![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
147 Cards in this Set
- Front
- Back
|
Atlanto-occipital articulation |
Flexion and extension |
|
|
Atlanto-axial articulation |
Rotation |
|
|
Articulations between C2 and S1 |
All the same (?) |
|
|
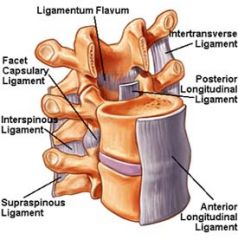
Anterior Longitudinal Ligament |
Tends to prevent excessive hyperextension - runs down the vertebral column on the anterior surface of the bodies - found in the thoracic and lumbar regions just deep to the aorta - Thin superiorly and thick inferiorly |
|
|
Posterior Longitudinal Ligament |
Prevents excessive flexion - runs along the vertebral bodies posteriorly, inside the vertebral foramen - thick superiorly, thin inferiorly (which increases disk injury in lumbar region) |
|
|
Supraspinal Ligament |
Extends from C7 distally to the sacrum posteriorly along the tips of the spinous processes |
|
|
Interspinal Ligament |
Runs between successive spinous processes |
|
|
Ligamentum Nuchae |
Very thick - takes the place of the Supraspinal and Interspinal ligaments in the cervical region |
|
|
Ligamentum Flavum |
Connects adjacent laminae anteriorly |
|
|
SCM Origin and Insertion |
O: Sternum and Clavicle I: Mastoid Process |
|
|
SCM Action and Innervation
|
A: Bilaterally - flexes neck, hyperextends head Unilaterally - Laterally bends the neck, rotates to the opposite side N: Accessory Nerve (Cranial Nerve XI); 2nd and 3rd cervical nerves |
|
|
Scalene Muscles Origin and Insertion |
O: Transverse Processes of the cervical vertebrae I: First and Second ribs |
|
|
Scalene Muscles Action and Innervation |
A: Bilaterally - assists in neck flexion Unilaterally - neck lateral bending N: Lower cervical nerves |
|
|
Erector Spinae Muscles Origin and Insertion |
O: Spinous processes, transverse processes, and posterior ribs from the occiput to the sacrum and ilium I: Spinous processes, transverse processes, and posterior ribs from the occiput to the sacrum and ilium |
|
|
Erector Spinae Muscles Action and Innervation |
A: Bilaterally - extend neck and trunk Unilaterally - laterally bend neck and trunk N: Spinal Nerves |
|
|
Transversospinalis Muscles Origin and Insertion |
O: Transverse Processes I: Spinous processes of vertebra above |
|
|
Transversospinalis Muscles Action and Innervation |
A: Bilaterally - extend neck and trunk Unilaterally - rotate neck and trunk to opposite side N: Spinal Nerves |
|
|
Splenius Capitis Muscles Origin and Insertion |
O: Lower half of nuchal ligament, spinous processes of C7 through T3 I: Lateral occipital bone, mastoid process |
|
|
Splenius Capitis Muscles Action and Innervation |
A: Bilaterally - extend head and neck Unilaterally - rotate and laterally bend the face to same side N: Middle and Lower Cervical Nerves |
|
|
Splenius Cervicis Muscles Origin and Insertion |
O: Spinous processes of T3 through T6 I: Transverse processes of C1 through C3 |
|
|
Splenius Cervicis Muscles Action and Innervation |
A: Bilaterally - extend neck Unilaterally - rotate and laterally bend the neck to the same side N: Middle and Lower Cervical Nerves |
|
|
Rectus Abdominis Muscles Origin and Insertion |
O: Pubis I: Xiphoid process and costal cartilages of 5th, 6th, and 7th ribs |
|
|
Rectus Abdominis Muscles Action and Innervation |
A: Trunk flexion, compression of abdomen N: 7th through 12th intercostal nerves |
|
|
External Oblique Muscle Origin and Insertion |
O: Lower 8 ribs laterally I: Iliac crest and linea alba |
|
|
External Oblique Muscle Action and Innervation |
A: Bilaterally - trunk flexion, compression of abdomen Unilaterally - lateral bending, rotation to opposite side N: 8th through 12th intercostal, iliohypogastric, and ilioinguinal nerves |
|
|
Internal Oblique Muscle Origin and Insertion |
O: Inguinal ligament, iliac crest, thoracolumbar fascia I: 10th, 11th, and 12th ribs - abdominal aponeurosis |
|
|
Internal Oblique Muscle Action and Innervation |
A: Bilaterally - trunk flexion, compression of abdomen Unilaterally - lateral bending, rotation to same side N: 8th through 12th intercostal, iliohypogastric, and ilioinguinal nerves |
|
|
Transverse Abdominis Muscle Origin and Insertion |
O: Inguinal ligament, iliac crest, thoracolumbar fascia, and last 6 ribs I: abdominal aponeurosis and linea alba |
|
|
Transverse Abdominis Muscle Action and Innervation |
A: Compression of abdomen N: 7th through 12th intercostal, iliohypogastric, and ilioinguinal nerves |
|
|
Quadratus Lumborum Muscle Origin and Insertion |
O: Iliac Crest
I: 12th rib, transverse processes of all 5 lumbar vertebrae |
|
|
Quadratus Lumborum Muscle Action and Innervation |
A: Trunk lateral bending N: 12th Thoracic and 1st lumbar nerves |
|
|
Motions available in the TMJ |
Mandibular depression, elevation, lateral deviation, protrusion, and retrusion |
|
|
Temporalis Muscle Action |
Bilaterally - elevation, retrusion (posterior fibers) Unilaterally - ipsilateral lateral deviation |
|
|
Masseter Muscle Action |
Bilaterally - elevation Unilaterally - ipsilateral lateral deviation |
|
|
Medial Pterygoid Muscle Action |
Bilaterally - elevation and protrusion Unilaterally - contralateral lateral deviation |
|
|
Lateral Pterygoid Muscle Action |
Bilaterally - depression and protrusion Unilaterally - contralateral lateral deviation |
|
|
Levator Palpebrae Action |
Elevate the eyelid (open the eyes) |
|
|
Orbicularis Oculi Action |
Circular muscle around the eye - closes the eye |
|
|
Corrugator Supercilii Action |
Draws the eyebrows down and medially (frowning) |
|
|
Occipitofrontalis Action |
Scalp down the front of the forehead - raises the eyebrows to wrinkle the forehead |
|
|
Procerus Action |
Wrinkles the nose (expressing distaste) |
|
|
Orbicularis Oris Action |
Encircles the mouth - purses the lips (kissing) |
|
|
Buccinator Action |
Positioning food in the mouth and blowing air out (like blowing up a balloon) |
|
|
Zygomaticus major Action |
Smile! Draws angles of the mouth upward and laterally |
|
|
Mentalis Action |
Protrudes the lower lip (pouting) |
|
|
Depressor Labii Inferior Action |
Draws the lower lip down and laterally (frowning) |
|
|
Biceps Reflex |
Tells you something about the integrity of the nervous system - nerve that innervates the bicep (C5) - one piece of the puzzle |
|
|
Brachioradialis Reflex |
Tells us something about C6 |
|
|
Triceps Reflex |
Tells us something about C7 |
|
|
Tinel Sign |
Designed to illicit pain/tenderness along the nerve (tap along the path of the nerve - symptoms better, worse, or the same - hurts worse is a + Tinel sign... same is - Tinel sign) |
|
|
Neurological Level tests C5 |
Motor: deltoid Reflex: biceps Sensation: lateral upper arm |
|
|
Neurological Level tests C6 |
Motor: Biceps/Wrist Extensors Reflex: Brachioradialis Sensation: Lateral lwer arm, thumb, index finger |
|
|
Compression of Cervical Spine |
Will reduce pain if nerve is compressed - if head tilted, called spurlings test |
|
|
Valsalva Test |
Will increase pain if pt has a disc problem |
|
|
Adson Test |
used to asses subclavian artery as in thoracic outlet syndrome - take pt's radial pulse and as you continue to feel the pulse, abduct, extend, and laterally rotate the arm - then instruct the person to take a deep breath and turn their head toward the arm being examined - if there is compression of the subclavian artery, there will be a significant decrease in the strength of the pulse |
|
|
Neurological control test for upper extremities |
pt stands with arms flexed to 90 degrees with eyes closed - pt is asked to hold this position for 30 seconds - examiner notes drifts outward or downward which may indicate a brain lesion |
|
|
Romberg Test |
pt asked to stand with feet together, arms at side with eyes open - assess balance, then ask pt to close eyes for at least 20 seconds (some suggest 60) - note any balance problems. + = pat sways excessively or falls to one side - a true + Romberg is when the pt falls or loses their balance - suggest a possible lesion involving peripheral nerves or conditions affecting the dorsal columns of the spinal cord |
|
|
Finger-to-nose test |
pt stands or sits with eyes open and is asked to bring the index finger to the nose - test is repeated with eyes closed - repeat several times and at increasing speed |
|
|
Finger-to-thumb test |
oppose each finger to thumb on each hand |
|
|
Hand flip test |
alternately touch back of stationary hand with front and back of test hand fingers |
|
|
Heel-to-knee test |
Heel to opposite knee and down to floor |
|
|
Proprioceptive Movement test |
if pt has the ability to know where their limb is or whether it's moving |
|
|
Proprioceptive position in space test |
if pt has the ability to know where their limb is or whether it's moving |
|
|
Thomas test |
Pt supine near the end of table, flex knees, flatten back and then extend hip so that leg lies flat - tight hip flexors if cannot let legs, lie flat down against table |
|
|
Ober Test |
test for tight TFL - side lying and let test leg adduct down to other leg |
|
|
Drawer's Sign |
Supine with knees flexed and resting on table - test for cruciates (ligamentous laxity) |
|
|
Lachman's Test |
Supine with one knee slightly flexed and resting in examiner's hands - test for cruciates |
|
|
Patellar Tendon Reflex |
Patellar deep tendon reflex (L4) |
|
|
McMurray's Test |
Test for meniscal problem in the knee - supine, flex hip and knee, palpate medially, rotate tibia externally on the femur and extend while applying a valgus stress - reverse for lateral meniscus |
|
|
Apprehension Test for Patellar Dislocation |
supine, attempt to move the patella laterally |
|
|
Patella Femoral grinding test |
supine, push patella distally and then have pt contract quads while providing resistance to the patella |
|
|
Ankle Reflex |
ankle jerk (S1) |
|
|
Neurological level tests L4 |
Motor: Tibialis Anterior (DF and INV) Reflex: Knee Jerk Sensation: Medial aspect of leg |
|
|
Babinski Sign |
Stimulate from heel laterally and across MT medially - positive = flare toes up negative = curl toes down - positive suggests an UMN lesion |
|
|
Straight Leg Raise test |
sciatic or nerve impingement in lower back - supine, relaxed, illicit pain on left side by raising left leg (passive - performed by examiner) - symptoms better, worse or the same - may cause "shooting pain" down the leg - don't confuse with tight hamstrings |
|
|
Test for Hamstring Tightness |
pt supine with hips flexed to 90 degrees and knees flexed fully as well with feet not touching the table - pt is asked to fully extend one knee as much as possible - if that same side knee is flexed more than 20 degrees, the hamstrings are considered tight |
|
|
Hoover Test |
Supine, cup under heels, have pt raise one leg - pt will always push down on other if really trying |
|
|
Patrick or Fabere's Test |
supine, test leg ER with foot resting on opposite knee - compress opposite pelvis and test medial aspect of knee - positive = problems with SI joint |
|
|
Distraction of Cervical Spine |
Trying to illicit any relief from a compressed nerve - slight retraction: better, worse or the same |
|
|
Neurological Level tests C7 |
motor: triceps reflex: triceps sensation: middle finger |
|
|
Neurological Level tests C8 |
motor: thumb extensors no reflex sensation: medial aspect of lower arm |
|
|
Neurological Level tests T1 |
motor: finger ABduction no reflex sensation: medial aspect of the elbow and upper arm |
|
|
Homan's Sign or Test |
To test for DVT - fully dorsiflex the pt's ankle with the knee extended - pain in the calf from this maneuver is a + Homan's sign - tenderness upon deep palpation of the calf muscle is further evidence of a DVT |
|
|
Sharp/Dull Sensation |
|
|
|
Light touch Sensation |
|
|
|
True Leg Length Discrepancy |
measure the distance from the left ASIS to the left medial malleolus and compare to the right side of same |
|
|
Valgus and Varus Stress at the Knee |
Valgus: Stress toward other knee (remember "Gum" - knees stick together) Varus: Stress away from opposite knee |
|
|
Phalen's Test |
to test for possible carpal tunnel syndrome - have pt flex both wrists and hold together for at least one minute to see if symptoms are reproduced |
|
|
Neurological control test for lower extremities |
pt sits with legs extended out in front without touching the ground - holds for 20-30 seconds - if drift is noted, suspect a brain lesion |
|
|
Neurological level tests L5 |
Motor: Extensor hallucis longus No reflex Sensation: Dorsum of foot |
|
|
Neurological level tests S1 |
Motor: Peroneals (Eversion) Reflex: ankle jerk Sensation: lateral aspect of foot and lower leg |
|
|
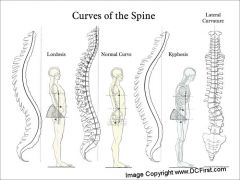
Importance of spine being curved instead of straight |
Provide the vertebral column with more strength and resilience - approx. 10X more than if it were straight |
|
|
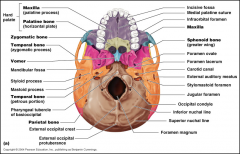
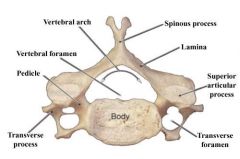
Identify:
|
|
|
|
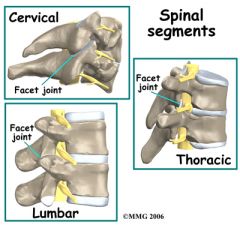
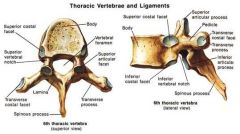
Identify:
|
|
|
|
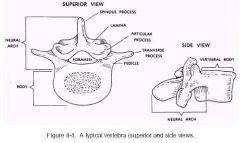
Identify:
|

|
|
|
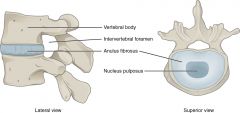
Identify:
|
|
|
|
Identify:
|
|
|
|
Atlas/Axis Landmarks and Characteristics |
|
|
|
C7 Landmarks and Characteristics |

|
|
|
Transverse Foramen (Cervical Vertebrae) |
|
|
|
Costal Facet (Thoracic Vertebrae) |
|
|
|
Ligaments of the spine:
|
|
|
|
Posture - Lateral View |
|
|
|
Posture - Anterior View |

|
|
|
Posture - Posterior View |

|
|
|
Spine
|
|
|
|
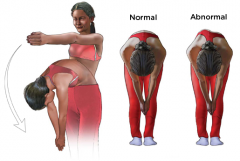
Scoliosis |

|
|
|
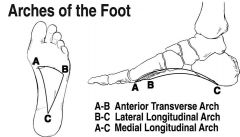
Longitudinal Arch of Foot |
|
|
|
Rib hump or spinal Rotation (Scoliosis) |
|
|
|
Genu Varus vs Genu Valgum |
|
|
|
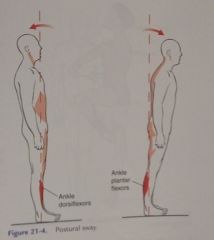
Postural sway (anteroposterior displacement of entire body) |
|
|
|
Muscles that control Lateral Pelvic Tilt |
Hip abductors (mainly the gluteus maximus and minimus), and the trunk lateral benders (erector spinae and quadratus lumborum) |
|
|
Antigravity muscles |
Neck flexors, neck and trunk extensors, trunk flexors, hip extensors, knee extensors |
|
|
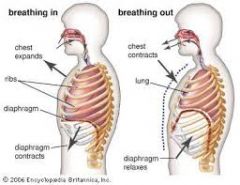
Function of the respiratory system |
Main function is to supply oxygen to and eliminate carbon dioxide from the lungs |
|
|
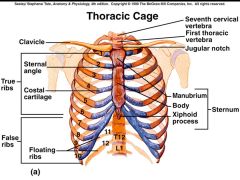
Thoracic Cage
|
|
|
|
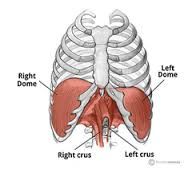
Diaphragm |
|
|
|
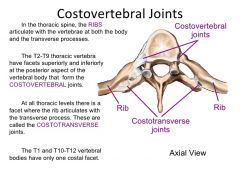
Costovertebral Articulations and Costal Facets |
|
|
|
Movement of the thoracic cage and inspiration/expiration |
|
|
|
Cervical Flexion (Goniometer) |
Axis: Ear Lobe Stationary Arm: Perpendicular to ceiling Moveable Arm: Parallel with base of nose Action: Chin to Chest |
|
|
Lateral Trunk Flexion (Goniometer) |
Axis: S2 Stationary Arm: Perpendicular to floor Moveable Arm: Along spinous processes, pointing toward C7 Action: Slide hand along thigh towards knee |
|
|
Trunk Flexion (Goniometer) |
Tape Measurer: C7 and S2 Action: Take initial measurement with pt standing. Have pt roll forward segmentally without bending at hips - take secondary measurement and subtract first. |
|
|
Cervical Rotation (Goniometer) |
Axis: Top of head Stationary Arm: Parallel with acromion processes Moveable Arm: parallel with nose Action: Pt turns head toward shoulder without rotating shoulders |
|
|
Trunk Extension (Goniometer) |
Tape Measurer: C7 and S2 Action: Take initial measurement with pt standing. Instruct pt to bend backwards without moving hips - take secondary measurement and subtract first. |
|
|
Trunk Rotation (Goniometer) |
Axis: Top of head Stationary Arm: Parallel with PSIS's Moveable Arm: Parallel with Acromion process Action: Pt crosses arms over chest and rotates body without lifting hips off table. |
|
|
Lateral Cervical Flexion (Goniometer) |
Axis: C7 Stationary Arm: Parallel to spinous processes, pointing toward S2 Moveable Arm: midline of skull Action: Pt moves ear toward shoulder on same side |
|
|
Cervical Extension (Goniometer) |
Axis: Ear Lobe Stationary Arm: Perpendicular to ceiling Moveable Arm: Parallel with base of nose Action: Look at ceiling |
|
|
Trunk Flexion (MMT) |
Position: Supine Action: Do a sit up - looking for inferior angle of scapula to leave table 5: Fingertips on ears, knees straight 4: Arms crossed over chest, knees straight 3: Arms down toward side, knees straight 2: Arms down toward side, knees bent 1: Cough |
|
|
Cervical Flexion (MMT) |
Position: Supine Action: Chin to chest, hold |
|
|
Trunk Rotation (MMT) |
Position: Supine Action: Bring arm toward opposite hip 5: Fingertips on ears, knees straight 4: Arms crossed over chest, knees straight 3: Arms down toward side, knees straight 2: Arms down toward side, knees bent 1: Palpation of obliques |
|
|
Cervical Extension (MMT) |
Position: Prone, head off table Action: Lift head up (make sure to provide support in case they are not a 5), hold |
|
|
Cervical Rotation (MMT) |
Position: Supine Action: Move head to both sides - have pt hold ear against bottom palm while you try to turn their head the opposite direction |
|
|
Trunk Extension (MMT) |
Position: Prone Action: Lift chest off table - looking for xiphoid process to come off table 5: Fingertips on ears 4: Hands on lumbar region of back 3: Hands on sacrum region of back 2: Hands down toward side 1: Palpate muscles |
|
|
Sore foot or Antalgic Gait |
Quick release - "Get off it" |
|
|
Weak Dorsiflexors |
Fairly flat foot - toe strike first - equins gait or slow drop foot |
|
|
Weak Plantarflexors |
No toe off phase, flat foot |
|
|
Weak Knee Extensors |
quads - lean forward, knee buckling swing phase - "slap" into extension |
|
|
Weak Hip Flexors |
Use whole body to swing through getting leg in front |
|
|
Weak Knee Flexors |
Hamstrings - knee hyperextends - can't slow down swing phase |
|
|
Weak Hip Extensors |
Glute Max gait - Trunk post rocking horse |
|
|
Weak Hip Abductors |
Glute med - trunk over affected side - trendelenburg |
|
|
Fused Ankle |
Zero movement in affected side - light weight on foot - short steps |
|
|
Fused Knee Joint |
Zero knee flexion/extension - vaulted on opposite side |
|
|
Plantarflexion Contracture |
Tip toe walking - knee could be bent |
|
|
Knee Flexion Contracture |
Knee stuck in flexion with more dorsiflexion or plantar flexion depending on how bad |
|
|
Leg length discrepancy |
Tip toe walking - non side bent compensating |
|
|
Hip Flexion Contracture |
Forward bent, walk on toe, knee bent |
|
|
Spastic Gait - LE are adducted and platarflexed (scissor gait) |
hip adductors are tight, bring foot across midline |