Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
104 Cards in this Set
- Front
- Back
|
How many skeletal muscles are in the body?
|
400 skeletal muscles
Constitute 40 - 50% of total body weight. |
|
|
Muscles that decrease joint angles are called?
|
Flexors
|
|
|
Muscles that increase joint angles are called
|
Extensors
|
|
|
What are the characteristics of Type IIa muscle fibers?
|
*Moderate numbers of mitochondria
*Moderate resistance to fatigue *Combination of aerobic and anaerobic *Intermediate speed between Type IIb and Type I *Very adaptable |
|
|
What are the characteristics fo Type IIb muscle fibers?
|
*Fast Glycolytic fibers
*Small number of mitochondria but a large capacity of glycotic enzymes *Less resistant to fatigue *Energy system is anaerobic *Vmax is the highest *Efficiency is low |
|
|
Other characteristics of muscle fiber types.
|
Slow fatigue resistant fibers (Type I) develop tension slowly.
Slow fatigue resistant fibers(Type I) maintain tension for long periods. Fast fatigable fibers (Type II) develop tension rapidly. |
|
|
Characteristics of Fiber Types and Performance
|
No apparent age or sex differences in fiber distribution.
Average sedentary man has 47-53% slow fibers. Successful power athletes have more fast fibers. Endurance athletes have more slow fibers. Training can result in shift in fiber type. from fast fibers to slow fibers. |
|
|
Age related muscle changes
|
Slow phase - 10% loss from age 25-50
Rapid phase - 40% loss from age 50-80 Aging results in loss of fast fibers Primary loss of muscle mass is due to inactivity. |
|
|
What are the types of muscle contractions?
|
Isometric or Static
Isotonic or Dynamic Concentric = muscle shortening Eccentric = muscle lengthening |
|
|
What are the types of injury and regeneration of nervous system as it supplies the muscle.
|
Ablation - cut into or severed
Constricted - crushed without severing Compromised - by immunological or vascular disease |
|
|
What is orthograde degeneration?
|
When the axon is severed and the distal portion of the nerve is removed from nourishment.
|
|
|
What is retrograde degeneration?
|
The cell body changes after damage. Includes the reorganization of the rough endoplasmic reticulum - chromatolysis
|
|
|
What is the three stages of muscle dennervation?
|
Fasciculation, Fibrillation then Atrophy
|
|
|
What is fasciculation?
|
Action potentials at the site of lesion due to depolarization.
Earliest objective sign of muscle dennervation. |
|
|
What is fibrillation?
|
Uncoordinated contractions not visible to naked eye
|
|
|
Types of Muscular Dystrophies
|
DuChanne's - incompatible with adulthood.
Becker's - compatible with adult life. Treatment used in past was to the cut the Achilles tendon. |
|
|
Hip Dysfunction
|
It is the direct cause of lower back pain in 20% of low back syndromes.
|
|
|
Trendelenburg Sign
|
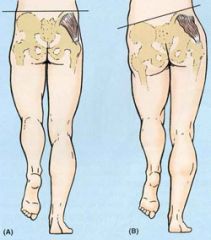
Test to determine the strength of the gluteus medius.. Compensated hip hike - use the weight of your torso to swing your leg thru gait.
Uncompensated hip hike - lift the opposite stance leg (Head Bobs) |
|
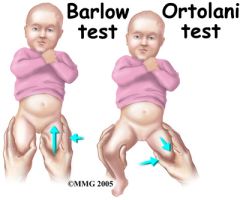
Ortolani's Hip Click Test
|
Performed on new born babies to detect hip dysplasia. Lazy parent treatment is swaddling.
|
|
|
Three cardinal signs of Degenerative Joint Dysplasia - radiological
|
Sclerosis - increased thickeneing of bone in joint
Loss of joint space. Osteophyte production (bone spur) |
|
|
Hip Fractures
|
20% of persons with hip fracture die within a year from factors directly related to these fractures.
|
|
|
Legg Calve Perthe's Disease
|
Self limiting hip disorder cased by a varying degree of ischemia and subsequent necrosis of the femoral head.
Blood supply to the epiphysis is thought to be the essential lesion. |
|
|
SCFE- Slipped Capital Femoral Epiphysis
|
The head of the femur stays in the cup of the hip joint while the rest of the femur is shifted. A change in their gait as they try to put as little weight as possible on the affected side. Occurs most often in adolescent males that are overweight, 13-15 .
|
|
|
Laseque's Differential Test
|
Helps differentiate hip pathology that could result in sciatic like pain from pain of discal origin or nerve root tension. If you suspect this, stop exam and take x-ray
|
|
|
Hip Rotation Test
|
The leg that is externally rotated returns short or the same length = short internal rotators.
The leg that is internally rotated returns long or the same length = short external rotators. Pain on return from abduction in either external or internal rotation = pathology of the hip joint, to include joint dysfunction, osteroarthritis. Note: shortened internal or external rotators can be due to altered pelvic, foot or ankle mechanics. |
|
|
Innominate
|
Nameless
|
|
|
Acetabulum
|
formed by three bones.
|
|
|
Femur
|
The longest bone in the body and articulates with the acetabulum
|
|
|
Classification of bone
|
Cortical- comapct- very dense
Cancellous- trabecular |
|
|
Paresis
|
Voluntary muscle weakness
|
|
|
Plegia
|
Complete loss of motor control
|
|
|
Cervical Transection
|
Affects all four extremities - quadriplegia
|
|
|
Lesions below the cervical enlargement
|
Paraplegia - lower extremeites
|
|
|
Muscles of the Hamstring include
|
Semimebranosis
Semitendonosis Adductor Magnus |
|
|
Counternutated Posture
|
Instablility created by excessive hamstring tightness.
Posture is hypolordotic. Tall and thin. Male >> female. Muscle shortness: Hamstrings, Adductors Prone to disc herniation |
|
|
Nutated Posture
|
Excessive stability but possible facet impringement.
Posture - hyperlordotic. Females >> Males Muscle shortness: iliopsoas and external rotators. |
|
|
Piriformis Syndrome
|
Often misdiagnosed: Its known to mimic other problems such as disc herniations, which also presnt with leg pain.
Pain and parathesias may be reported in the low back, groin, buttock, hip, posterior thigh, leg and foot. Pain can be deep seated and the patient may perceive pain in the rectum. Symptoms may be aggravated by sitting for long periods, running, driving a car for long periods of time, not properly stretching before and after activity, or from lifting in an awkward position. |
|
|
Piriformis Syndrome II
|
Affected leg is often exernally rotated when relaxed,
Some re[ports suggest a 6:1 female to male perdominance The leg doen't necessarily have to have been externally rotated for a long time - piriformis syndrome may be a result of faulty foot or spinal mechanics, gait disturbances, poor postures or sitting habits or any other factor that could cause that muscle to function abnormally. |
|
|
The axial skeleton consists of:
|
Cranium
Vertebral column Ribs Sternum |
|
|
Central Nervous System
|
Brain, brain stem, spinal cord
|
|
|
Peripheral nervous System
|
Cranial nerves: come directly off the brain/brain stem (12 pairs)
Spinal nerves: come off the cord (31 pairs) |
|
|
What are the symptoms of disc herniation?
|
Disruption of motor functions.
Numbness , asnesthia or parathesias. |
|
|
What does the Vertebral column consist of?
|
Consist of 33 vertebral segments:
7 Cervical 12 Thoracic 5 Lumbar 5 Sacral (fused) 4 Coccygeal (fused) |
|
|
What causes Scoliosis?
|
Lack of curves in sagittal plane combined with excessive flexibility can lead to Scoliosis.
|
|
|
What is Scoliosis?
|
A lateral deviation of the spine accounting for 80% of all types of scoliosis cases.
Must have lateral deviation of at least 10 - 15 degrees to be clinically significant. 8 to 9 degrees on the curve side of handiness is considered normal. |
|
|
What is the Ligamentum Flavum?
|
Originates on anterior surface of the lamina and inserts on the posterior surface of the lamina.
Also called the yellow ligament - lots of elastic connective tissue. Passive tension in these stretched ligaments limits flexion in the spinal column. Lies just posteior to the spinal cord. Hyperextension causes buckling of ligamentum flavum that can pinch the spinal cord. Thickening with age can also lead to spinal stenois. |
|
|
What are the pathomechanics of Spinal Stenosis?
|
Affects Middle Aged and Elderly population.
Pathomechanics - Entrapment of the Cauda Equina roots by hypertrophy of the osseous and soft tissue structures (ligamentum flavum) surrounding the lumbar spinal canal. |
|
|
What are the clinical manifestations of Spinal Stenosis?
|
Incapacitating pain in back and lower extermities.
Difficulting ambulating. Leg parasthesias and weakness. Severe cases - bowel and bladder disturbances. Neurogenic intermittent claudication |
|
|
What is the Anterior Longitudinal ligaments (ALL) relationship to the vertebral column?
|
Limits motion.
Anterior Longitundinal ligament - Long strap like structure that runs from the occiput to the anterior surface of all the vertebra including the Sacrum. Narrow at cephalic end (head) and widens caudally (tail). Blends with disc to help reinforce the fibers. --- The thickness of the ALL is the reason why disc herniations tend to be posterior by limiting extesion and excessive lordosis. |
|
|
What is the Posterior Longitundinal ligament (PLL) relationship to the vertebral column?
|
Maintains natural curvature
Indirectly protects the spinal cord. A continuious band of tissue that extends the entire length of the posterior surfaces of all vertrabrae for the axis tothe sacrum. Located within the vertebra canal- just anterior to the spinal cord. Also blends with and helps reinforce the IVD. Broad at the Cephalic end and narrows in the lumbar spine. The slender lumbar portion limits its ability to restrain a bulging slipped disc. |
|
|
What is Fibroadipose Meniscoids?
|
Located between the internal side of the capsule and the periphery of the articular cartilage.
Composed of small fat pads mixed with thin sheets of connective tissue. May help protect exposed cartilage and synovial membrane from compressive forces at the extermities of movement. Involved with Acute Locked Back condition. |
|
|
What is the Meniscoid Extrapment?
|
Upon flexion of the inferior articular process of a zygopophyseal joint moves upward taking a meniscoid with it.
Upon attempted extension, the interior articular process returns toward its neutral position, but the meniscoid, instead of re-entering the joint cavity, impacts against the edge of the articular cartilage, and buckles forming a space occupying lesion udner the capsule. Pain occurs as a result of capsular tension and extension is inhibited. Manipulation of the joint involving gapping and flexion reduces the impaction and opens the joint to encourage re-entry of the meniscoid into the joint space. |
|
|
When does cartilaginious degeneration begin?
|
Within 48 hours.
|
|
|
What is Spina Bifida?
|
The lack of joining of posterior arch in bone.
|
|
|
What are the characteristics of the Atlas?
|
Designed to support the weight of hte head.
Posses no body, pedicle, lamina or SP's. Essentially two lateral masses joined by anterior and posterior arches. Large convex facet accept the large condyles of the occiput. |
|
|
What are the characteristics of the Axis?
|
Large tall body with dens (remnant of the body of the atlas) projecting upward to articulate with the atlas.
Dens means rigid vertical axis of rotations. Bifid spinous peculiar to the axis - good reference point for palpation. |
|
|
What is Clay Shoveler's Fracture?
|
An oblique fracture of the SP of the lower cervical spine, typically C7, results from hyperflexion usually shoveling snow.
Originally named for those who mined clay. Stable fracture. |
|
|
What are the characteristics of the sacrum?
|
Triangular shaped bone with base and apex.
Transmits weight of vertebral column oto the pelvis. In childhood- 5 sacral vertebra fused in adult. Dorsal surface is convex- forms posterior wall of pelvic cavity. |
|
|
What are the characteristics of the Coccyx?
|
Small triangular bone consisting of 4 fused vertebra.
Forms sacrococcygeal joint with sacrum with fibrocartilagenous disc (amphiarthroisis)- fuses late in life. |
|
|
What is the Cauda Equina?
|
Spinal cord and vertebral column have different growth rates.
As a result, the spinal cord usually terminates adjacent to the IVF of L1-2. The lumbosacral nerves must travel a great distance to exit thier ivf's. This elongation resembles a horse's tail - hence Cauda Equina. Severe fracture or trauma of thelumbar spine can result inCaud Equina Syndrome (damage to nerve but sparing spinal cord): Muscle paralysis and atrophy Altered sensation - saddle numbness Reduced reflexes |
|
|
The Thoracic extension/lateral flexion/rotation is responsible for?
|
last 15 degrees of arm abduction.
|
|
|
As a general rule _________ facet surfaces favor ________ rotation, wheras _________ facet surfaces block ________ rotation.
|
horizontal, axial, vertical, axial
|
|
|
The structural arrangement of the annular rings resists:
|
Distraction (vertical separation)
Shear (sliding) Torsion (twisting) |
|
|
What is imbibition?
|
The process by which a fluid penetrates into a porous medium.
|
|
|
How does the the intervertebral disc handle load?
|
80% of the load across two lumbar vertebrae is carried through the interbody joint (disc).
The remaining 20% is carried by posterior structures, such as apophyseal joints and laminae. |
|
|
What causes disc height loss?
|
Not a consequence of aging - disc height maintained or actually increased.
|
|
|
Characteristics of disc heights
|
During bedrest disc pressure is low.
Low pressure and hydrophilic nature of the dis cause cause dis to swell- disc herniation patients have more pain in the morning. Weight bearing activities force water out of the disc- 1.1% variation in height during a single day. Water content: At birth - 88% 65-72% by age 75 less able to handle loads May lead to microfracture and bony resorption of the vertebral endplates - eventual widow's and dowager's hump. Lost of height with age with not a function of disc height - it is a function of bone loss. |
|
|
What is Down's Syndrome?
|
No Transverse ligament
Increased ADI |
|
|
Where does the rotation of the cervical spine occur?
|
About half the total rotation of the cervical spine (40-45 degrees) occurs at the atlanto-axial joint complex.
Flexion 5 degrees and extension 10 degrees. |
|
|
Motion of the Cervical Spine?
|
Flexion 40 -50 degrees
Extension 85 degrees Rotation 90 degrees Lateral Flexion 40 degrees |
|
|
What are the two most common examples of postural abnormalities of the Thoracic Spine?
|
Excessive Kyphosis and Sciolosis
The two most common conditions associated with kyphosis are Scheuermann's disease and osteoporosis. Scheueurmann's disease is also called Juvenile Kyphosis (5-8% of population). Onset, most often in early to mid adolsecence and most often in boys 13 -17 |
|
|
Scoliosis
|
Functional - can be corrected with active shift in posture
Structural- a fixed deformiity that can not be changed by posture. 80 - 90% idiopathic. Non-idiopathic: Congenital abnormalities Polio Muscular Dystrophy Spinal Cord injury Cerebral Palsy Trauma |
|
|
Thoracic Disc Prolapse
|
One-third associated with Trauma.
Pain can be mid=line, unilateral or bi-lateral, sensory disturbances, cold feet, weakness, tightness around chest or abdomen, bladder and bowl dysfunction, hyper-reflexia, spasticity and gait disturbances |
|
|
Maigne's Syndrome
|
Patients never complain of thoracolumbar pain.
|
|
|
Sacrum
|
The base of the sacrum is naturally inclined anteriorily and inferiorily, forming an approximate 40 degree sacrohorizontal (Ferguson's Sacral Base Angle) angle while standing.
Above 45 degrees = Hyperlordosis Below 40 degrees = Hypolordosis A typical sacral base angle of 40 degrees produces an anterior shear force at the L5-S1 junction equal to 64 % of superimposed body weight. |
|
|
Spondylolisthesis
|
Too much anterior shear force
|
|
|
Scotty Dog
|
The view of a the radiograph in patients that have Spondylolisthesis.
Definition- anterolisthesis typically of L5 on Sacrum with a break in the pars interarticularis |
|
|
Lytic (L5-S1)
|
Stress Fatigue fracture
Elongated but intact pars - repeated stress fracture of trabeculae Acute Fracture- rare- hyperextension injury |
|
|
Degenerative (L4-5)
|
Due to disc degeneration
|
|
|
Meyerding's Classification
|
Used to determine the severity of slippage
Up to 25% - Grade 1 26-50% - Grade 2 51-75% - Grade 3 - considered a surgical case if any further slippage occurs. 76 - 100% - Grade 4- considered a surgical case if any further slippage occurs in this stage Completely off sacrum - Grade 5 - surgury most likely due to the possibility of Cauda Equina Syndrome |
|
|
Single Photon Emission Computed Tomography (SPECT)
|
Provides bone scans - active or inactive
Not an MRI |
|
|
Lumbar Flexion
|
Relative to the neutral position, full felxion of the lumbar spine increases the diameter of the intervertebral foramina gy 19% and increases the volume of the vertebral canal by 11% - Good for Stenosis
|
|
|
Williams (Flex) exercises
|
Good for stenotic conditions but not Disc - look for centralization
|
|
|
Protusion
|
Displaced nucleus pulposus remains within the annulus but may create a pressure bulge on the spinal cord
|
|
|
Prolapse
|
Displaced nucleus pulposus reaches the posteior edge of the disc but remains confined within the outer layers of the annulus
|
|
|
Extrusion
|
Annulus fibrosis ruptures - allowing the nucleus pulposus to escape from the disc into the epidural space
|
|
|
Sequestration
|
Parts of the nucleus pulposus and fragments of annular material become lodged within the epidural space.
|
|
|
McKenzie exercises
|
Good for disc but not stenotic conditions
|
|
|
Illiopsoas
|
Consists of two muscles:
Iliacus Psoas Major |
|
|
Lumbar Rotation
|
Rotation is minimal only in lordotic state
Increases with flexed posture |
|
|
Lumbar Lateral Flexion
|
During lateral flexion:
In neutral or extension the spinous rotates toward the same side as Lateral Flexion. In flexion, the spinous rotates opposite the direction of Lateral Flexion (like cervicals) |
|
|
How does the Sacroiliac Joint change over time?
|
Between puberty and young adulthood, the sacroiliac joint gradually changes from a diarthrodial (synovial) joint to a modified amphiarthrodial (Cartilaginous-like the pubic symphysis) type of joint
|
|
|
Iliolumbar Ligament
|
Limits axial rotation and anterior glide of L5 on the sacrum
|
|
|
Sacrotuberous Ligament
|
Resists nutation which tightens the ligament. It also has an important connection to the long head of the biceps femoris.
|
|
|
Sacrospinal Ligament
|
Resists nutation which tightens the ligament. It also has an important connection to the long head of the biceps femoris.
|
|
|
Dorsal Sacral Iliac Ligament
|
This large ligament resists counter-nutation which tighens the ligament. It makes up 2/3 of the posterior SI connections and blends with the sacrospinal ligament, erector spinae and thoraolumbar fascia
|
|
|
Anterior Sacroiliac Ligament
|
Opposes axial translation of the sacrum and separation of the SI joints
|
|
|
Interosseous Ligament
|
Fills in the irregular spaces posterior and superior to the joint; resists joint separation
|
|
|
Functional Consideration of the SI Joint
|
Increased nutation during childbirth rotates the lower part of the sacrum posteriorly, thereby increasing the size of the pelvic outlet and favoring the passage of the infant
|
|
|
What is the close-packed position of the SI joint?
|
The close packed position of the sacroiliac joint is full nutation. Forces that create a nutation torque therefore stabilize the sacroiliac joint. Torques are created by the actions of gravity, stretched ligaments and muscle activation.
|
|
|
Clinical Consequences of Posterior Pelvic Tilt
|
Stiff hips
Hamstrings tight and short Excessive mobile lumbar spine Leads to early degeneration of hip and knees lumbar disc herniation |
|
|
Sacroiliac Syndrome
|
Acute low back pain
Typically unilateral Patient usually indicates the area of pain by placing their entire hand over the PSIS area therefore diffuse pain. If severely inflammed...can be very sharp and localized to the SI joint Worse in the AM and when sitting..and transitions...patient often gives history of having difficulty trying to find a comfortable position to sleep at night. |
|
|
Ankylosing Spondylitis
|
Decreased lumbar ROM
Paraspinal hypertonicity Flattened spinal curvatures Heel pain Pain and tenderness over bony protuberances Limited Chest Expansion Other organ systems affected like heart, great vessels, pulmonary, GI and GU systems |
|
|
Kidney Stones
|
Colic
Pain occurs suddenly Pain awakens patient at night Pain locailized to the flank. Pain associated with nausea and vomiting. Patient is constantly moving to find relief in contract to acute abdomen. |