![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
30 Cards in this Set
- Front
- Back
|
What serves as the septum between right and left pouches? How about Medial to lateral? |
Longus capitus and restus capitus mm Stylohyoid bone |
|
|
Who lives in the Medial compartment? (8) |
1) Sympathetic trunk 2) Hypoglossal (XII) 3) Glossopharyngeal (IX) 4) Accessory (XI) 5) Vagus (X) 6) Internal Carotid a 7) Longus capitus muscle 8) Retropharyngeal LNs |
|
|
Who lives in the Lateral compartment? (4) |
1) Maxillary branch of the external carotid a 2) Maxillary v 3) Facial (VII) 4) Digastricus muscle |
|
|
Remind me about the blood flow again? |
Retrograde flow internal = circle of willis external = transverse facial and palatine Left to right |
|
|
What diagnostics can we use with gutteral pouches ( |
1) Upper airway endoscopy 2) Radiographs 3) CT 4) MRI 5) Culture and sensitivity (Strep MC) 6) Biopsy |
|
|
Etiologies of Guttural pouch Empyema (5): |
1) Upper Resp Tract INFXN (beta-hemolytic strep= equi and zoo 2) rupture of retropharyngeal LNs 3) Middle Ear infection 4) Fractured stylohyoid bone 5) Pharyngeal trauma |
|
|
Medical Treatment of Guttural pouch empyema: |
Lavage through nasal passage ABX Anti-inflamm may take several treatments to get it all |
|
|
Clinical signs of Guttural pouch empyema |
Nasal Discharge (any combo) Swelling (caudodistal to ramus of mandible Lymphadenopathy Dysphagia (Hypo and glosso) Facial nerve paraly (neuritis Horner's Syndrome (sympathetic trunk) |
|
|
Differential DX for guttural pouch empyema |
Upper resp Pneumonia sinusitis GP tympany GP mycosis Retropharyngeal abscess |
|
|
Diagnostics for Guttural pouch empyema |
endoscopy Rads ( see fluid line) |
|
|
Surgical Treatment for guttural pouch empyema |
Modified Whitehouse = Ventral and Medial to the linguofacial vein (Best ventral drainage and best access ventral opening) Viborg Triangle= Sternomandibularis tendon, vertical ramus of mandible, linguofacial vein (some ventral drainage and avoid neurovascular) Hyovertebrotomy= Dorsolateral at caudal aspect of pouch (No ventral drainage) |
|
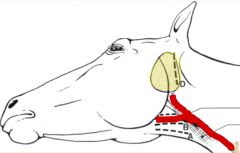
Who's B: Who's C: Who's D: |
B= Modified Whitehouse C= Viborg Triangle D= Hyovertebrotomy |
|
|
Prognosis and Complications of Guttural Pouch Empyema? |
GOOD Aspiration Pneumonia Airway Obstruction |
|
|
Gutteral Pouch Mycosis MC site in guttural pouch is? |
Dorsocaudal aspect of medial compartment |
|
|
What are the clinical signs of guttural pouch mycosis (8)? Remember who lives there |
1) Dysphagia- may ne only presenting complaint 2) Epistaxis- remember increase severity with each bleed 3) Facial paralysis 4) Horner's 5) Laryngeal paralysis 6) Head shaking 7) Blindness 8) Respiratory stridor |
|
|
What other differentials are there for guttural pouch mycosis (8)? |
1) Upper Resp infections 2) Gutteral pouch empyema 3) Rupture of longus capitis and rectus capitis ventralis mm +/- basiophenoid fracture 4) Sinusitits 5) Ethmoid hematoma 6) Neoplasia 7) Pulmonary Abscess 8) EIPH |
|
|
How do we diagnose guttural pouch mycosis? |
Endoscopy Rads CBC- Leukocytosis, anemia, and hypoproteinemia Fungal culture |
|
|
What does guttural pouch mycosis medical treatment look like? |
Systemic and topical antifungals anti-inflamm Supportive therapies |
|
|
surgical treatment of guttural pouch mycosis: |
Occlude effected vessels ligate- recall retrograde balloon occlusion transarterial coil embolization |
|
|
Prognosis of guttural pouch mycosis |
Fair with no dysphagia surgical before medical better chance of resolution |
|
|
possible sequela of guttural pouch mycosis |
Fatal hemorrhage pharyngeal fistula erosion through septum osteitis of stylohyoid bone blindness secondary to vessel occlusion |
|
|
A little bit about guttural pouch tympany |
Not really Common air- filled dilation redundant or thickened plica salpingopharyngea results in trapped air congenital-young (up to 1 year) |
|
|
Clinical signs of guttural pouch tympany |
Respiratoty Stridor Marked swelling caudal to ramus of mandible (nonpainful, fluctuating) Dyspnea Aspiration pneumonia |
|
|
How to we diagnose guttural pouch tympany |
Endoscopy Rads *Lateral- air distended pouch, empyema *DV- tell bilat or unilat * Thorax - aspiration pneumonia |
|
|
Medical treatment of guttural pouch tympany |
prolonged indwelling catheter ABX |
|
|
Surgical treatment of guttural pouch tympany |
Fenstration across pouches or fistual out if bilat Approaches= modified whitehouse and virborg's triangle |
|
|
Prognosis for guttural pouch tympany |
ok if unilateral worse if bilat poor medical alone can recurr if fenestration closes with scar |
|
|
How about Temporohyoid Osteoarthropathy |
clinical signs depend on nerves affected diagnose endoscopy > rads, MRI/CT for planning treatment- conservative (treat the signs), surgical (certahyoidectomy) Prognosis- good to guarded dont fracture the stylohyoid |
|
|
What happend when you rupture the ventral straight muscles? |
Bleed into guttural pouch rupture- longus capitis and rectus capitis ventralis can fracture basisphenoid-basioccipital junction |
|
|
CS, DX, and PX of rutpturing the ventral straight muscles |
CS= severe epistaxis, ataxia, recumbancy DX= rads, endoscopy Px= fair no neuro deficits, poor if can't rise |