune etiology is proposed. |
|

What is the mnemonic for testicular regression? |
V—Vascular conditions bring to mind varicoceles, which cause atrophy on the side of the dilated veins. |
|

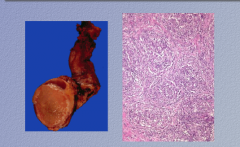
What is this an image of? |
Torsion of the testis |
|
|
Torsion is twisting of the ______, leading to ischemia and ______ stasis. It may be related to trauma, but frequently the inciting event is ______. Often there will be a predisposing anatomic abnormality which allows the testis excess ______ within the scrotum (“bell clapper phenomenon”); this abnormality may be ______, which is why there is a risk of contra lateral torsion in a patient who has torsion. This is a true urologic emergency, since surgery within ______ hours may save the testis; after that, hemorrhagic ______ with obliteration of the testis is inevitable if reduction of the torsion is too late. |
Torsion is twisting of the spermatic cord, leading to ischemia and venous stasis. It may be related to trauma, but frequently the inciting event is obscure. Often there will be a predisposing anatomic abnormality which allows the testis excess mobility within the scrotum (“bell clapper phenomenon”); this abnormality may be bilateral, which is why there is a risk of contra lateral torsion in a patient who has torsion. This is a true urologic emergency, since surgery within 4-6 hours may save the testis; after that, hemorrhagic infarction with obliteration of the testis is inevitable if reduction of the torsion is too late. |
|
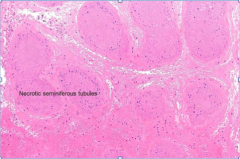
What is the condition (what would cause the seminiferous tubules to become necrotic)? |
Torsion of the testis |
|
What is shown in the image? What are 50% of germ cell tumors? What is the histologic hallmark?
What are 15% of germ cell tumors produce? |
Germ cell tumors: |
|
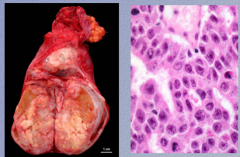
Embryonal carcinoma (occasionally a ______ tumor, but much more commonly a component of a mixed ______ cell tumor) |
Embryonal carcinoma (occasionally a pure tumor, but much more commonly a component of a mixed germ cell tumor) |
|
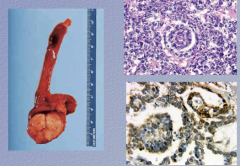
What type of tumor? (______ sinus tumor) |
Yolk sac tumor (endodermal sinus tumor) |
|
|
What is alpha-fetal protein? |
Fetal albumin |
|
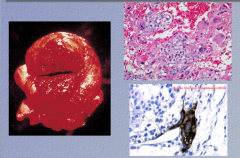
What is the tumor type?
Only ___% of germ cell tumors are pure chorio, but chorio is commonly represented in mixed ______ cell tumors. |
Only 1% of germ cell tumors are pure chorio, but chorio is commonly represented in mixed germ cell tumors. |
|
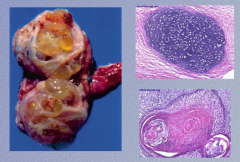
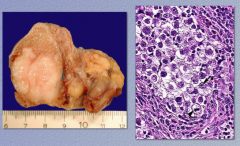
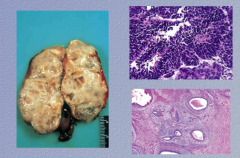
What type of tumor is this? (that's cartilage...) |
Teratoma! |
|
|
Teratoma:
In pure form, teratoma is more common in ______…rare in ______; it is commonly mixed with other ______ cell tumor types in adults
Mature types (with ______ tissues) and immature types with (______ tissues) exist
Tissue represents more than one _______ layer. May be grossly quite large with variegated color and texture; ______ are common
This photo represents a mature testicular teratoma in a 22 year old; mature cartilage and skin are represented in the photomicrographs. |
Teratoma |
|
What is the tumor type? What type of tissue does it demonstrate? |
Germ cell tumors: |
|
|
Remind your male patients to do testicular self exams just as you remind your female patients to do breast self exams; you very well may save a life! |
Remind your male patients to do testicular self exams just as you remind your female patients to do breast self exams; you very well may save a life! |