Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
26 Cards in this Set
- Front
- Back
|
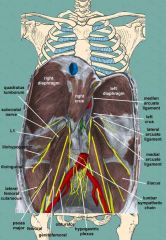
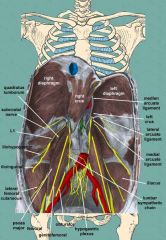
Traumatic rupture of the diaphragm is most common @ which location? |
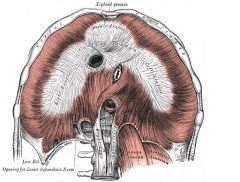
Traumatic rupture of the diaphragm: ~1% of thoracic trauma, up to 8% of those requiring laparotomy.
-high energy injuries, usually MVCs. LEFT 2x more common than R. Usually tears in a radial orientation along the weak posterolateral aspect of L hemidiaphragm -Sx: epigastric and abdominal pain, referred shoulder pain, SOB, vomiting, dysphagia, or shock. -Initial CXR is nondiagnostic in up to 50 %. -Collar sign = focal constriction of herniated viscera at the site of the tear, producing circumferential compression. -Acute diaphragmatic injuries are best managed through an abdominal approach |
|
|
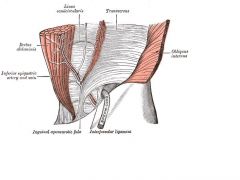
what are the borders of the femoral canal?
|
Femoral canal:
Superior: inguinal ligament Medial: lacunar ligament (from inguinal ligament to the pectineal ligament; part of ext oblique aponeurosis) Lateral: femoral vein -Posterior (floor): iliacus + psoas tendons, pectineal AKA Coopers ligament (extension of the lacunar ligament that runs on the pectineal line of the pubic bone) |
|
|
65M presents c/ tender mass below the inguinal ligament
-Suspect _ -Tx is _ |
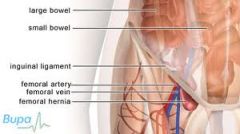
Femoral hernia:
-M>F -Bulge on the anterior-medial thigh below the inguinal ligament, medial to femoral vein, lateral to lymphatics (in empty space) -Femoral canal bounderies: Cooper's ligament, inguinal ligament, femoral vein (Poupart's ligament is medial) -High risk of incarceration => may need to divide inguinal ligament to reduce the bowel, then repair the ligament -Hernia usually repaired through an inguinal approach c/ McVay or Bassini repair (suprainguinal groin incision) |
|
|
The lateral boundary of a femoral hernia sac is formed by _
|
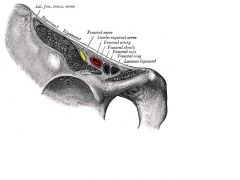
Femoral hernias develop in an empty space at the medial aspect of the femoral canal after passing through the femoral ring (navEl). The boundaries of the sac include: medial - lacunar ligament, lateral - fascia on the femoral vein, anterior - inguinal ligament, and posterior - fascia on the pectineus muscle.
|
|
|
The nerve injury associated with laparoscopic preperitoneal inguinal hernia repair is _
|
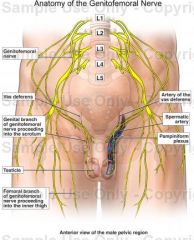
Genitofemoral nerve.
-Genital branch runs on spermatic cord to cremaster (motor) and scrotum (sensory ) -Femoral branch: sensory to upper lateral thigh |
|
|
What is the most likely etiology of small bowel obstruction in a 50 year old obese female with no previous abdominal surgery?
|
Incarcerated groin hernia
|
|
|
Congenital condition _ results from ischemia of the right omphalomesenteric artery
|
Gastroschisis:
Intrauterine rupture of umbilical vein before collateral circulation is established, and ischemia of the R omphalomesenteric artery (OMA) -> mesodermal and ectodermal defects. -Disruption of the distal segment of the right OMA -> R paraumbilical ischemia -> paramedian defect. -After infarction, the bowel herniates through the necrotic abdominal wall and enters the amniotic cavity. -Further SMA ischemia => high incidence of concomitant JEJUNAL ATRESIA -10% rate of congenital anomalies, esp. malrotation (vs. 50% c/ omphalocele) |
|
|
what hernia goes through defect made by 12h rib, internal oblique, and lumbosacral aponeurosis
|
Grynfelt's hernia = superior lumbar hernia
-Internal ab oblique, lumbodorsal aponeurosis, and 23th rib (or posterior lumbocostal ligament) |
|
|
what are the borders of hesselbach's triangle?
|
Rectus abdominis muscle (medially)
Inferior epigastric vessels (superior and laterally). Inguinal ligament AKA Poupart's ligament (inferiorly) |
|
|
old lady presents c/ inner thigh pain c/ internal rotation. this is _
|
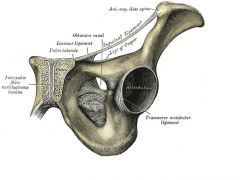
Obturator hernia:
-Howship-Romberg sign = inner thigh pain c/ internal rotation -X-ray: bowel gas below superior pelvic ramus -5:1 women: men -Tx: operative reduction +/- mesh. check other side for similar defect. may find bowel obstruction in OR. |
|
|
Patient presents after inguinal hernia repair c/ numbness on ipsilateral penis, scrotum, and thigh. Loss of cremasteric reflex.
-The _ nerve was injured, most likely @ landmark _ |
Ilioinguinal nerve:
-traverses inguinal canal. runs on top of cord. -Sensation to supero-medial thigh and scrotum -Injury (usually @ external ring) -> loss of cremasteric reflex. numbness on ipsilateral penis, scrotum, thigh |
|
|
pt c/o pain following inguinal hernia repair.
-Suspect _ -_ can be diagnostic and therapeutic |
Inguinal hernia repair ->
compression of ilioinguinal nerve (branch of L1) -> PAIN -Local infiltration can be diagnostic, therapeutic |
|
|
#! Complication following inguinal hernia repair = _
|
Inguinal hernia repair:
-Urinary retention = #1 early post-op complication (RFs: old, male, narcotics) -2% wound infection, 2% recurrence -Spematic cord venous thrombosis in indirect hernia repair -> Testicular atrophy -Pain 2/2 compression of ilioinguinal nerve (runs on top of cord, usually injured @ external ring) -> loss of cremasteric reflex, thigh/scrotum numbness -Genitofemoral nerve injury: usually c/ laparoscopic hernia repair |
|
|
Testicular atrophy following inguinal hernioplasty is usually due to _
|
Testicular atrophy following inguinal hernioplasty is usually due to thrombosis of the veins in the spermatic cord
|
|
|
What is the rate of recurrence with Lichtenstein repair of inguinal hernia?
|
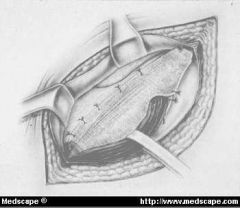
recurrence <1% for Lichtenstein repair. Some investigators, however, have reported 0.2% recurrence rate with mesh plug repair.
-Tension free synthetic mesh repair also has a reported recurrence rate of less than 1%. The recurrence rate for laparoscopic repair performed by experienced surgeons is reported to be around 1%. Lichtenstein: Mesh is sutured from the transversus arch to the shelving edge of the inguinal ligament creating a "tension-free" repair. |
|
|
what is the #1 abdominal hernia?
|

Abdominal hernias develop in nearly 5% of the world population over a lifetime. Inguinal hernias are the most common abdominal wall hernias and constitute about 80% of the total cases. Femoral hernias are found in approximately 5%, while incisional, umbilical, epigastric, and other miscellaneous hernias make up the other 15%. Most inguinal hernias are found with a male to female ratio of 7:1. Femoral hernias have a female dominance of approximately 1.8:1.
|
|
|
At reoperation for inguinal hernia recurrence following laparoscopic repair, #1 location for recurrence = _
|
Inguinal hernia recurrence s/p laparoscopic repair:
-Most commonly @ medial portion of mesh, usually b/c mesh is too small > failure to attach mesh appropriately on medial aspect |
|
|
What is the most commonly injured nerve in inguinal hernia repair:
|
Inguinal hernia repair:
-Ilioinguinal = most common nerve injury (runs on top of cord, usually injured @ external ring) -> loss of cremasteric reflex, thigh/scrotum numbness -Genitofemoral nerve injury: usually c/ laparoscopic hernia repair -> genital branch => cremaster (motor), scroum (sensory); Femoral branch => upper lateral thigh (sensory) |
|
|
complication of laparoscopic indirect inguinal hernia repair that is most frequently ass'd c/ signficant post-op pain
|
entrapment of the lateral femoral cutaneous nerve = complication of laparoscopic indirect inguinal hernia repair that is most frequently ass'd c/ signficant post-op pain
-Pain in lateral thigh -arises from the dorsal divisions of the second and third lumbar nerves (genitofemoral also arises from these) |
|
|
60M presents with pain in his long standing inguinal hernia. The ER resident reduces the hernia with difficulty and sends the patient home. The patient presents again a few hours later with hypotension, tachycardia and localized tenderness in the lower quadrant, but without hernia. What is the likely diagnosis?
|
Maydl's hernia = strangulated bowel within the abdominal cavity, with the loops of the intestines forming a W
2 adjacent loops of small intestine are within a hernial sac with a tight neck. The intervening portion of bowel within the abdomen is deprived of its blood supply and eventually becomes necrotic. |
|
|
Pt presents c/ tender medial thigh mass
-Pain increases c/ medial thigh rotation -Suspect _ -Tx is _ |
Obturator hernia: anterior pelvis
-Xray: bowel gas below inferior pubic ramus -Howship-Romberg sign = pain c/ internal thigh rotation -RFs: elderly women, previous pregnancy -Bowel gas below superior pubic ramus -Tx: operative reduction (inguinal approach requires incision in the inguinal floor = transverse fascia), may need mesh; check other side for similar defect -Diagnosis usually made @ time of surgery for SBO |
|
|
How does an obturator hernia commonly present?
|
Obturator hernias:
- Age 60+. 9x more common in females (large, wide pelvic bones and more horizontally oriented obturator canals). -RFs: thin, prior pregnancy, chronic illness, malnutrition, -Protrude through the obturator foramina: anterolateral pelvic wall immediately inferior to the acetabula. -SBO = #1 symptom. May be mild + intermittent. -Related physical findings are rare since the incarcerated hernia is located posterior to the pectineus and adductor longus muscles. -Howship-Romberg sign in 50%= pain along the medial aspect of the thigh, extending to the knee, 2/2 irritation of the obturator nerve. -CT plays an important role in the diagnosis of obturator hernia by demonstrating incarcerated small bowel posterior to the pectineus muscle. -Tx: laparotomy and repair of the hernia defect. |
|
|
Petit's hernia (inferior lumbar hernia) goes through triangle made by what 3 anatomic strucures?
|
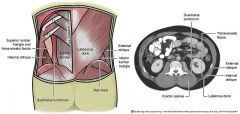
Petit's hernia:
-inferior lumbar triangle (ilaic crest, ext oblique, lat dorsi) -lmakes a preety large defect, so lower risk of strangulation |
|
|
What is the most common organ involved in sliding hernia in men?
|
Sliding hernia: A VISCERAL WALL MAKES UP PART OF THE SAC
-occurs when an organ drags along part of the peritoneum, i.e. the organ is part of the hernia sac. -Women, OVARY (or fallopian) tubes = most common (=> ligate the round ligament, return ovary to peritoneum, bx if it looks abnormal) -Men: CECUM OR SIGMOID = most common -Bladder also commonly involved |
|
|
What is the most common organ involved in sliding hernia in women?
|
Sliding hernia: A VISCERAL WALL MAKES UP PART OF THE SAC
-occurs when an organ drags along part of the peritoneum, i.e. the organ is part of the hernia sac. -Women, OVARY (or fallopian) tubes = most common (=> ligate the round ligament, return ovary to peritoneum, bx if it looks abnormal) -Men: CECUM OR SIGMOID = most common -Bladder also commonly involved |
|
|
_ hernias almost always develop at or below the arcuate line = linea semicurcularis
|
Spigelian hernia or lateral ventral hernia arise through the spigelian fascia, = aponeurotic layer between the rectus abdominis muscle medially, and the semilunar line laterally.
-Develop at or below the arcuate line (linear semicircularis) 2/2 lack of posterior rectus sheath. - interparietal = do not lie below the subcutaneous fat but penetrate between the muscles of the abdominal wall; therefore, there is often no notable swelling. Sx: intermittent mass, localized pain, or signs of bowel obstruction. -Dx: US, CT (more sensitive and specific) -Tx: surgery b/c high risk of strangulation. |