![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
123 Cards in this Set
- Front
- Back
- 3rd side (hint)
|
Pharmacokinetics |
Absorption, distribution, metabolism, excretion and effect of a drug on the body |
5 |
|
|
Pharmacodynamics |
Mechanisms of/and actions of drugs |
|
|
|
Drug |
Chemical that affects physiological function in a specific way |
|
|
|
Drug target site |
biological entity who's activity is modulated by a compound |
|
|
|
Affinity |
Ability of a drug to locate and bing to its target/receptor |
|
|
|
Efficacy |
Measure of how well a drug induces a response |
|
|
|
Potency |
Measure of how much of a drug is required to induce a particular level of response. Depends of affinity and efficacy |
Definition What does is depend on? |
|
|
Competitive antagonist |
Act on the same site as the agonist Surmountable Shifts dose-response curve to the right Atropine, Propanolol |
2 points Effect on dose-response curve 2 examples |
|
|
Irreversibel antagonist |
Acts on the same site or a different site to the agonist Insurmountable Shifts dose-response curve to the right and lowers maximum response Hexamonthonium |
2 points Effect on dose-response curve 1 example |
|
|
Four main categories of drug target sites |
Receptors Ion-channels Transport mechanisms Enzymes |
|
|
|
4 types of receptors |
Ion-channel linked (msec) G-protein coupled (sec) Tyrosine kinase linked (min) Intracellular steroid (hours) |
|
|
|
2 types of ion channels
|
Voltage-sensitive
Receptor-linked |
|
|
|
2 examples of drugs that act on transport systems |
TCA - reduced NA uptakeDigoxin - Cardiac glycoside acting on Na+/K+ ATPase |
|
|
|
3 kinds of drug interactions with enzymes |
Enzyme inhibitors - Neostigmine False substrates - MethylDOPA (competitively inhibits DOPA decarboxylase) Prodrugs - Chloral hydrate - Trichloroethanol |
|
|
|
3 non-specific drug actions |
General anaesthetics? Antacids - ranitidine Osmotic purgatives |
|
|
|
Receptor reserve phenomenon |
There are excess receptors on the cell surface than what is necessary for a full effect -Allows for high sensitivity and high speed response to a low stimulus -Same response can still be produced if the some receptors are damaged |
|
|
|
Four principle types of drug antagonism |
Receptor blockade Physiological antagonism Chemical antagonism Pharmacokinetic antagonism |
|
|
|
Physiological antagonism |
Stimulating receptors with the opposite effecte.g. NA - vasoconstriction / Histamine - vasodilation |
Definiton Example |
|
|
Chemical antagonism |
Interaction in solution leading to the effect of the active drug being lost e.g. dimercarpol - chelating agent |
Definiton Example |
|
|
Pharmacokinetic antagonism |
Reduced concentration of the active drug at the site of action Decreased absorption, increased metabolism, increased excretion e.g. barbituates - phenolbarbital (decreases effect of warfarin) |
Definition 3 mechanism Example |
|
|
5 mechanisms that contribute to drug tolerance |
Pharmacokinetic factors Loss of receptors Change in receptors Exhaustion of chemical mediators Physiological adaption |
|
|
|
The journey of a drug through the body |
Administration Absorption Distribution Metabolism Excretion Removal |
6 |
|
|
Enteral administration of drugs |
Sublingual Buccal Oral Rectal |
4 |
|
|
Parenteral administration of drugs
|
Intravenous Intramuscular Subcutaneous Percutaneous Inhalation |
5 |
|
|
What kind of chemical are most lipid soluble drugs |
Small volatile / Non-ionized |
|
|
|
What kind of chemical are most water soluble drugs |
Weak acids or bases which can become charged |
|
|
|
6 ways molecules can be transferred across a membrane |
Passive diffusion - Lipophillic Facilitated diffusion Active transport Pinocytosis Filtration - small water soluble molecules Paracellular transport |
|
|
|
pH partition hypothesis |
States that only the unionised form of a drug passes through the intestinal membrane Ionised drug - Unionised drug are in dynamic equilibrium Predicts that: Weakly acidic drugs e.g. aspirin are preferentially absorbed in the stomach as opposed to the more alkali intestine. These drugs are more likely to be ionised in the small intestine and therefore will not diffuse well through hydrophobic lipid membranes. Vice versa for basic drugs e.g. antihistamine |
|
|
|
Problem with the pH partition hypothesis |
Vast majority of drugs are absorbed in the small intestine irrespective of their degree of ionization due to the SI's large SA and rich blood supply. |
|
|
|
Factors affecting drug distrubution |
Regional blood flow
Extracellular binding - PPB affects half life Capillary permeability - affects metabolism Localisation in tissues - fatty tissue accumulates drugs well |
|
|
|
Effect of kidneys on distribution of a drug |
Glomerulus: drug-protein complexes not filtered Proximal tube: active secretion of acids and bases Proximal and Distal tubes: lipid soluble drugs reabsorbed - prolongs half life |
3 Glomerulus Proximal tube Proximal tube + Distal tube |
|
|
Effect of liver on distribution of a drug |
Biliary excretion: LMW molecules can be concentrated in the bile (LMW cut off in humans - 1500) Active transport: into bile Enterohepatic cycling: Drug excreted into guy via bile and then reabsorbed in the duodenum - Drug persistence |
3 Biliary excretion Active transport Enterohepatic Cycling |
|
|
Effect of lungs on distribution of a drug |
Excreted via expired air Passive diffusion of volatile compounds |
2 |
|
|
Bioavailability |
Proportion of the administered drug that is available within the body to exert its pharmacological effect. Measured by comparing areas under concentration/time curves (AUC) |
Definition How it is measured |
|
|
Apparent volume of distrubution |
Volume in which a drug is distributed - indicator of pattern of distrubution |
|
|
|
Clearance |
Volume of blood plasma cleared of a drug per unit time Related to volume of distribution and rate at which the drug is eliminated |
|
|
|
First-pass metabolism |
Phenomenon by which the concentration of a drug is greatly reduced before it enters systemic circulation / any metabolism before the drug goes into circulation |
|
|
|
Reactions of phase I drug metabolism |
Oxidation Reduction Hydrolysis |
3 |
|
|
Reactions of phase II drug metabolism |
Glucuronidation Acetylation Amino acid conjugation Sulphation Methylation Glutathione conjugation |
6 |
|
|
General function of each phase of drug metabolism |
Phase I - generation of a derivative with a functional group Phase II - Use of functional group to attach a large, polar, endogenous molecule to promote excretion |
Phase I Phase II |
|
|
Cytochrome P450 mediated oxidation |
|
|
|
|
Glucuronidation |
Glucuronyl transferase UDP-glucuronic acid OH, COOH, NH2, SH Most common reaction |
Enzyme Conjugating agent Target functional group |
|
|
Acetylation |
Acetyl transferase Acetyl-CoA OH, NH2 |
Enzyme Conjugating agent Target functional group |
|
|
Amino acid conjugation |
Acyl transferase Glycine, glutamine, taurine COOH |
Enzyme Conjugating agent Target functional group |
|
|
Methylation |
Methyl transferase S-adenosyl-methionine OH, NH2 |
Enzyme Conjugating agent Target functional group |
|
|
Sulphation |
Sulphotransferase 3'-phosphoadenosine-5-phosphosulphate (PAPS) OH, NH2 |
Enzyme Conjugating agent Target functional group |
|
|
Glutathione conjugation |
Glutathione-S-transferase Glutathione Electrophiles |
Enzyme Conjugating agent Target functional group |
|
|
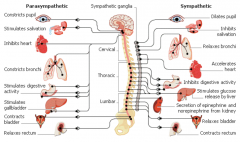
Effect of sympathetic innervation on: Eye Trachea/bronchioles Liver Adipose Kidney Ureters/bladder |
Pupil dilation Bronchodilation Glycogenolysis/gulconeogensis Lipolysis Increased renin secretion Relaxes detrussor/constriction of trigone + sphincter |
|
|
|
Effect of sympathetic innervation on: Salivary glands Skin Heart GI Blood vessels to skeletal muscle Blood vessels to skin, mucous membranes + splanchnic area |
Thick, viscous secretion Piloerection/increase sweating Increased rate and contractility Decrease in motility and tone/sphincter contraction Dilation Constriction |
|
|
|
Effect of parasympathetic innervation on: Eye Trachea and bronchioles Ureters and bladder Salivary glands Heart GI |
Pupil constriction/ciliary muscle contraction Constriction Contracts detrussor/relaxation of trigone and sphincter Copious water secretion Decreased rate and contractility Increase in motility, tone and secretions |
|
|
|
Which spinal and cranial nerves do parasympathetic fibres arise from |
S2 S3 S4 CN3 CN7 CN9 CN10 |
3 spinal 4 cranial |
|
|
Which spinal nerves do sympathetic fibres arise from |
T1 - L2 |
Range |
|
|
Transmitters release from pre- and post- ganglionic fibres in sympathetic and parasympathetic nervous systems |
Sympathetic: ACh - ACh Parasympathetic: ACh - NA ACh - Adrenal medulla - NA ACh - ACh |
1 sympathetic 2 parasympathetic |
|
|
The reaction for ACh synthesis |
Acetyl-CoA + Choline - ACh + CoA via Choline acetyl transferase |
|
|
|
Summarise ACh release |
ACh packaged into vesicles Action potential stimilates Ca2+ influx into the neuron at the presynaptic terminal This promotes fusion of vesicles with presynaptic membrane ACh released into synaptic cleft and diffuses across synpase ACh binds to receptor and is then released |
5 ACh packaged into vesicles - - - -Binds to receptor |
|
|
Summarise ACh degredation |
ACh degradation occurs in synaptic cleft ACh - choline + acetate via acetylcholinesterase Products used to regenerate ACh |
Where does it occur Equation Use of products |
|
|
Summarise the synthesis of NA |
Tyrosine actively transported into neurone Tyrosine -> DOPA via Tyrosine hydroxylase DOPA -> DA cia DOPA decarboxylase Dopamine packaged into vesicles NA synthesis occurs in vesicles DA -> NA via Dopamine B-hydroxylase |
6 3 reactions 3 points |
|
|
Summarise the degradation of NA |
Uptake 1: Neurones + degraded by MAO-A (monoamine oxidase A) Uptake 2: Non-neuronal tissue + degraded by COMT |
2 |
|
|
Summarise adrenaline synthesis |
Same as NA except NA is released from vesicles and NA -> Adrenaline via phenylethanolamine methyl transferase |
|
|
|
Summarise the principle metabolites of NA and A |
Degradation: NA/A -> MOPEG/VMA via COMT/MAO-A Conjugation: MOPEG/VMA -> Glucuronide/sulphate (urine) |
|
|
|
Principle metabolites of NA/A in the CNS and PNS |
CNS: MPEG PNS: VMA (principle urinary metabolite) |
|
|
|
Define: COMT MAO-A MOPEG VMA |
COMT: Catechol-O-methyl transferase MAO-A: Monoamine oxidase A MOPEG: 3-methoxy-4-hydroxy-phenyl ethylene glycol VMA: Vanillylmandelic acid |
|
|
|
Nicotinic cholinoreceptors |
All autonomic ganglia Stimulated by nicotine/acetylcholine Type 1 - Ionotropic Blocked by hexamethonium |
Location Stimulated by Type of receptor Blocked by |
|
|
Muscarinic cholinoreceptors |
All effector organs innervated by post-ganglionic parasympathetic fibres and certain organs innervated by sympathetic fibres (sweat glands) Stimulated by muscarine/acetylcholine Type 2 - G-protein couples M1 - Neural M2 - Cardiac M3 - Exocrine and smooth muscle Blocked by atropine |
Location Stimulated by Type of receptor Subtypes Blocked by |
|
|
Adrenoreceptors |
At all effector organs innervated by post-ganglionic sympathetic fibres Stimulated by NA and A Sype 2 - G-protein coupled a1 a2 b1 b2 |
Location Stimulated by Type of receptor Subtypes |
|
|
Subunit combination of nicotinic receptors in the somatic nervous system and autonomic nervous system |
Somatic (muscle): 2abge Autonomic (ganglion): 2a3b |
§ |
|
|
Directly acting cholinomimetic drug |
ACh receptor agonists e.g. bethanecol (choline ester) pilocarpine (alkaloid) |
Definition 2 examples |
|
|
Indirectly acting cholinomimetic drugs |
Inhibits acetylcholinesterase Use-dependent Reversible anticholinesterases: physostigmine, neostigmine, donepezil Irreversible anticholinesterases: ecothiopate, dyflos, sarin |
Definition 2 examples of reversible 2 examples of irreversible |
|
|
Symptoms of anicholinesterase poisoning |
Early: headache, nausea, dizziness and hypersecretion Late: muscle weakness, twitchiness, tremor, incoordination, vomiting, abdominal cramps, diarrhea |
2 early symptoms 3 late symptoms |
|
|
Treatment of organophosphate poinsoning |
Atropine (abolishes muscarinic effects) Artificial respiration Pralidoxime (binds to organophosphate inactivated anticholinesterase) |
3 |
|
|
Systems targeted by high muscarinic activity |
Eye Salivary glands Sweat glands Lungs Heart Gut Bladder Vasulcature |
8 |
|
|
Muscarinic effects on the eye |
Contraction of the ciliary muscle - accommodation for near vision Lacrimation Contraction of sphincter pupillae - pupil constriction (miosis) - opens canals of schlemm allowing aqueous humour to drain - reducing intra-ocular pressure - treatment of glaucoma |
3 |
|
|
Muscarinic effects on the heart |
Acts on M2 AChR in atria and nodes Decrease in cAMP: -Decreased Ca2+ influx - decreased CO -Increased K+ efflux - decreased HR |
Receptor 2 effects |
|
|
Muscarinic effects on vasculature |
Most blood vessels do not have parasympathetic innervation M3 AChR on vascular endothelial cells Stimulates NO release - induces smooth muscle relaxation - vasodilation - decreased TPR |
Location Effect |
|
|
Muscarinic effects on CVS |
Sharp drop in blood pressure |
|
|
|
Muscarinic effects on non-vascular smooth muscle |
Contraction Lungs: bronchoconstriction Gut: increased gut motility Bladder: increased bladder emptying |
3 |
|
|
Muscarinic effects on exocrine glands |
Salivation Increased bronchial secretions Increased gastro-intestinal secretions Increased sweating |
4 |
|
|
Summarise muscarinic effects on the body |
Hypotension Increased sweating Difficulty breathing Increased urination GI pain Increased salivation and lacrimation |
5 |
|
|
Where are muscarinic M4 and M5 founds |
CNS |
|
|
|
M1, M3, M5 G-protein subtype |
Gq (IP3) |
|
|
|
M2, M4 G-protein subtype |
Gi (cAMP) |
|
|
|
Acetylcholinesterase |
True/specific cholinesterase All cholinergic synapses Very rapid action (10, 000/s) Highly selective for ACh |
Location Speed of action Specificity |
|
|
Butyrylcholinesterase |
Pseudocholinesterase Plasma and tissues (e.g. liver and skin) not synapses Broad substrate specificity: hydrolyses other esters e.g. suxamethonium (skeletal muscle relaxant) principle reason for low plasma ACh Shows genetic variation |
Location Specificity |
|
|
Nicotinic receptor antagonists |
Ganglion blocking drugs at all autonomic ganglia Do not block at NMJ since the receptors are different Effect depends on dominant autonomic tone to the effector organ Use-dependent channel blockade = incomplete block |
Definition
NMJ Effect Use-dependent channel blockade |
|
|
Effect of nicotinic receptor antagonists on the kidney |
Sympathetic NS dominates - causes renin secretion - Increased NA and water retention Effect: decreased renin secretion (Trimetaphan use in surgery) |
Dominant autonomic tone's effect Antagonist's effect Use |
|
|
Effect of nicotinic receptor antagonists on blood vessels |
Sympathetic NS dominates
Effect: Vasodilation - hypotensive effect (Trimetaphan use in surgery) |
Dominant autonomic tone Effect Use |
|
|
Treatment of atropine poisoning |
Anti-cholinesterases e.g. physostigmine (indirect cholinomimetic) Allows increased ACh levels in synaptic cleft to out-compete atropine Atropine will be cleared over time |
Drug MoA |
|
|
Botulinum toxin |
Parasympatholytic Protease enzyme that breaks down SNARE proteins preventing fusion of ACh vesicle with the pre-synaptic membrane - preventing ACh release Remove wrinkles by paralysing skeletal muscle (ACh at NMJ) Treat excessive sweating (Muscarinic receptors in sweat glands) |
ToD MoA Use (2) |
|
|
Adrenal receptor subtype and effect in the: Eye Lacrimal glands |
Eye: Mydriasis (a1++) Aqueous humour production by ciliary body (B+) Lacrimal glands: Tears (a1+) |
Eye (2) Lacrimal glands (1) |
|
|
Adrenal receptor subtype and effect in the: Salivary glands Skin |
Salivary glands: Thick, viscous secretion (ab) Skin: Increased sweating, contraction of pilomotor muscle (a1+++) |
Salivary glands (1) Skin (1) |
|
|
Adrenal receptor subtype and effect in the: Heart Trachea and Bronchioles |
Heart: Increased rate and contractility (B1+++) Trachea and Bronchioles: Diation (B2+) |
Heart (1) Trachea and bronchioles (1) |
|
|
Adrenal receptor subtype and effect in the: Liver GIT Adipose |
Liver: glycogenolysis, gluconeogenesis (a1/B2+++) GIT: Decreased muscle motility and tone, contraction of sphincters (a/B) Adipose: Lipolysis (a1B1++) |
Liver (1) GIT (1) Adipose (1) |
|
|
Adrenal receptor subtype and effect in the: Kidney Urinary Bladder Ureter |
Kidney: Increased renin secretion (B1++) Urinary bladder: Relaxes detrussor (B2+) Constricts trigone and sphincter (a1++) Ureter: Increased motility and tone (a1+) |
Kidney (1) Urinary bladder (2) Ureter (1) |
|
|
Adrenal receptor subtype and effect in the: Female genitalia Male genitalia Blood vessels |
Female genitalia: Relaxation of uterus (B2) Male genitalia: Stimulates ejaculation (a1+++) Blood vessels: Skeletal muscle vasodilation (B2++) Skin, mucus membrane, splanchnic, abdominal viscera, salivary gland vasoconstriction (a1+++) |
Female genitalia (1) Male genitalia (1) Blood vessels (2) |
|
|
Describe the selectivity of the subtypes of adrenoceptors for adrenaline and noradrenaline |
Alpha - Higher selectivity for noradrenaline Beta - Higher selectivity for adrenaline |
Alpha: Beta: |
|
|
Directly acting sympathomimetics |
Mimic the actions of Adrenaline and Noradrenaline by acting on adrenoceptors Used principally for their actions on CVS, eyes and lungs |
Definition Principal use |
|
|
Secondary messengers of each of the subtypes of adrenoceptors |
a1 - PLC: IP3 + DAG increases a2 - cAMP decreases B1 - cAMP increases B2 - cAMP increases |
4 |
|
|
Clinical use of adrenline |
Allergic reaction and anaphylactic shock COPD, chronic bronchitis, emphysema and asthma emergencies Acute management of heart block Intra spinal anaesthesia Prolong the duration of local anaesthetics Treat glaucoma |
6 |
|
|
Which effects of adrenaline are used for treatment of allergic/anaphylactic reactions |
Administered IV/autoinjector Reverses severe hypotension and bronchoconstriction via vasoconstriction, increased heart rate + contractility, bronchodilation and inhibition of release of hypotensive + bronchoconstrictor mediators |
Administration What does it reverse How does it do this |
|
|
Which effects of adrenaline are used for treatment of COPD, chronic bronchitis, emphysema and asthma |
Bronchodilator action combined with suppression of bronchoconstrictor mediator release |
Effect |
|
|
Which effects of adrenaline are used for treatment of acute management of heart block |
IV Increase in TPR - increased venous return Increase in HR and force of contraction Caution: over-stimulation of heart or reflex tachycardia |
Administration Effect Caution |
|
|
Which effects of adrenaline are used in spinal anaesthesia |
To maintain blood pressure since epidural anaesthetics affect the sympathetic nervous system which usually controls blood pressure |
Effect |
|
|
Which effects of adrenaline are used in local anaesthesia |
Vasoconstriction reduces blood flow to target region and therefore: prolongs duration of anaesthesia minimises dose of anaesthesia required |
Effect |
|
|
Which effects of adrenaline are used for treatment of glaucoma |
Vasoconstriction in ciliary processes that produce aqueous humour |
Effect |
|
|
Unwanted, if any, effects of adrenaline on: Secretions CNS CVS GIT Skeletal muscle |
Secretions: reduced and thickened mucous CNS: minimal, does not cross BBB CVS: Vasoconstriction - cold extremities GIT: minimal Skeletal muscle: tremor |
|
|
|
Pharmacokinetics of NA and A |
Administration: IV, intramuscular, locally/topically Poorly absorbed orally Rapid metabolism in gut, liver and other tissues Duration of action: minutes |
Administration (3) Administration of poor absorption Metabolism Duration of action |
|
|
Explain why foods which contain tyramine, an indirectly acting sympathomimetic, represent no harm to the normal subject, but may precipitate a life-threatening hypertensive crises in patients taking monoamine oxidase inhibitors |
Has weak adrenoceptor agonistic activity Competes with catecholamines for Uptake 1 Displaces NA from its storage vesicles into cytosol Competes with NA for a site on MAO Cytoplasmic NA leaks through neuronal membrane and acts on postsynaptic adrenoceptors MAO inhibition - hypertensive crisis |
|
|
|
Parasympathetic and Sympathetic effects on and from which vertebrae the nerves arise: Pupil Salivation Heart Bronchi Digestive system Liver Kidney Gallbladder Bladder Rectum |
|
|
|
|
5 types of adrenoceptors |
a1 a2 b1 b2 b3 |
|
|
|
Effect of a1 adrenoceptor |
Vascoconstriction Relaxation of GIT |
2 |
|
|
Effect of a1 adrenoceptor |
Inhibition of transmitter release Contraction of vascular SM CNS actions |
3 |
|
|
Effect of b1 adrenoceptor |
Increased cardiac rate and force Relaxation of GIT |
2 |
|
|
Effect of b2 adrenoceptor |
Bronchodilation Vasodilation Relaxation of visceral smooth muscle Hepatic glycogenolysis |
4 |
|
|
Effect of b3 adrenoceptor |
Lipolysis |
1 |
|
|
Clinical uses of SNS antagonists |
Hypertension Cardiac arrhythmias Angina Modify plasma lipid levels Glaucoma |
5 |
|
|
Define hypertension |
Sustained diastolic pressure greater than 90mmhg |
|
|
|
Main elements that contribute to hypertension |
Blood volume - kidney CO Peripheral vascular tone |
3 |
|
|
Tissue targets for antihypertensives |
Sympathetic nerves that release NA (vasoconstrictor) Kidney Heart Arterioles CNS |
5 |
|
|
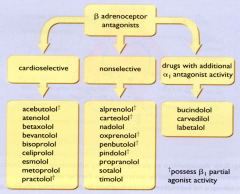
B adrenoceptor antagonists that: Cardioselective Nonselective Also have a1 antagonistic activity |
|
3/4 each |
|
|
A selective and non-selective cardioselective adrenoceptor antagonist |
Selective - Atenolol (B2) Non-selective - Propanolol (B1 + B2) |
|
|
|
Cardioselectivity |
Having greater activity on the cardium |
|
|
|
Effect of beta-adrenoceptor antagonism on the CNS |
Reduce sympathetic tone: Reduction in HR and CO Renin production from the kidney |
3 |
|
|
Effect of beta-adrenoceptor antagonism on synapses |
Blocks pre-synaptic B1 receptors - reduction in NA release - contributing 5-7% of total antihypertensive effect |
Blocks which receptor Reduces release of what Responsible for what percentage of which effect |