![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
144 Cards in this Set
- Front
- Back
|
Milk |
mammalian characteristic main component: human milk oligosaccharides (HMO) - food for gut microbes comprised of lactose, fat, HMO |
|
|
Bifidobacteria longum infantis |
more common in stool of breast fed babies vs. formula babies changes babies gut with short chain fatty acids makes gut cells more adhesive proteins seal gaps between gut cells protect against foreign bacteria produce anti-inflammatory molecules supports baby's brain growth by eating HMOs |
|
|
HMOs |
Human Milk Oligosaccharides (200 variations) Sailic acid is released when bacteria eats HMOS attach to pathogens by mimicking glycans of gut epithelium Can block salmonella, listeria, librio chlorae, campylobacter, HIV |
|
|
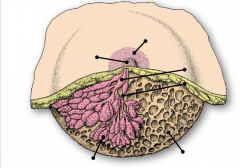
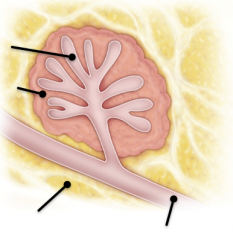
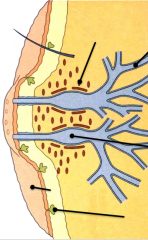
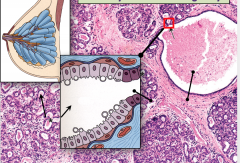
Mammary Gland- compound tubuloalveolar gland with 15-20 lobes derived from modified apocrine sweat glands Top to Bottom: areola nipple lactiferous sinus lactiferous duct dense connective and adipose tissue |
|
|
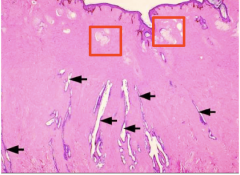
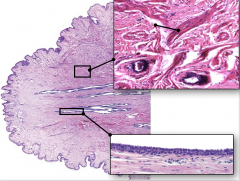
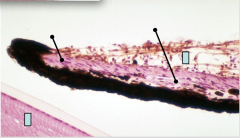
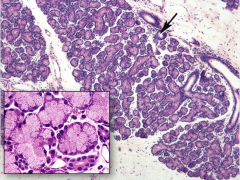
Nipple with Ducts Red boxes: sebaceous glands without hair follicle Arrow: lactiferous ducts |
|
|
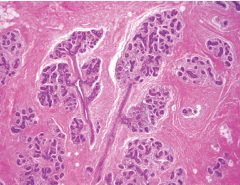
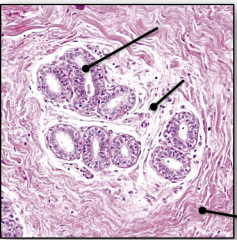
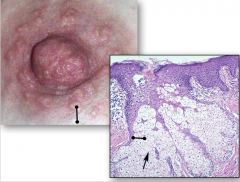
Normal Breast duct connects with nipple and glandular tissue non-lactating because there is too much fibrous tissue (sometimes mistaken for eccrine sweat glands, but there is NO ADIPOSE) |
|
|
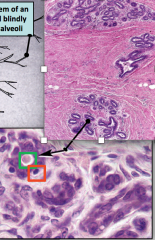
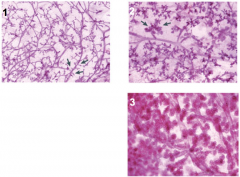
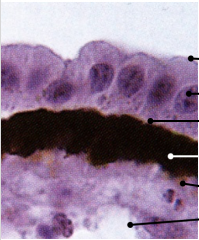
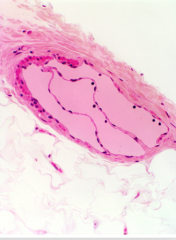
Lactiferous chambers: reservoir for milk Red: myoepithelial cells Green: duct |
|

|
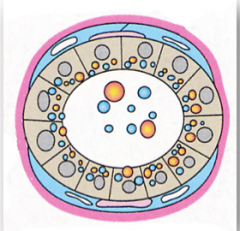
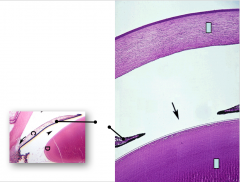
1 . Dermal mesenchymal cells induce formation of epithelial bud 2. Adipose cells stimulate branching of epithelial cell cords 3. Mammory cords become hollow and some luminal epithelial cells differentiate into myoepithelial cells (pink) Squares are epithelial cells |
|
|
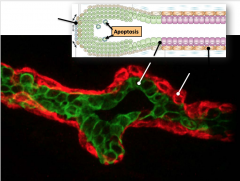
Tip: cap cells (apoptosis/die out to make lumen) Red stain: myoepithelial cells Green stain: luminal cells |
|
|
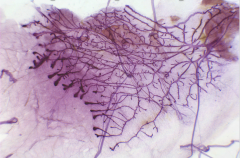
Mouse Mammary Gland |
|
|
Top to Bottom: Dutcules and acini Intralobular LOOSE CT Interlobular DENSE CT |
|
|
Top to Bottom: Dutcules and acini Intralobular LOOSE CT Interlobular DENSE CT Lactiferous duct |
|

|
Top to Bottom: lactiferous sinus Sebaceous gland |
|
The Nipple |
Top to Bottom: lactiferous duct smooth muscle lactiferous sinus areola sebaceous gland / Montgomery glands |
|
|
The Nipple Top to Bottom: Smooth muscle bundles Lactiferous Sinus (stratified cuboidal epithelium) nuclei long an flat (not erector pilae because there is no hair follicle) |
|
|
Sebaceous glands/Glands of Montgomery not associated with hair follicles lubricate nipple secrete volatile compounds that stimulate suckling antimicrobial substance |
|
|
Mammary Gland: Puberty vs. Pregnancy |
Puberty: estrogen (stimulates duct development), progesterone (stimulates alveolar bud formation), and prolactin Pregnancy: prolactin and placental hormones Hyperplasia of fat and lobules= alveolus gets bigger and increases in cell number |
|

Mouse Mammary Gland: Development |
Pre-Puberty (4 weeks): Rudimentary Duct System Mid Puberty (6 weeks): Duct Elongation Adult Virgin (10 weeks): Duct Branching |
|
|
1. Early Pregnancy- Side Branching 2. Mid-Pregnancy: alveologenesis (alveoli number increases) Alveoli gets larger in 1 and 2 3. Post-partum: lactation |
|

|
Non pregnant woman gland has inactive duct system has a lot of fibrous tissue |
|

|
During Pregnancy alveoli proliferate at ends of ducts - hyperplastic hormones cause proliferation ducts produce collostrum |
|

|
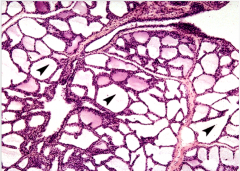
After birth/during lactation alveoli are fully differentiated with abundant milk secretion (may get confused with thyroid follicle but NO ELONGATED DUCT) |
|
|
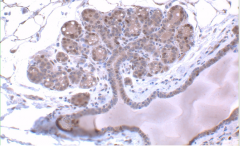
Resting Mammary gland during early stages of pregnancy Top to Bottom: Adipose Tissue Lactiferous Duct Proliferation of corpus luteum, placenta, duct cells, and secretory cells due to estrogen and progesterone control Also controlled by prolactin (by anterior pituitary, human placental lactogen (somatomammotropin), adrenocorticoids, and thyroid hormone |
|
|
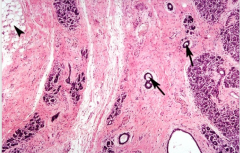
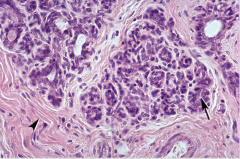
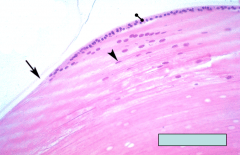
Mammary gland during early pregnancy: proliferation of ducts and secretory alveoli formation Left to right: Interlobular dense irregular CT Alveoli surrounded by intralobular loose CT |
|
|
Breast During Pregnancy (end of pregnancy) Little connective tissue and many ducts Hyperplasia of glandular units Start to make milk in the lumen (don't mistake for carcinoma) |
|
|
TDLU: Terminal Duct Lobular Unit not pregnant because of the amount of connective tissue |
|
|
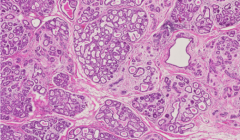
Mammary Gland at late Pregnancy Prolactin stimulates secretion of collostrum and milk by alveolar cells Left to Right: Distended alveoli Lactiferous Duct: filled with milk |
|
|
Lactating Mammary Gland with distended alveoli Influence of Prolactin Alveoli secrete milk and other, especially Immunoglobulin A. Expanded alveoli compress secretory cells somewhat. (Don't mistake for thyroid or lung, mammary glands have long systems of ducts. Lungs don't have as many cells and this picture lacks bronchi and blood vessels. Kidney has glomeruli.) |
|
|
Steps to lactation |
1. Mammogenesis, stimulated during pregnancy by estrogen and progesterone, as well as prolactin. 2. Lactogenesis, stimulated after parturition by prolactin 3. Galactopoiesis, stimulated by prolactin and oxytocin. |
|
|
Hormone Control: hypothalamus->? |
Hypothalamus controls anterior pituitary/adenohypophysis/pars distalis to release prolactin via prolactin releasing factor and thyrotropin-releasing hormone. Inhibition via dopamine Posterior pituitary/pars nervosa/neurohypophysis makes oxytocin |
|
|
Top to bottom: Lipids Lactose Proteins IgA Prolactin Oxytocin |
|
|
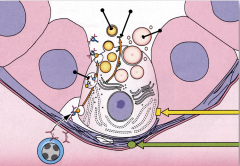
Secretion steps |
1. Prolactin stimulates milk production 2. plasma cells bring in IgA which is shuttled across epithelium and exocytosed 3. Lactose, produced in the Golgi, is secreted via merocrine release 4. Lipids released surrounded by rim of cytoplasm, apocrine secretion 5. Proteins (casein, lactabumin,) secreted by merocrine mechanism 6. Oxytocin stimulates milk release by inducing contraction of myoepithelial cells |
|
|
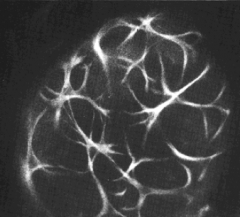
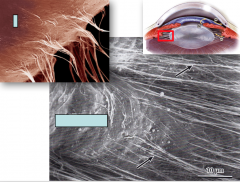
Top: Picric acid methylene blue stain Bottom: H&E stain Interdigitating, star shaped, myoepithelial cells around individual alveoli and ducts Myoepithlial cells have 5-8 dendritic extensions with keratin, function like smooth muscle (If you can see myoepithelial cell, then not cancer) |
|

|
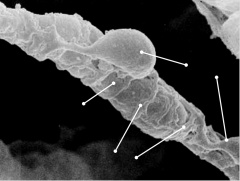
Technique: scanning electron micrographs Secretory acini surrounded by myoepithelial cells Contract with stimulation via oxytocin, making secretory products release into duct system |
|
|
Technique: F-actin staining Secretory acini surrounded by myoepithelial cells Contract with stimulation via oxytocin, making secretory products release into duct system |
|
|
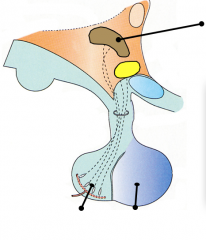
Top to Bottom: Paraventricular nucleus of the Hypothalamus Pars Nervosa/Neurohypophysis/Posterior Pituitary (Left) Pars Distalis/Adenohypophysis/Anterior Pituitary |
|
|
Paraventricular nucleus of the Hypothalamus produces release of Oxytocin via Posterior pituitary Oxytocin causes contraction of myoepithelial cells in lactating mammary gland |
|
|
Breast Cancer |
Ductal (most common at 80%): invasive ductal carcinoma Lobular (10% of cancer): invasive lobular carcinoma Other 10% scattered between 10 other kinds of breast cancer If cancer stays inside duct, then not invasive |
|
|
Breast Cancer Molecular Subtypes |
ER+, HER- (luminal) 50-65% with low proliferation and high proliferation (BRCA2) HER2+ (20%) ER-, HER2- (basal like) 15% (BRCA1): triple negative, worst for african americans because nothing will work Minority of breast cancers run in the family |
|
|
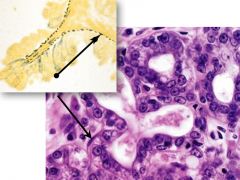
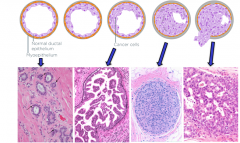
Breast Cancer: Ductal Carcinoma (most common form of breast cancer) Left to Right: 1. Normal duct 2. Ductal hyperplasia 3. Atypical hyperplasia 4 DCIS 5. Invasive ductal carcinoma |
|
|
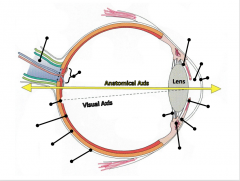
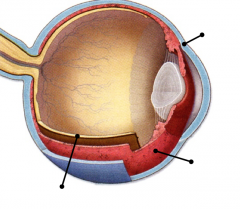
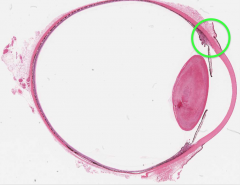
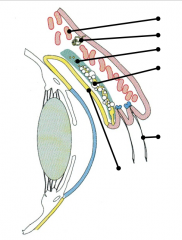
Top to Bottom: Optic Nerve: CN2 Posterior Chamber Vitreous Chamber Anterior chamber Optic Disk Cornea Fovea Centralis Iris Suspensory Ligament Retina Canal of Schlemm Choroid Ciliary Body with Ciliary Muscle Sclera |
|
|
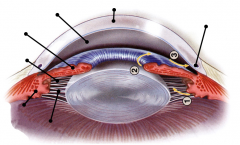
Top to Bottom: Outer Fibrous Tunic (sclera and cornea): Cornea: accommodation and light refraction Sclera: continuous with anterior chamber and dura Middle vascular Tunic (Uvea) Iris Ciliary body: where viterous and aqueous humor are made Choroid Inner Tunic (retina) Pigmented epithelium Neural Retina *No blood vessels in the cornea or lens |
|
|
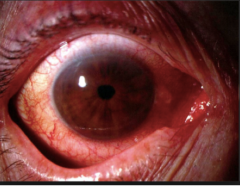
Uveitis: redness and inflammation of the middle vascular tunic |
|

|
Jaundice Yellow eyes from excess of bilirubin Due to drugs |
|

|
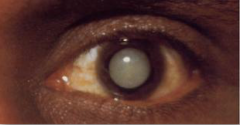
Retinoblastoma: looks like white reflection in pupil |
|
|
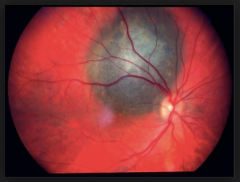
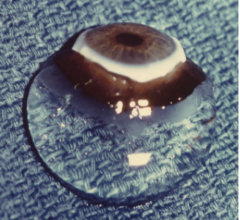
Choroidal Melanoma: large black mass |
|
|
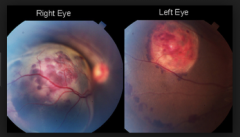
Renal Cell Carcinoma, Metastatic from Choroid of Right to Left Eye Left has a larger carcinoma then right |
|
|
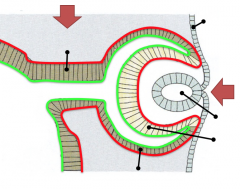
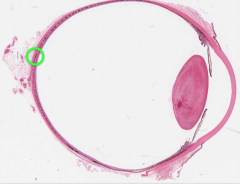
Eye Development Red: basal surface Green: apical surface Top to Bottom: Envagination of Diencephalon (top red arrow) Surface ectoderm Optic stalk: neuroepithelium Invagination of Ectoderm (bottom red arrow) Lense Vesicle Neural Retina Pigmented Epithelium |
|
|
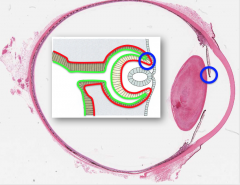
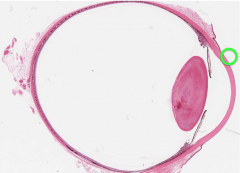
Developmental to Mature Eye Outer edge of the iris represents the margin of the optic cup having a double epithelium |
|
|
Cornea front of eye between pupil for accommodation and refraction continuous with sclera |
|
|
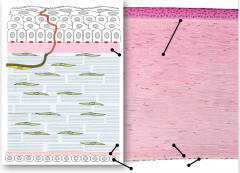
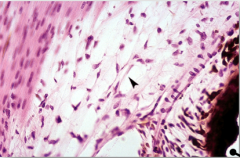
Top to Bottom: Dark pink top: Corneal Epithelium Bowman's Layer Middle: Stroma Descemet's Membrane Corneal Endothelium Cornea lined by stratified squamous cells No blood vessels or pigment Nutrients come through aqueous humor after ascending up from the endothelium Similar maturation in the skin desmosomes holding cells together Ferritin (has iron) in nuclei is for light absorption for UV protection (no melanocytes) Stroma: 60 thin layers of lamellae with collagen bundles of perpendicular orientation. There are fibroblasts in between. Desmet's membrane: basement membrane of endothelial cells where aqueous humor is and somewhat regenerates Endothelium: regulates fluid to stroma Turnover 7 days |
|
|
Corneal Epithelium |
Stratified squamous Attached to hemidesmosomes Innervated by unmyelinated axons |
|
|
Bowman's Layer |
Type I collagen barrier to trauma and bacterial invasion |
|
|
Stroma |
Collagen lamellae at an angle to one another Transparency depends on arrangement and affinity to water |
|
|
Decemet's Membrane |
Thick basement membrane Type IV collagen |
|
|
Corneal Endothelium |
Permeable to air Regulates hydration of stroma Vital to transparency of stroma |
|
|
Aqueous Humor |
made of water, AA, and glucose |
|

|
Top to Bottom: Cornea Canal of Schlemm Sclera Anterior chamber Iris Posterior Chamber |
|
|
Ciliary Muscle: accommodation of lens |
|
|
Trabecular Meshwork: draining aqueous humor into canal of schlemm |
|
|
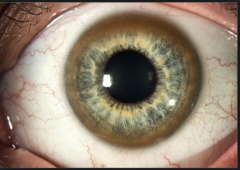
Kayser Fleischer Ring/Wilson's Disease autosomal recessive disease Copper deposits in Decemet's membrane |
|
|
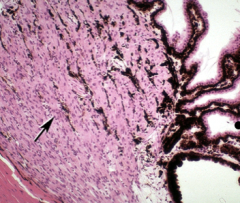
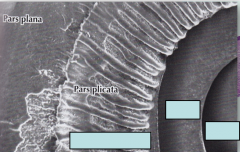
Limbus region and Ciliary Body Limbus region: where cornea meets sclera corneal epithelial stem cells and aqueous humor made here Ciliary Body: between iris and cornea creates aqueous humor anchors zonal fibers to change shape during lens accommodation |
|
|
Top to Bottom: Cornea Anterior chamber: from posterior chamber Canal of Schlemm: drains aqueous humor to control intraocular pressure Iris Posterior chamber: from ciliary body Lens Ciliary body: makes vitreous and aqueous humor Zonular fibers |
|
|
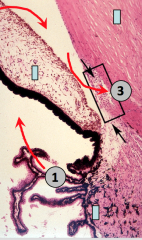
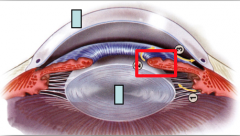
Top to Bottom: Cornea Iris Ciliary Body Arrows: Movement of Aqueous Humor 1. Ciliary body produces aqueous humor and moves into posterior chamber 2. Fluid moves around the iris into the anterior chamber 3. Fluid them moves into the Canal of Schlemm |
|
|
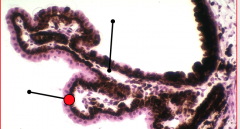
Top to Bottom: Ciliary Process: Fenestrated capillaries and attachment of lens Double Epithelium: Outer pigmented layer and inner ciliary epithlium |
|
|
Ciliary Muscle |
Contraction facilitates accommodation of lens attached to ciliary body (CN III parasympathetics) |
|
|
Posterior Chamber with Aqueous Humor (Zonula Fibers-lies on top of basal lamina for lens attachment; NOT shown in picture) Top to Bottom: Basal Lamina Ciliary Epithelium Ciliary Channel Pigmented Ciliary Epithelium Basal Lamina Fenestrated Capillaries |
|
|
Top to Bottom: Cornea Pupil Iris Lens |
|
|
Left to Right: Ciliary Process Iris Pupil |
|

|
Iris |
|
|
Top to Bottom: Cornea Red Box: Iris Lens |
|
|
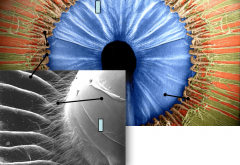
Top to Bottom: Dilator Pupillae (CN III Sympathetic- Internal Carotid Plexus and Ciliary Ganglion): Contraction increases diameter Sphincter Pupillae (CN III Parasympathetic Ciliary Ganglion): Contraction reduces diameter Melanocytes Lens |
|
|
Top to Bottom: Iris Ciliary Proccess Zonular Fibers: Lens attachment to ciliary process Lens |
|
|
Top to Bottom: Lens Arrows and Red box: Zonular fibers Ciliary Process |
|
|
Accommodation- Close Vision |
Ciliary muscle contracts Ciliary body and zonular fibers moves closer to lens Tension is reduced and lens rounds up |
|
|
Accommodation- Distant Vision |
Ciliary muscle relaxes Ciliary body and zonular fibers moves away from lens Tension increases and lens flattens |
|

|
Lens |
|
|
Lens Fibers |
metabolically active surrounded by lens capsule dividing cells near equatorial region anterior epithelium on top |
|
|
Equatorial Region |
of Lens Cells orient their long axis parallel to the surface Cells start producing lens specific filensins and crystallins Lens fibers move towards lens nucleus |
|
|
Top to Bottom: Anterior lens epithelium Lens capsule Cortical lens fibers Nuclear lens fibers |
|
|
Cataract Glucose is major metabolite of lens Diabetes cause sorbitol to accumulate in lens fibers Excess sorbitol reduces solubility of crystallins ->opacity must replace lens with artificial lens |
|
|
Retina |
|
|
Vitreous Body |
|
|
Vitreous Floaters |
|
|
Top to Bottom: Vitreous Body Retina: Neural Retina Retinal Pigment Epithelium Chorioid Bruch's membrane Choroidal Stroma Choriocapillaris Sclera |
|
|
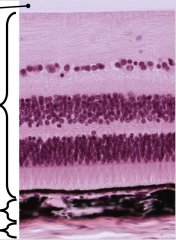
10 Retinal Layers |
Bottom to Top: 1. Retinal Pigment Epithelium 2. Photoreceptor: inner and outer segments 3. Outer Limiting Membrane 4. Outer Nuclear Layer 5. Outer Plexiform Layer 6. Inner Nuclear Layer 7. Inner Plexiform Layer 8. Ganglion Cell Layer 9. Nerve (Ganglionic Axon) Fiber Layer 10. Inner Limiting Membrane |
|

|
Bottom to Top: (Sclera) 1. Retinal Pigment Epithelium: squamous cuboidal epithelial 2. Photoreceptor: inner and outer segments 3. Outer Limiting Membrane: 4. Outer Nuclear Layer: rod and cone nucleus 5. Outer Plexiform Layer: axons of rods and cones 6. Inner Nuclear Layer: Muller (glial) and neuron (amacrine, bipolar, and horizontal) nucleus 7. Inner Plexiform Layer: Neurons connection to ganglionic cells 8. Ganglion Cell Layer: Ganglion nucleus 9. Nerve (Ganglionic Axon) Fiber Layer 10. Inner Limiting Membrane (Vitreous Fluid) |
|

|
Photoreceptors Rods and Cones More rods than cones but, organization is similar between two photoreceptors 4. Outer Plexiform Layer: axons from photoreceptors to neuron nucleus 3. Outer Nuclear Layer: photoreceptor nucleus 2. Outer Limiting Membrane: Photoreceptor inner and outer segment: photoreceptor bodies Photoreceptor outer body anchored to retinal pigmented epithelium |
|
|
Photoreceptors |
Rods- dim light, motion detection pigment: rhodopsin smaller nuclei Cones- color perception, most concentrated in fovea centralis iodopsin: blue, green, and red larger nuclei |
|

|
Rod Inner Segment Centriole Basal Body Modified Cilium Outer Segment: where light hits Modified Cilium Membranous Disks: engulfing Rhodopsin is bleached when light hits but, is recycled afterwards! |
|
|
In the Dark, Rods.. |
In the dark, outer segment of rod is depolarized and releasing neurotransmitter spontaneously Retinol and Opsin are inactivated High cGMP levels Inactive phosphodiesterase Sodium enters cell, Potassium leaves cell |
|
|
When light enters, Rods.. |
In light, outer segment of rod is hyperpolarized and action potential is created. Neurotransmitter is not released spontaneously. Light hits rhodopsin, activating opsin and creating retinol Phosphodiesterase in activated cGMP is decreased Sodium channels close, but, potassium still leaves cell, hyperpolarizing cell. |
|
|
Retinal Pigment Epithelium |
Supply nutrients to photoreceptors Phagocytose outer segments of photoreceptors Prevent internal light reflection Conversion of retinol to retinal Basement membrane: Bruch's membrane - where macular degeneration occurs Choroid fenestrated capillary underneath basement Bruch's membrane brings nutrients to RPE |
|
|
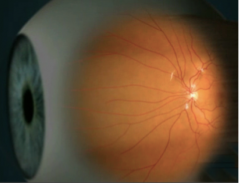
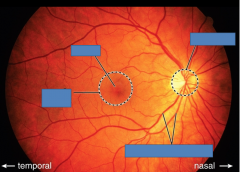
Top to Bottom: Optic Disc Fovea Macula lutea Central retinal vessels |
|
|
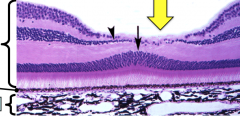
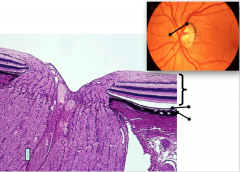
Fovea Centralis- only conestightly packed cones arrange in an angle; highest area of color vision Nuclear layers don't obstruct light path (squished) Top to Bottom: Neural Retina Retinal Pigmented Epithelium Choroid |
|
|
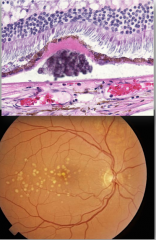
Age Related Macular Degeneration: leading cause of vision loss Bruch's membrane thickens Wet type: has neovascularization- blood vessels coming from Choroid Dry type: most common; drusen (extracellular debris) accumulates in between the choroid and the RPE |
|
|
Retinal Detachment |
|
|
Large Retinal Detachment |
|
|
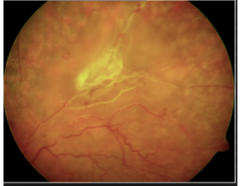
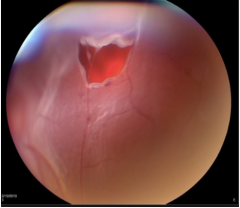
Retinal Detachment and Tear Vitreous has pulled away from the retina Laser repair if caught quickly |
|
|
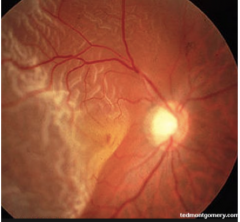
Optic Disc: BLIND SPOT Entrance of retinal blood vessels Exit of (optic nerve) ganglionic cell axons Neural Retina, RPE, and Choroid do not exist at optic disc; they stop to make way for optic nerve within the disc |
|
|
Eye Lid Top to Bottom: Palpebral par of Obicularis oculi (skeletal muscle) Sweat gland Tarsal Plate (fibroelastic tissue) Tarsal glands (Meibomian glands) Eye lashes with sebaceous glands Smooth Conjuctiva: stratified columnar epithelium |
|
|
Lacrimal Gland: tubulo-acinar serous glands produce tear film tears drain into nasal cavity via naso-lacrimal sac |
|

|
Chalazion: sebaceous glands get clogged and sebum blocked from moving out |
|

|
Chalazion: sebaceous glands get clogged and sebum blocked from moving out |
|

|
Left to Right: Aorta- oxy blood to tissues Arteries- oxy blood to tissues Arterioles oxy blood to tissues Capillaries (gas exchange with tissues) Venules -deoxy blood back to heart Veins-deoxy blood back to heart Vena Cava-deoxy blood back to heart |
|
|
Pulmonary Artery vs. Pulmonary Vein |
Only artery and vein that do opposite of what they normally do Pulmonary Artery- brings deoxygenated blood to lungs to be reoxygenated from right ventricle Pulmonary Vein- brings oxygenated blood back to left atrium from lungs |
|
|
Arteries Arterioles Metarterioles |
Arteries: elastic (changes tension to equalize pressure through body and muscular): distribute blood from heart to tissues Arterioles and Metarterioles: regulate blood flow |
|
|
Capillaries |
Capillaries: metabolic exchange 3 kinds: continuous, fenestrated, discontinuous |
|
|
Veins Venules Postcapillary Venules |
Veins (small, medium, and large) and Venules: collect and return blood to heart from tissues Postcapillary Venules: extravasation of fluid and leukocytes/drains oxygen back from capillaries |
|
|
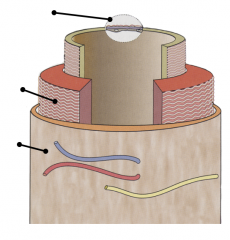
Muscular Distributing Arteries structure- Top to Bottom: Tunica Intima: Internal elastic lamina Subendothelial layer Endothelium Tunica Media: Smooth muscle cells producing elastic, reticular, and collagen fibers Tunica Adventitia: Connective tissue containing blood vessels (Vasa Vasorum) and nerves |
|
|
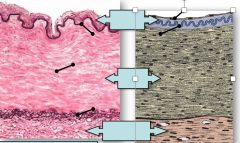
Muscular Distributing Arteries Top to Bottom: Endothelium (right drawing) Intima Internal Elastic Lamina Media Smooth Muscle (right drawing) Elastic Fiber External Elastic Lamina Adventitia Connective tissue |
|
|
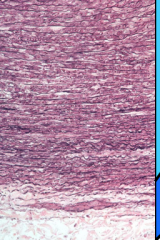
Elastic Artery Structure: Top to Bottom: Tunica Intima: more connective Tunica Media: elastic and fibrous Elastic lamina |
|
|
Elastic Artery Structure: Top to Bottom: Tunica Media: elastic and fibrous Tunica Adventitia |
|

|
Elastic (laminae) sheets Prominent in elastic arteries and maintain blood pressure during diastolic recoil |
|
|
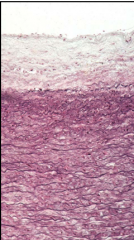
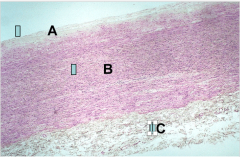
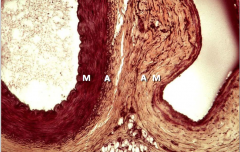
Elastic Artery: Aorta Top to Bottom: A: Tunica Intima B: Tunica Media C: Tunica Adventitia |
|
|
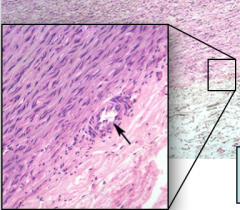
Elastic Artery: Aorta Arrow: Vasa Vasorum in Tunica Media |
|
|
Muscular Artery vs. Accompanying Vein |
Oxygenated blood vs. Deoxygenated blood Thicker vs. Thinner wall Bigger Media with more Elastic fibers vs. smaller Media with less Elastic fibers Smaller Adventitia vs. Larger Adventitia |
|
|
Left: Large Muscular Artery Right: Accompanying Vein M: Media A: Adventitia |
|
|
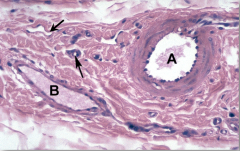
Left: Accompanying Vein Right: Medium Muscular Artery |
|
|
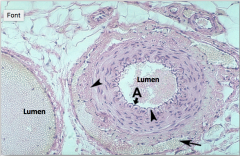
Between arteriole and venule, is a capillary bed Arrows: Top: Venule Bottom: Arteriole- thick wall; large resistance to blood flow for larger oxygen unloading |
|
|
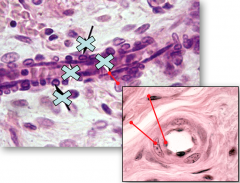
Small Arteriole Red Lines Top to Bottom: Endothelium Smooth Muscle |
|
|
All blood vessels are lined by endothelial cells- tiny flat cells covering entire lumen of vessel barrier for blood to stay in lumen controls intestinal fluid provides white blood cells angiogenesis site- new blood vessels come out of endothelial cells signals the change in smooth muscle cells to control blood pressure |
|

|
Transcellular molecular traffic across cardiac endothelium |
|
|
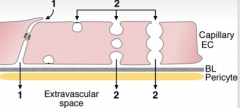
Cardiac Endothelium Transport to Extracellular Space 1. Paracellular molecular traffic: trough cell-cell junctions 2. Transcellular molecular traffic: vesicular transport |
|
|
Endothelial cell function |
1. Regulate blood coagulation: separates tissue factor starting coagulation cascade 2. Modulate smooth muscle contractibility: in heat, vasodialator; in cold, vasoconstrictor 3. regulate leukocyte traffic into tissues for pathogenic response |
|
|
Atheroma Formation leading to.. |
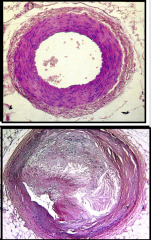
Atherosclerosis 1. Accumulation of oxidized lipids in the tunica intima 2. Infiltration of inflammatory cells 3. Proliferation of smooth muscle cells 4. Synthesis of collagen, necrosis, and calcification if vessels supply heart, then will lead to heart attack |
|
|
Coronary Artery: Top: normal Bottom: atherosclerotic, almost total occluding of the lumen (need stent or cardiac bypass) |
|
|
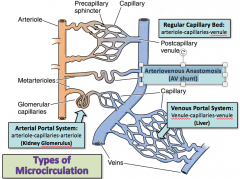
Types of Microcirculation |
Regular Capillary Bed: arteriole-capillaries-venule Ateriovenous Anastomosis: AV shunt Venous Portal System: Venule-capillaries-venule (liver) Arterial Portal System: arteriole-capillaries-arteriole (kidney glomerulus) |
|
|
Types of Microcirculation |
|
|
|
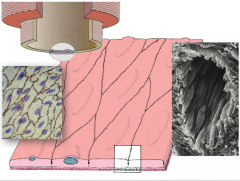
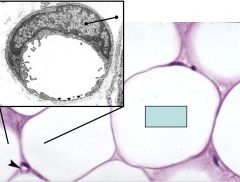
Capillary walls only consist of endothelium Top to Bottom: Endothelial cell nucleus Adipocyte Capillary |
|
|
Continuous Capillary Arrows: Tight Junctions highly selective for gas exchange lung, brain, testis |
|

|
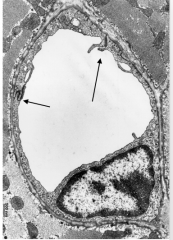
Fenestrated Capillary (leaky) selective barrier with filtration intestine, kidney |
|

|
Discontinuous Capillary Poorly selective with large gaps for passage of large molecules liver, spleen |
|
|
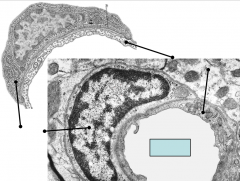
Top to Bottom: Pericytes Endothelium Pericyte Processes |
|
|
Pericytes: stem cells that give rise to endothelial cells, smooth muscle cells, and fibroblasts Top to Bottom: Endothelial Cell Pericyte Capillary lumen |
|
|
Valves in Veins only blood goes back to heart, does not leak backwards |
|
|
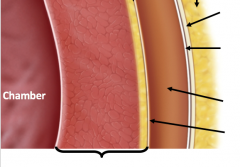
Coverings of the Heart Top to Bottom: Epicardium Adipose (large yellow outer layer) Fibrous Pericardium: dense irregular connective tissue Parietal layer of serous pericardium: mesothelium Pericardial Cavity: fluid filled space fill with blood or constrict and could kill you Visceral layer of serous pericardium: mesothelium Wall of heart (myocardium) |
|
|
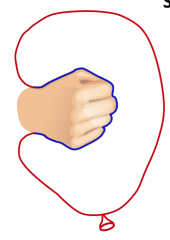
Red: Parietal Pericardium Blue: Visceral Pericardium Hand=heart; goes into ballon |
|
|
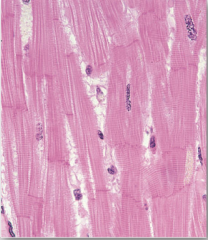
Myocardium -intercalated discs, connecting muscle cells -striations -perinuclear spaces -branched fibers |
|
|
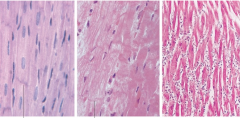
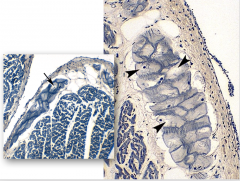
Left: normal myocardium- can see nuclei and striations clearly Middle: Myocardial ischemia- no more filaments, pyknotic nuclei Right: 3 days post MI- neutrophils eating dead tissue. Fibroblasts will follow black lines: intercalated discs |
|
|
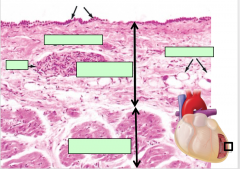
Top to Bottom: Mesothelium Connective tissue Adipose tissue Nerve Epicardium- first layer Myocardium- 2nd layer; more muscular |
|
|
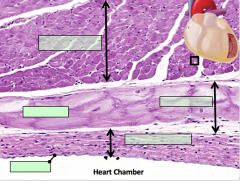
Top to Bottom: Myocardium- 1st layer Purkinje Fibers- pacemakers Subendocardial layer- 2nd layer: loose CT Endocardium- 3rd layer Epithelium |
|
|
Conduction |
Spread of Conduction: 1. SA pacemaker, starts electrical impulse 2. AV 3. Purkinjie fibers |
|
|
Purkinje Fibers |