![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
83 Cards in this Set
- Front
- Back
|
How many bones does the viscerocranium have? |
14 facial bones! (plus frontal bone)nasal - 2lacrimal - 2 Palatine - 2Zygomatic - 2Vomer - 1 Mandible - 1Maxilla - 2 Inferior Nasal Conchae - 2 |
|
|
How long does face development take? |
Between 4-8 weeks of gestation. The mandible is first to develop at 4th week |
|
|
What are the 2 main features of skull? |
1. Protect brain 2. Protect facial structures |
|
|
How can you divide the neurocranium? |
1. Calvarium (roof) consists of frontal, parietal, occipital 2. Cranial Base (floor) has some of the calvarial bones: frontal, ethmoid, cribiform plate (transmit the olfactory nerves), sphenoid, temporal and parietal, occipital 6 bones totally |
|
|
What is the face derived from? |
Derived from 5 parts of tissue: facial primordia Begins at week 4 in the uterus. Finished by week 8 |
|
|
How many buds of tissue does the embryo have? |
5 buds of tissue all from mesenchyme (from neural crest) 1. Frontonasal prominence -frontal bone 2. Maxillary prominence (x2) -2 maxilla 3. Mandibular prominece (x2) -x2 mandible Also have stomodeum in the middle - goes on to form the opening of the oral cavity |
|
|
What happens in the beginning of 4th week? |
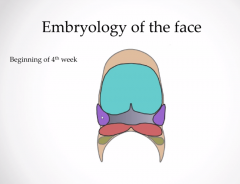
the 5 buds 1st pharyngeal arch: maxilla + mandible prominences |
|
|
What happens in the end of 4th week? |
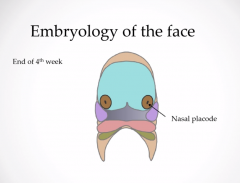
Have 2 nasal placodes At the front of frontonasal prominences. They are bits of mesenchyme which will go on to form nasal tissue. |
|
|
Week 5 |
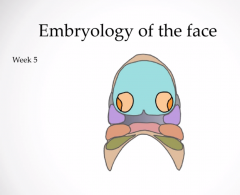
You have mesenchymal cells proliferating at the border of the placodes. These are known as medial nasal prominence - becomes nasal septum and fultrum of upper lip. You also have the lateral nasal prominence - goes to become the nasal ala (side of the nose) |
|
|
Week 6 |
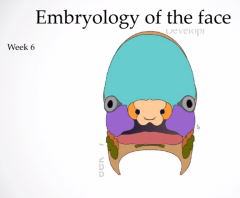
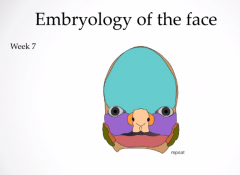
Looks more like human. The 2 maxillary prominences are getting bigger and they are squashing the two medial nasal prominences to form the nose and upper lip. |
|
|
week 7 |
|
|
|
Cleft Lip - What is it? |
Definition: a common pathology of max-fax, esp paediatrics. It is a failure of the 2 medial nasal prominences to FUSE TOGETHER (between week 4-6) prevalence: 1 in 700 live births |
|
|
What are the categories of cleft lip? |
1. unilateral or bilateral 2. complete or incomplete -left is more common than the right. -incomplete means it doesnt affect the nasal septum, only affects the upper lip. -complete = affects the upper lip, fultrum and nasal septum |
|
|
What is the main issue with cleft lip? |
feeding and articulations |
|
|
when do cleft lip surgery takes place? |
Usually repair within 10 weeks of birth. RULE of 10s: operate within 10 weeks, when baby weighs 10 Lb and has 10g of Haemoglobin. -if cleft is extensive, may take more than one surgery |
|
|
What is cleft palate? |
Related but NOT the same. Failure of fusion of the medial nasal prominences. Cleft palate occurs between 6-8 weeks of development. Cleft palate can also occur with cleft lip. |
|
|
What is the classification system of cleft palate? |
Same as cleft lip. 1. Unilateral incomplete - just hard and soft palate, not the lip 2. Unilateral complete - all of palates and lip and going up 3. bilateral complete - most severe. Needs to be repaired because of feeding and articulations issues |
|
|
When is cleft palate repaired? |
-a little later than cleft lip -between 6 to 12 months. In the mean time to fill the deficit in the palate, they put a little plastic plate (known as the palatal obturator) that will help the baby feed until surgery |
|
|
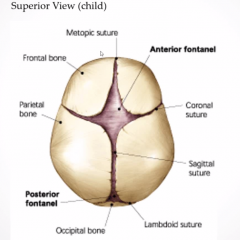
What are sutures? |
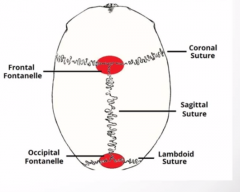
-development of the neurocranium -metopic suture runs from frontal fontanelle to bridge of the nose |
|
|
what joints are sutures? |
-fibrous joints, unique to the skull -give them a lot of stability -fuse completely at age 25-30 EXCEPTION: metopic suture (cant see normally) runs across the frontal bone, fuses in childhood (age 12) |
|
|
Difference between children and adult sutures? |
-fontanelles: soft depressions 1. Frontal in front 2. Occipital in the back -usually fuse by 1-2 years -allow for skull expansion as the brain grows -also useful in radiology for cranial USS probing in the fontanelles to scan brain of infant |
|
|
how does the skull look like in a baby? |
|
|
|
What happens when the sutures fuse prematurely? |
CRANIOSYNOSTOSIS -1 in 2000 to 1 in 5000 development (RARE than cleft series) -definition: premature fusion of 1 or more cranial sutures -restricts skull growth in one direction -you get compensatory growth in the direction that is perpendicular to the fused suture -result: a very bizarre looking skull -may need surgery to ensure that the brain development is not restricted -simple: affects 1 suture -complex: affects >1 sutures |
|
|
What is trigonocephaly? |
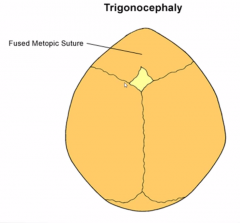
-5% of total deformity -premature fusion of the metopic suture -skull expands parallel to the direction of the suture -strange triangular appearance -can draw the eyes close together |
|
|
What is scaphocephaly? |
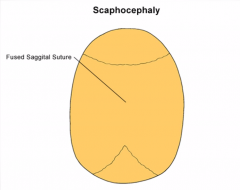
-fusion of sagittal suture -most common type of craniosynostosis -restricts lateral growth of skull, so increased AP growth -result: narrow elongated skull (boat-shaped) |
|
|
What is plagiocephaly? |
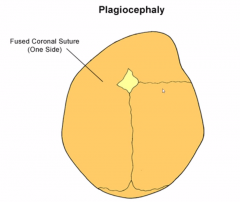
-when you have early fusion of one of the coronal sutures -you have an assymmetrical growth -causes restriction on fused side -compensation: growth more on the opposite side -can also happen in the back (lamboid suture) |
|
|
What is brachycephaly? |
Opposite of scaphycephaly. You have fused coronal sutures on both sides. AP growth restriction, so increase in lateral growth - round skull is the end result. You also get retrusion of the forehead Can be Associated with: -cruzon syndrome -alpert syndrome -carpenter syndrome (rare genetic syndromes) |
|
|
What is the management of brachycephaly? |
-complex -if not bad, can be left (only small aesthestic issue) -if it is raising the ICP, then max-fax operate -if growth restriction affects forehead: FRONTO-ORBITAL advancement, where they cut through the skull at the level of suture and orbit, take block out and move it forward, so skull can continue to grow |
|
|
Management of scaphocephaly? |
Reopen the suture so that they can continue to grow normally |
|
|
How do the muscles of facial expression develop? |
-all the facial muscles originate from the SECOND PHARYNGEAL arch -all are innervated by CN VII (facial nerve) so unilateral facial nerve palsy affects all the muscles |
|
|
How do you classify the muscles of facial expression? |
-can classify them into 3 groups. 1. Superiorly - ORBITAL GROUP 2. Nose - NASAL 3. Mouth - ORAL 42 muscles in total |
|
|
What is the orbital group made up of? |
1. orbicularis oculi: has 2 parts -inner palpebral part -outer orbital part -both work together to work the eyelids 2. Corrugator Supercilii -above and behind OO -contract to draw the eyebrows together |
|
|
What is the nasal group made up of? |
1. Nasalis -has 2 parts: transverse and alar -transverse part compresses nostrils -alar part opens nostrils 2. Procerus -above nasalis -pulls eyebrows downwards -works together with CS 3. Depressor septi nasi -pulls nose inferiorly which can open the nostrils |
|
|
What is the oral group made up of? |
1. Orbicularis Oris -surrounds the mouth -purses the lip when contracts 2. buccinator -deep to the other facial muscles -pulls cheek inwards, which prevents buildup of food in the mouth |
|
|
What are the symptoms of facial nerve paralysis? |
-important signs: lose forehead wrinkles, lower lid (ectropion) -cant smile normally |
|
|
Whats the most common cause of CN VII palsy? |
-Bell's palsy -Lower motor neuron lesion -unknown cause, can be viral origin -given steroids, dont know how it works -usually resolves without meds in 3-6 months DDx: Stroke - upper motor neuron lesion. Always look at the forehead - if they have stroke, forehead is SPARED |
|
|
How do you classify head and neck cancers? |
-complex cancers because of difficult anatomy -can break down cancer based on region 1. oral cancer 2. pharyngeal: naso- and oro- 3. Laryngeal |
|
|
How do you manage Head and neck cancers ? |
chemotherapy Radiotherapy Surgery Usually diagnosis is late, so palliative care is often the solution |
|
|
What is oral cancer made up of? |
90% squamous cell carcinoma |
|
|
Which organ is most involved in oral cancer? |
50% is tongue (lateral surface) -usually painless -late stage - invades the lingual nerve, so can cause pain |
|
|
What are the risk factors and prevalence of oral cancer? |
-it is associated with smoking, alcohol and HPV virus -high prevalence in the Indian subcontinent - because of chewing betel nut and tobacco |
|
|
What is the usual treatment for Oral cancer? |
Usually treated with a combination of surgery +/- radiotherapy +/- chemotherapy (glossectemy = removal of tongue) -lymph node dissection also key |
|
|
What is the anatomy of the oral cavity? |
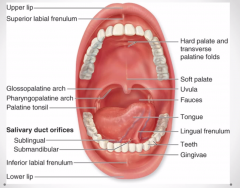
-tongue -soft palate -tonsils -2 fauces on either side (like pillars) |
|
|
What is a free fibula flap? |
-used in advanced head and neck cancers -used to reconstruct the mandible, a flap of tissue is taken from the fibula -fibula + skin island + cuff of muscle + peroneal artery and vein |
|
|
what is pharyngeal cancer? |
-can be divided into naso-, oro- |
|
|
what is the histology of Oropharynx cancer? |
-75% squamous cell, rest are lymphoma |
|
|
Where is the common site for oro-pharynx cancer? |
-Tonsils and the Faucial pillars |
|
|
What is oropharynx cancer usually associated with ? |
Smoking/HPV |
|
|
What are symptoms of Oropharynx cancer? |
-throat pain -globus sensation (sensation of something in the throat) |
|
|
What is the treatment for oropharynx cancer? |
Radiotherapy +/- chemotherapy If there are neck node metastases, then only is surgery done |
|
|
What is the histology of nasopharynx cancer? |
Mostly squamous cell carcinoma |
|
|
What are risk factors of nasopharynx cancer? |
-chinese descent -EBV |
|
|
Where is the highest incidence of nasopharynx cancer? |
SOUTHEAST asia (china, Hong kong, taiwan, malaysia) |
|
|
What are symptoms of nasopharynx cancer? |
-can cause facial pain (CN V) because it can invade through the foramen ovale |
|
|
What is treatment of nasopharynx cancer? |
-Radiotherapy mainly -survival rate (if the cancer has a protracted course) is 60-80% in 5 years (decent cancer) |
|
|
What is FNE? |
Fine nasal endoscopy |
|
|
What is the histology of laryngeal cancer? |
Mostly squamous cell |
|
|
Which organs are affected in laryngeal cancer? |
-supraglottis -glottis -subglottis |
|
|
What is the most common symptom of laryngeal cancer? |
-glottic cancer - early presentation because of dysphonia (Hoarse voice) so early Dx and better outcomes -supraglottic cancer - tends not to affect voice and can grow to large size before causing DYSPHAGIA (bad outcomes) -subglottic cancer - RARE but similar presentation to supraglottic cancer |
|
|
What is the anatomy of the larynx? |
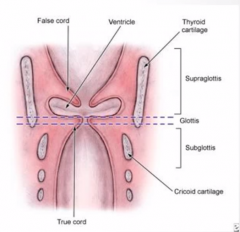
Divide into 3 parts: -supraglottis is above the level of true vocal cord -glottis is on the level of the true vocal cord -subglottis is on the level before the true vocal cord |
|
|
Why has the incidence of laryngeal cancer fallen since the 1990s? |
because less men have smoked since 1990 -LARYNGEAL CANCERS HEAVILY LINKED TO SMOKING |
|
|
What is the incidence of supraglottic cancer? |
40% |
|
|
What is the presentation of supraglottic cancer? |
-dysphagia -metastatic neck node -late presentation is common |
|
|
How do you manage supraglottic cancer? |
-Supraglottic laryngectomy + radiotherapy -do only a total laryngectomy if there is residual/recurrent disease (or metastatic neck nodes) |
|
|
How common is glottic cancer? |
60% |
|
|
What is the symptom of glottic cancer? |
Dysphonia - usually an early presentation |
|
|
What is the management of glottic cancer? |
-Radiotherapy for early tumours (there is a 95% cure rate for T1 lesions) -total laryngectomy and neck dissection for tumours which are residual or recurrent |
|
|
What is the most important thing to remember in facial traumas? |
-AIRWAY management -if they have facial trauma, then they probably have fractures/injuries elsewhere |
|
|
How are facial traumas divided? |
-upper 1/3: frontal -middle 1/3: small facial bones -lower 1/3: mandible |
|
|
What are orbital rim fractures? |
-normally occur at suture lines (weakest point) -superior orbital rim is the STRONGEST |
|
|
What are the bones forming the orbital rim? |
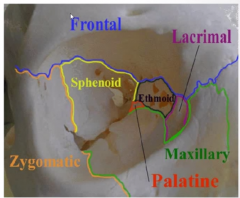
frontal - upper eyebrow zygomatic - side maxilla - underneath + floor side - lacrimal/ethmoid/palatine Sphenoid - back |
|
|
How can you test for the fracture of the zygomatic arch? |
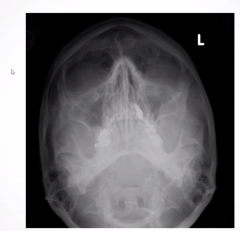
-trace down elephant's line on the side of an XRAY |
|
|
What is an orbital blowout fracture? |
-when there is raised pressure intraorbital -usually from something flying at the eye -partial HERNIATION of the orbital contents through the weakest part of the cavity (usually FLOOR) -fat and blood usually spill out into the maxillary sinus -also entrapment of the inferior rectus muscle (enables eye to look downwards) so paralysis of upward gaze, so inferior rectus is permanent contraction |
|
|
How are maxillary fractures classified ? |

-Le Fort classification -all need surgical management |
|
|
What is Le Fort type 1? |
horizontal fracture that separates teeth from upper face (fracture passes from the inferior alveolar ridge to below the maxillary sinus) (floating palate) - so teeth moves separate to the nose |
|
|
What is Le Fort type 2? |
base of pyramid - alveolar ridge apex - nasofrontal suture -floating nose and palate |
|
|
Le fort 3? |
Most severe type of fracture -fracture line all the way across separating the viscerocranium from neurocranium |
|
|
What are the major incidences of mandibular fractures? |
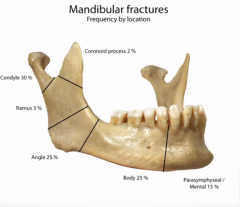
-Most common place is usually the left side of the mandible (left body) WHY? most people are right-handed so puncture left side of mandible -condyles, body and angle are most common -ramus and coronoid process are rare |
|
|
What percentage are bifocal in mandibular fractures? |
60% Why? because the mandible is a BONY ring |
|
|
What are the symptoms of mandibular fractures? |
-Trismus (because of spasm of temporalis) -malocclusion (cant bite cos of malalignment of maxilla and mandible) -paresthesia to the chin (disruption to the inferior alveolar nerve) |
|
|
Anatomy of the maxilla and mandible (sagittal view) |
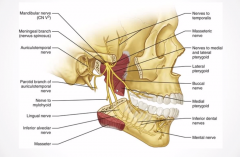
inferior alveolar nerve (V3 branch) enters the mandible, travels through the bone and emerges through the mental foramen to become the mental nerve (which supplies the lower lip) |
|
|
How easy is it to get a frontal bone fracture? |
NOT EASY need 100-200x force of gravity |
|
|
What are the symptoms of frontal bone fractures? |
-forehead paresthesia (because of disruption of supraorbital nerve) -Rhinorrhea ( runny nose, but actually it is CSF leak) |