![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
183 Cards in this Set
- Front
- Back
- 3rd side (hint)
|
Affinity vs Avidity |
Affinity- Individual antibody-antigen interaction Avidity- Cumulative binding strength of all antibody-antigen interaction |
|
|
|
IgG |
1- Produce antibody in secondary response to antigen 2- most abounding isotype in serum 3- Fixed complement, Opsonization of bacteria and neutralization of bacterial toxins and virus 4- Only isotype that crosses the placenta |
|
|
|
IgA |
1- Prevent attachment of bacteria and virus to mucus membrane 2- Crosses epithelial cells by transcytosis 3- Produce in the GI tract( peyers patches) and protect against gut organism 4- Most abundantly produce isotype however low in the serum 5- Release in secretion(tears, saliva, mucus) and breast milk 6- Pick up secretary component from epithelial cell, protect Fc portion from luminal protease 7- Monomer in circular Dimer in secretion (J chain) |
|
|
|
IgM |
1- Produce antibody in primary response to antigen 2- Fixes complement 3- Does not bind to antigen while humoral response evolve |
|
|
|
IgE |
1- Bind to mast cells and basophils when exposed to allergen, mediate immediate hypersensitivity (type 1) through release of inflammatory mediators such as histamine 2- Contributes to immunity of parasites by activating eosinophils |
|
|
|
IgD |
1- Unclear function 2- Found in surface of many B cells and in serum |
|
|
|
What benefit is conferred by IgM assuming a pentameric configuration |
Increase ability to trap free antigen out of tissue while the humoral response is evolving |
|
|
|
Mature, naive B cells express what immunoglobulin isotype on their surface before class switching |
IgM IgD |
|
|
|
Which immunoglobulin isotypes are secreted by plasma cells |
IgG IgA IgE |
|
|
|
Immunoglobulin isotype differentiate in germinal centers of lymph nodes by which mechanism |
Isotype switching into plasma cells |
|
|
|
Name 2 molecules that induce gene rearrangement/Isotype switching |
Cytokines CD40L |
|
|
|
Which immunoglobulin isotypes are associated with cold and warm autoimmune hemolytic anemia |
IgM(cold) IgG(warm) |
|
|
|
Thymus independent antigen |
1- Lack peptide component 2- Cannot be presented by MHC to Th 3- Weak immunogenicity vaccine- often requires booster or adjuvant |
|
|
|
Thymus dependent antigen |
1- Contain protein component 2- Class switching and immunological memory occur as a result of direct contact of B cell with Th cel |
|
|
|
What kind of antigen are lipopolysaccharides from gram-negative bacteria |
Thymus independent antigen that lack a peptide component |
|
|
|
Complement proteins |
Hepatically synthesized plasma proteins that plays a role in innate immunity and inflammation |
|
|
|
Function of C3b , (C3a, C4a, C5a), C5a and C5b-9 |
C3b- opsonization C3a, C4a, C5a- anaphylaxis C5a- neutrophil chemotaxis C5b-9- cytolysis (MAC) |
|
|
|
Function of membrane attract complex |
C5b-9 Defends against gram negative bacteria |
|
|
|
Opsonization |
1- Prepare for eating 2- C3b and IgG 3- Enhance phagocytosis 4- C3b also help to clear immune complex 5- C3b binds to lipopolysaccharides on bacteria |
|
|
|
Inhibitors of complement protein |
1- Decay accelerating factor (DAF)- CD55 2- C1 esterase inhibitor Help prevent complement activation in self cells eg RBC |
|
|
|
Activation pathways |
1- Classical pathway - 1- antigen-antibody complex 2- IgG and IgM 2- Alternative pathway - Microbes surface molecules 3- Lectin pathway- sugar on microbe surface |
|
|
|
Function of CH50 in classical pathway |
Screen for activation |
|
|
|
Alternative pathway from C3 all the way to the cleavage of C5 |
1- C3 cleaves into C3b 2- C3b + Bb - C3bBb (C3 convertase) 3- Cleaves C3 into C3a/b 4- C3bBb + C3b- C3bBb3b (C5 convertase) 5- Cleaves C5 into C5a/b |
|
|
|
Lectin pathway to C5 cleavage |
1- Microbial surface 2- C1 like complex 3- Cleaved C4 into C4a/b 4- C4b+ C2b - C4b2b (C3 convertase) 5- Cleaves C3 into C3a/C3b 6- Increase C4b2b3b (C5 convertase) 7- Cleaved C5 into C5a/C5b |
|
|
|
2 complexes that can act as C5 convertase in the complement system to cleave C5 into C5b |
C3bBb3b (alternative pathway) C4b2b3b (classic/Lectin pathway) |
|
|
|
C3 convertase in different pathways |
C3bBb - Alternative pathway C4b2b- classic/Lectin pathway |
|
|
|
Complement protein deficiency |
1- Early complement protein deficiency (C1-C4) 2- Terminal complementary protein deficiency (C5-C9) |
|
|
|
Early complement deficiency (C1-C4) |
1- Increase risk of severe, recurrent pyogenic sinus and respiratory tract infection 2- Increase risk of SLE |
|
|
|
Terminal complement deficiency (C5-C9) |
Increase susceptible to recurrent Nesseria bacteremia |
|
|
|
Complementary regulatory protein deficiency |
1- C1 esterase inhibitor deficiency 2- Paroxysmal nocturnal hemoglobinuria |
|
|
|
C1 esterase inhibitor deficiency |
1- Hereditary angioedema due to unregulated activation of kallikrein- increase basophils 2- Characterized by decrease C4 levels 3- ACE inhibitors contraindicated |
|
|
|
Paroxysmal nocturnal hemoglobinuria |
1- Defect of PIGA prevent formation of GP1 anchor protein for complement inhibition eg decay- accelerating factor (DAF/CD55) or Membrane inhibitor of reactive lysis (MIRL/CD59) 2- Cause complement mediated inyravasculat hemolysis 3- Decrease heptoglobulin red urine 4- Triad 1- Coombs negative hemolytic anemia 2- Venous thrombosis 3- Pancytopenia 5- Treatment- Eculizmab |
|
|
|
How does complement deficiencies (C1-C4) increase the risk of SLE |
Reduce clearance of antigen antibody complexes due to lack of C3b |
|
|
|
4 examples of atypical venous thrombosis that can occur in paraoxysmal nocturnal hemoglobinuria |
Budd- Chiari syndrome Cerebral thrombosis Dermal thrombosis Portal vein thrombosis |
|
|
|
Interleukin 1 |
1- Cause fever and active inflammation 2- Activate endothelium to express adhesive molecules 3- Induce chemokine secretion to recruit WBC 4- Also called osteoclasts activating factor |
|
|
|
Interleukin 2 |
stimulate T cell production |
|
|
|
Interleukin 3 |
Stimulate bone marrow |
|
|
|
Interleukin 4 |
1- Induce differentiation of th2 cells 2- Promote growth of B cells 3- Enhance class switching to IgE and IgG |
|
|
|
Interleukin 5 |
1- Promote the growth and differentiation of B cells 2- Promote growth and differentiation of eosinophils 3- Enhance class switch of IgA |
|
|
|
Interleukin 6 |
Stimulate active phase protein production |
|
|
|
Tumor necrosis factor |
1- Activate endothelium 2- Induces chemokine secretion to recruit WBC and vascular leaking 3- Causes cachexia in malignancy 4- Maintain granulomas in TB 5- Mediate fever and sepsis |
|
|
|
Interferon y |
1- Secreted by Nk cells and T cells in response to antigen or Il12 from macrophages 2- Inhibit the differentiation of TH2 3- Stimulate macrophages to kill phagocytic pathogen 4- Stimulate NK to kill virally infected cells 5- Stimulate macrophages to induce granuloma formation |
|
|
|
Interleukin 8 |
Chemotactic factor for neutrophils |
|
|
|
Interleukin 12 |
1- Induce differentiation of T cell in Th1 2- Activate Nk cells |
|
|
|
Interleukin 10 |
1- Attenuated inflammatory response 2- Decrease expression of MHC II and Th cytokines 3- Inhibit activated macrophages and dentritic cells 4- Secreted from regulatory T cells |
|
|
|
Which 2 cytokines have the same attenuating effect on the immune system |
Transforming growth factor - beta Interleukin 10 |
|
|
|
3 cytokines secreted by macrophage |
IL -1 IL -6 IL- 8 IL- 12 TNF - alpha |
|
|
|
What 2 types of immune cells secrete interleukin- 10 |
Regulatory T cells Th2 cells |
|
|
|
Which cells secrete interleukin 2 and interleukin 3 |
T cells |
|
|
|
What 2 cytokines function in the recruitment of immune cells after the initial phase of acute inflammation |
IL- 8 IL- 12 |
|
|
|
Interleukin 13 |
1- Promotes B cell mediated IgE production 2- Induce alternative activation of macrophages |
|
|
|
Respiratory burst |
1- Also called oxidative burst 2- Activation of the phagocyte NADPH oxidase complex (neutrophils and monocytes) which utilized O2 as a substrate 3- Plays an important role in immune response - rapid release of reactive oxygen species ROS 4- NADPH also play a role in both the creation and neutralization of ROS 5- Myeloperoxidase is a blue-green heme-contains pigment that gives sputum its color 6- Pyocyanin in P.aeruginosa generates ROS that kill competing pathogens 7- Oxidative burst also lead to K influx which release lysosomal enzymes |
|
|
|
Respiratory burst |
1- Also called oxidative burst 2- Activation of the phagocyte NADPH oxidase complex (neutrophils and monocytes) which utilized O2 as a substrate 3- Plays an important role in immune response - rapid release of reactive oxygen species ROS 4- NADPH also play a role in both the creation and neutralization of ROS 5- Myeloperoxidase is a blue-green heme-contains pigment that gives sputum its color 6- Pyocyanin in P.aeruginosa generates ROS that kill competing pathogens 7- Oxidative burst also lead to K influx which release lysosomal enzymes |
|
|
|
Lectoferrin |
Protein found in secretory fluids and neutrophils that inhibit microbial growth via iron chelation |
|
|
|
Chronic granulomatous disease |
1- Deficiency of NADPH oxidase 2- Patient with CGD utilize H2O2 from invading organism and convert them ROS 3- Increase risk of infection by catalase positive species (S. Aires, Aspergillosis) capable of neutralization their own H2O2 leaving phagocytes without ROS for fighting infection 4- Abnormal dihydrohodamine (flow cyometry) decrease green fluorescence Nitro blue tetrazolium dye reduction test fails to turn blue |
|
|
|
In what part of the phagocyte does respiratory burst occur |
Phagolysosome |
|
|
|
Which enzyme catalyzes the conversion of oxygen to superoxide in the first step of respiratory burst |
NADPH oxidase |
|
|
|
What end product of oxygen-dependent respiratory burst is used to kill bacteria in the phagolysosome |
Bleach HOCl (Hypochlorite) |
|
|
|
2 cells that utilize the phagocyte NADPH oxidase complex |
Neutrophils Monocytes |
|
|
|
Enzyme that catalyzes the conversion of superoxide into hydrogen peroxide in the second step of respiratory burst |
Superoxide dismutase |
|
|
|
Function of bacterial catalase enzyme in oxidative burst of H2O2 |
Form water and oxygen |
|
|
|
Function of myeloperoxidase in oxidative burst |
Formation of HOCL (hypochlorite free radial) by incorporating chloride with hydrogen peroxide |
|
|
|
Enzyme involved in the regeneration of NADPH from NAD |
Glucose 6 phosphate dehydrogenase (G6PD) |
|
|
|
Interferons alpha, beta and gamma |
1- Innate host defense 2- Interfere with both DNA and RNA 3- Cells that are infected with virus produces these glycoproteins which act in local cells 4- Priming them for vitral defense by downregulating protein synthesis to resist potential viral replication and up regulation of MHC expression to recognize infected cells 5- Plays a major role in activating anti-tumor immunity |
|
|
|
Uses of interferon alpha beta and gamma |
1- Chronic granulomatous disease 2- Chronic HBV 3- Condylomata acuminatum 4- Kaposi sarcoma 5- Renal cell carcinoma 6- Hairy cell leukemia 7- Malignant melanoma 8- Multiple sclerosis |
|
|
|
Adverse effect of interferon alpha beta and gamma |
1- Flu like symptoms 2- Depression 3- Neutropenia 4- Myopathy 5- Interferon induced autoimmunity |
|
|
|
Markers on all T cells |
TCR- (binds antigen-MHC complex ) CD 3- ( associated with TCR for signal transduction) CD28- (Binds B7 on APC) |
|
|
|
Helper T cells receptors |
CD4 CD40 CXCR4/CCR5 (co receptor HIV) |
|
|
|
Cytotoxic T cell receptor |
CD8 |
|
|
|
Regulatory T cell receptors |
CD 4 CD 25 |
|
|
|
B cell receptors |
1- Ig (binds antigen) 2- CD 19, 20, 21 (receptor for Epstein bait) 3- CD 40 4- MHC II 5- B7 |
|
|
|
B cell receptors |
1- Ig (binds antigen) 2- CD 19, 20, 21 (receptor for Epstein bait) 3- CD 40 4- MHC II 5- B7 |
|
|
|
Macrophage receptor |
1- CD 14 (receptor for PAMP eg LPS) 2- CD 40 3- CCR5 4- MHC II 5- B7 (CD80/86) 6- Fc and C3b (enhance phagocytosis) |
|
|
|
NK cell receptors |
CD16 (bind Fc of IgG) CD 56(suggestive marker) |
|
|
|
Hemoropoeitoc stem cells market |
CD 34 |
|
|
|
Anergy |
State during which a cell cannot be activated by exposure to its antigen |
|
|
|
In what situation do T and B cells become anergic |
Do not receive a costimulatory signal on exposure to an antigen |
|
|
|
Passive immunity |
1- Requiring preformed antibodies 2- Rapid 3- Short live antibody 4- Example 1- Ig A in break milk 2- IgG in placenta 3- Humanized monoclonal antibody 4- Antitoxin |
|
|
|
Active immunity |
1- Exposure to exogenous antigen 2- Slow 3- Long lasting protection (memory) 4- Example 1- natural infection 2- Vaciins 3- Toxoid |
|
|
|
Antibodies given in passive immunity |
1- Tetanus toxin 2- Botulinum 3- HBV 4- Varicella 5- Rabies 6- Diphtheria toxi |
To be healed very rapidly before dying |
|
|
Exposure to which 2 cities requires combined active and passive immunization |
HBV - hepatitis B virus Rabies virus |
|
|
|
Live attenuated vaccine |
1- Micro-organism losses it pathogenicity and is capable of transient growth in inoculated cells 2- Induce humoral and cellular response 3- Pros- Induced strong, life long immunity Cons 1- May revert to the virulent form 2- Contraindicated in pregnancy and immunodeficiency |
|
|
|
Examples of live attenuated vaccine |
1- Adenovirus 2- Typhoid (oral) 3- Poli (Sabin) 4- Varicella 5- Small pox 6- Yellow fever 7- BCG 8- Influenza (intranasal) 9- MMR 10- Rotavirus |
Attention teachers please vaccinate small young beautiful infants with MMR regularly |
|
|
Killed or inactivated vaccine |
1- Pathogens are inactivated by heat or chemical 2- Induce humoral response 3- Pro 1- Safer Cons 1- Weak immune response 2- Require booster |
|
|
|
Killed or inactivated vaccine |
1- Pathogens are inactivated by heat or chemical 2- Induce humoral response 3- Pro 1- Safer Cons 1- Weak immune response 2- Require booster |
|
|
|
Examples of killed or inactivated vaccine |
1- Hepatitis A 2- Typhoid (IM) 3- Rabies 4- Influenza 5- Polio (Salk) |
|
|
|
Killed or inactivated vaccine |
1- Pathogens are inactivated by heat or chemical 2- Induce humoral response 3- Pro 1- Safer Cons 1- Weak immune response 2- Require booster |
|
|
|
Examples of killed or inactivated vaccine |
1- Hepatitis A 2- Typhoid (IM) 3- Rabies 4- Influenza 5- Polio (Salk) |
|
|
|
Subunit vaccine |
1- Include only antigen that best stimulate the immune system 2- Pros 1- Decrease risk of adverse reaction Cons 1- weak immune response 2- Expensive |
|
|
|
Killed or inactivated vaccine |
1- Pathogens are inactivated by heat or chemical 2- Induce humoral response 3- Pro 1- Safer Cons 1- Weak immune response 2- Require booster |
|
|
|
Examples of killed or inactivated vaccine |
1- Hepatitis A 2- Typhoid (IM) 3- Rabies 4- Influenza 5- Polio (Salk) |
|
|
|
Subunit vaccine |
1- Include only antigen that best stimulate the immune system 2- Pros 1- Decrease risk of adverse reaction Cons 1- weak immune response 2- Expensive |
|
|
|
Example of subunit vaccine |
1- HBV 2- HPV (type 6,11, 16 and 18) 3- Steptococcus pneumonia 4- Neisseria meningitis 5- Hemophilus influenza type B 6- Acellular pertussis |
|
|
|
Killed or inactivated vaccine |
1- Pathogens are inactivated by heat or chemical 2- Induce humoral response 3- Pro 1- Safer Cons 1- Weak immune response 2- Require booster |
|
|
|
Examples of killed or inactivated vaccine |
1- Hepatitis A 2- Typhoid (IM) 3- Rabies 4- Influenza 5- Polio (Salk) |
|
|
|
Subunit vaccine |
1- Include only antigen that best stimulate the immune system 2- Pros 1- Decrease risk of adverse reaction Cons 1- weak immune response 2- Expensive |
|
|
|
Example of subunit vaccine |
1- HBV 2- HPV (type 6,11, 16 and 18) 3- Steptococcus pneumonia 4- Neisseria meningitis 5- Hemophilus influenza type B 6- Acellular pertussis |
|
|
|
Toxoid vaccine |
1- Denatured bacterial toxin with intact receptor binding site 2- Pros 1- Protects against bacterial toxins Cons 1- Require booster |
|
|
|
Killed or inactivated vaccine |
1- Pathogens are inactivated by heat or chemical 2- Induce humoral response 3- Pro 1- Safer Cons 1- Weak immune response 2- Require booster |
|
|
|
Examples of killed or inactivated vaccine |
1- Hepatitis A 2- Typhoid (IM) 3- Rabies 4- Influenza 5- Polio (Salk) |
|
|
|
Subunit vaccine |
1- Include only antigen that best stimulate the immune system 2- Pros 1- Decrease risk of adverse reaction Cons 1- weak immune response 2- Expensive |
|
|
|
Example of subunit vaccine |
1- HBV (HBsAg) 2- HPV (type 6,11, 16 and 18) 3- Steptococcus pneumonia 4- Neisseria meningitis 5- Hemophilus influenza type B 6- Acellular pertussis |
|
|
|
Toxoid vaccine |
1- Denatured bacterial toxin with intact receptor binding site 2- Stimulate the immune system to make antibodies without potentially causing a disease 3- Pros 1- Protects against bacterial toxins Cons 1- Require booster |
|
|
|
Example of toxois vaccine |
Clostridium tetani Corynebacterium diphtheria |
|
|
|
What are the 2 live attenuated vaccines that can be given to patients with HIV infection and a CD4 cell count of >200 cells/mm3 |
MMR Varicella |
|
|
|
Which live nonattenuated viral vaccine is only given to military recruits |
Adenovirus |
|
|
|
Which typhoid vaccine is capable of producing a stronger immune response |
Ty21 typhoid vaccine in live attenuated vaccine |
|
|
|
Which vaccine against salmonella typhi poses a lower risk of causing infection |
Intramuscular which is the killed/inactivated vaccine |
|
|
|
What are the 3 common mechanisms of type II hypersensitivity reaction |
Cell destruction Inflammation Cell dysfunction |
|
|
|
How does the immediate phase of type 1 hypersensitivity reaction take place |
1- Antigen cross-links IgE on the surface of presenting mast cells 2- Immediate degranulation 3- Release histamine, typtase and leukotrienes |
|
|
|
How do you test for type 1 hypersensitivity |
Skin test or blood test (ELISA) for allergen specific IgE |
|
|
|
What are the 4Ts associated with type 4 hypersensitivity reaction |
1- T cell 2- Transplant rejection 3- TB skin test 4- Touching (contact dermatitis) |
|
|
|
2 examples of type 4 hypersensitivity |
Graft vs host disease Contact dermatitis |
|
|
|
Direct Coombs test |
Detect antibodies directly bound to RBC |
|
|
|
Indirect Coombs test |
Detect antibodies unbound in the serum |
|
|
|
Mechanism of type 3 hypersensitivity |
1- Immune complex antigen-antibody complex activate complement 2- Neutrophil chemotaxis 3- Neutrophils release lysosomal enzymes |
|
|
|
Isotype most commonly form in type 3 hypersensitivity |
IgG |
|
|
|
What is the marker of mast cell activation during type 1 hypersensitivity reaction |
Release of tryptase following mast cell degranulation |
|
|
|
Examples of type 1 hypersensitivity |
Anaphylaxis Allergic asthma |
|
|
|
How does the late phase of type 1 hypersensitivity occurs |
Release of chemokine and other mediators from mast cell |
|
|
|
Cellular destruction in type 2 hypersensitivity |
Cell opsonized by antibody leading to either 1- Phagocytosis and/or activation of complement system 2- NK cell killing (antibody-dependent cellular cytotoxicity ) |
|
|
|
Inflammation in type 2 hypersensitivity reaction |
1- Binding of antibody to cell surface 2- Activation of complementary system and Fc receptor mediated inflammation |
|
|
|
Examples of cellular destruction in type 2 hypersensitivity reaction |
Hemolytic anemia of the newborn Immune thrombocytopenia Autoimmune hemolytic anemia Transfusion reaction |
|
|
|
Examples of cellular destruction in type 2 hypersensitivity reaction |
Hemolytic anemia of the newborn Immune thrombocytopenia Autoimmune hemolytic anemia Transfusion reaction |
|
|
|
Examples of inflammation in type 2 hypersensitivity reaction |
Good pasture disease Rheumatic fever Hyperacute transplant rejection |
|
|
|
Cell dysfunction in type 2 hypersensitivity |
1- Antibody binds to cell surface receptors 2- Abnormal blockade or activation of downstream process |
|
|
|
Cell dysfunction in type 2 hypersensitivity |
1- Antibody binds to cell surface receptors 2- Abnormal blockade or activation of downstream process |
|
|
|
Example of cellular dysfunction in type 2 hypersensitivity |
Myasthenia graves Pemohigus vulgarisms Graves’ disease |
|
|
|
Serum sickness in type 3 hypersensitivity |
1- Prototypic immune complex disease 2- Antibodies to foreign proteins are produced 1-2 weeks later 3- Antibody-antigen complex form and deposit in tissue 4- Activation of complement system 5- Inflammation and tissue damage |
|
|
|
Cause of serum sickness in type 3 hypersensitivity |
Drugs (heptens eg penicillin) Infection (hepatitis B) |
|
|
|
Cause of serum sickness in type 3 hypersensitivity |
Drugs (heptens eg penicillin) Infection (hepatitis B) |
|
|
|
Features of serum sickness in type 3 hypersensitivity 1-2 weeks later |
Fever Urticaria Lymphadenopathy Arthralgia Proteinuria |
|
|
|
Cause of serum sickness in type 3 hypersensitivity |
Drugs (heptens eg penicillin) Infection (hepatitis B) |
|
|
|
Features of serum sickness in type 3 hypersensitivity 1-2 weeks later |
Fever Urticaria Lymphadenopathy Arthralgia Proteinuria |
|
|
|
Arthus reaction in type 3 hypersensitivity reaction |
1- subacute immune complex mediated hypersensitivity reaction 2- Intradermal injection of antigen in a pre-sensitized individual leads to immune complex formation in skin 3- Characteristics edema, necrosis and activation of complement |
|
|
|
Cause of serum sickness in type 3 hypersensitivity |
Drugs (heptens eg penicillin) Infection (hepatitis B) |
|
|
|
Features of serum sickness in type 3 hypersensitivity 1-2 weeks later |
Fever Urticaria Lymphadenopathy Arthralgia Proteinuria |
|
|
|
Arthus reaction in type 3 hypersensitivity reaction |
1- subacute immune complex mediated hypersensitivity reaction 2- Intradermal injection of antigen in a pre-sensitized individual leads to immune complex formation in skin 3- Characteristics edema, necrosis and activation of complement |
|
|
|
Examples of type 3 hypersensitivity |
SLE Polyarteritis Nodosa Poststreptococcal glomerulonephritis |
|
|
|
Type 4 hypersensitivity reaction |
1- Involve T cells 2- Direct cell cytotoxicity- CD8 cytotoxic T cells kill targeted cells 3- Inflammatory reaction- effector CD4 T cells recognize antigens and release inflammatory mediated cytokines 4 - 4 T (T cell, transplant rejection, TB test, Touch(contact dermatitis) 5- PPD test in TB, Patch test in contact dermatitis and candidiasis test for T cell immune function |
|
|
|
Allergic/anaphylactic transfusion reaction |
1- Type 1 hypersensitivity reaction against plasma protein in transfused blood 2- Patients with IgA deficiency should get blood products without IgA 3- Minutes - (2-3hr) 4- Features 1- Pruritus 2- Urticaria 3- Hypotension 4- Respiratory arrest 5- Shock |
|
|
|
Acute hemolytic transition reaction |
1- Type 2 Hypersensitivity reaction 2- Cause intravascular hemolysis (ABO blood group incompatible) 3- Occurs during transfusion or within 24 hr (preformed antibodies) 4- Hypotension, fever, tachycardia, tachypnea, flank pain, hemoglobinuria, jaundice |
|
|
|
Febrile non-hemolytic transfusion reaction |
1- Cytokines created by donor WBC accumulate during storage of blood products 2- Can be prevented by leukoreduction of blood product 3- Occurs between 1-6hr 4- Fever, headache, chills, flushing 5- Most common in children |
|
|
|
Transfusion related acute lung injury |
2 hit mechanism 1- Neutrophils are sequester and prime in pulmonary vasculature due to recipient risk factor 2- Neutrophils are activated by products in the transfused blood and release inflammatory mediators- increase capillary permeability - pulmonary edema 3- Occurs minutes -6 hrs 4- Respiratory distress, non cardio genie pulmonary edema |
|
|
|
Transfusion related acute lung injury |
2 hit mechanism 1- Neutrophils are sequester and prime in pulmonary vasculature due to recipient risk factor 2- Neutrophils are activated by products in the transfused blood and release inflammatory mediators- increase capillary permeability - pulmonary edema 3- Occurs minutes -6 hrs 4- Respiratory distress, non cardio genie pulmonary edema |
|
|
|
Delayed hemolytic transfusion reaction |
1- Delayed response to foreign antigen on donor RBC previous encountered by recipient 2- Extravascular hemolysis 3- Occurs after 24 hrs or 1-2 weeks later (due to slow destruction by reticularendothelial system) 4- Self limiting and clinically silent 5- Mild fever and hyperbilirubinemia |
|
|
|
Autoantibody associated with Lambert- Eaton myasthenic syndrome |
Anti- presynaptic voltage gated calcium channel autoantibodies |
|
|
|
Antibody in rheumatoid arthritis |
Rheumatic factor (IgM antibodies against the Fc region of IgG) Anti-CCP |
|
|
|
MPO-ANCA/p-ANCA associated with which 4 disorders |
Primary sclerosing cholangitis Ulcerative colitis Microscopic polyangitis Eosinophilia granulomatosis with polyangitis |
|
|
|
Antibody associated with celiac disease |
1- IgA and IgG deamindated gliadin peptide 2- IgA anti-endomysial 3- IgA anti-tissue transdlutaminase autoantibody |
|
|
|
Autoantibody for mixed connective tissue disease |
Anti-U1 RNP |
|
|
|
Autoantibody in Graves’ disease |
Anti- TSH receptor |
|
|
|
Antibody in Sjogren syndrome |
Anti- Ro/SSA Anti- La/SSB |
|
|
|
Autoantibody in autoimmune hepatitis |
Anti- smooth muscle Anti liver/kidney microsomal 1 |
|
|
|
Autoantibody in diffuse scleroderma |
Anti- Scl- 70 (anti-topoisomerase 1 |
|
|
|
Autoantibody associated with pernicious anemia |
Anti- parietal cell Anti intrinsic factor |
|
|
|
Autoantibody in primary biliary cholangitis |
Anti mitochondrial |
|
|
|
Autoantibody in Hashimoto thyroiditis |
Anti thyroglobulin Anti thyroid peroxidase (anti microsomal) |
|
|
|
Autoantibody in dermatomyositis and polymyositis |
Anti synthetase (anti-Jo) Anti helicase (anti- Mi-2) |
|
|
|
Autoantibody in drug induced lupus |
Anti histone |
|
|
|
Autoantibody in bullous pemphigoid |
Anti hemidesmosome |
|
|
|
Auto antibody in type 1 DM |
Islet cell cytoplasmic Anti- glutamic acid decarboxylase |
|
|
|
Autoantibody in SLE |
Anti dSDNA Anti smith Antinuclear antibody Anti- cardiolipin Lupus coagulant |
|
|
|
Autoantibody in pemphigus vulgaris |
Anti desmosome (anti- desmoglein) |
|
|
|
Autoantibody in limiters scleroderma (CREST syndrome) |
Anti centromere |
|
|
|
Autoantibody in Goodpastures syndrome |
Anti glomerular basement membrane |
|
|
|
Autoantibody in myasthenia gravis |
Anti Ach receptor |
|
|
|
Autoantibody in anti phospholipid syndrome |
Anti B2 glycoproteins 1 Anti- cardiolipin Lupus anticoagulant |
|
|
|
Autoantibody for granulomatosis with polyangitis |
PR3- ANCA /cANCA |
|
|
|
Autoantibody for primary membranous neuropathy |
Anti- phospholipasebA2 receptor |
|
|
|
Bacterial infection in immunodeficiency |
T- cell - Sepsis B- cell - encapsulated organism Granulocytes - Staphylococcus, Burkholder cepacia, Pseudomonas aeruginosa, Nocardia, Seratia Complement - early - severe recurrent pyogenic sinus and respiratory tract infection, SLE Late Niesseria meningitidis
|
|
|
|
Virus infection In immunodeficiency |
T cell- CMV, EBV, JC virus, VSV, chronic infection with respiratory and GI tract virus B cell- enteroviral encephalitis, polio virus |
|
|
|
Fungal infection in immunodeficiency |
T cell- Candida (oral), PCP, Crytpoccocus B cell- GI giardia Granulocytes - Candida(systemic), aspergillosis mucor |
|
|
|
Immunodeficiency of what type of cell can cause gastrointestinal giardiasis |
B cell define you without IgA production |
|
|
|
What type of vaccines are contraindicated for patients with B cell immunodeficiency |
Live attenuated vaccines |
|
|
|
What is the general difference between infections commonly associated with T cell and B cell immunodeficiency |
T cell deficiencies tend to produce recurrent viral/fungal infection B cell deficiency produce recurrent bacterial infection |
|
|
|
Hyperacute transplant rejection |
1- Within minutes 2- Pre-existing recipient antibodies against donor antigen 3- Widespread thrombosis of graft vessels - Ischemia/necrosis (type 2 hypersensitivity reaction) 4- Grapft must be remove |
|
|
|
Acute transplant rejection |
1- Weeks to months 2- Cellular 1- CD8 T cells and/or CD 4 T cells activated against donor MHC Humoral - Similar to hyperacute except antibodies develop after transplant 3- Vasculitis graft vessel and dense interstitial lymphocytic infiltrate (type 4 hypersensitivity) 4- Prevent/revers with Immunosuppressants |
|
|
|
Chronic transplant rejection |
1- Months - Years 2- CD 4 T cells respond to receipt APC presented on donor peptide (allogenic MHC) 3- Both Hunoral and cellular components (type 2 and 4 hypersensitivity reaction) 4- Recipient T cell react and secrete cytokine- proliferation of vascular smooth muscle, parenchyma atrophy and interstitial fibrosis 5- Dominated by arteriosclerosis 6- Organ specific examples 1- Accelerated artherosclorosis 2- Bronchiolitis obliterans 3- Chronic allograft nephropathy 4- Vanishing bile duct syndrome |
|
|
|
Graft vs host transplant rejection |
1- Time varies 2- Graft immuno -competent T cell proliferated in immunocompromised host and reject host cell with foreign protein- sever organ dysfunction 3- Type 4 hypersensitivity reaction 4- Mucopapulary rash, Diarrhea, Jaudice and Hepatosplenomegaly 5- Occurs in liver and bone marrow transplant(rich in lymphocytes) 6- Potentially beneficial in bone marrow transplant for leukemia 7- Immunocompromised patients should receive irradiated blood products before transfusion to prevent GvHD |
|
|
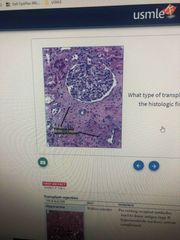
What type of transplant rejection |
Chronic transplant rejection |
|
|
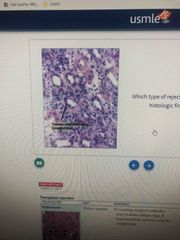
What type of transplant rejection |
Acute transplant rejection |
|
|
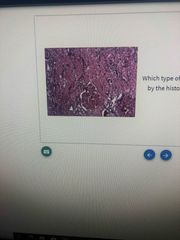
What transplant rejection |
Hyperacute rejection |
|