Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
90 Cards in this Set
- Front
- Back
|
MCV
|
hct / RBC
|
|
|
MCH
|
hgb/RBC
|
|
|
MCHC
|
hgb/hct
|
|
|
HbA
|
α2β2
|
|
|
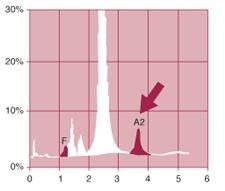
HbA2
common situation this is increased? |
α2δ2 (delta)
beta-thal |
|
|
HbF
|
α2γ2 (gamma)
|
|
|
HbS
|
α2βs2
|
|
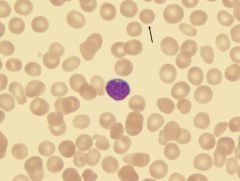
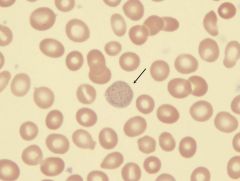
What is this called?
What RBC parameters are affected? Causes? |
Spherocyte
Loss of membrane without volume loss MCHC is increased Osmotic fragility is increased HS, warm aiha, old blood, burn, venom, oxidant damage |
|
|
How is HS inherited & what is the defect?
|
AD
Defect in spectrin / ankyrin RBC membrane protein (ankyrin is MOST COMMON, chrom 8) |
|
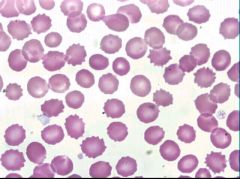
Name?
Causes? |
Echinocyte (Burr cell)
ACUTE RENAL FAILURE Acidic environment; sitting in EDTA too long "Prickle cells" of pyruvate kinase deficiency |
|
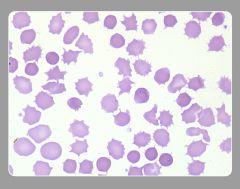
Name?
How is this different than burr cell? Seen in what 3 classic pictures? |
Acanthocyte (Spur cell)
Irregular, fewer, blunted projections LIVER DISEASE Kx deficiency (McLEOD PHENOTYPE) aB-lipoproteinemia -also in hypothyroid, MDS |
|

Name?
Seen in? |
Codocyte (target cell)
too much membrane = decreased osm fragility Seen in: Asplenia IDA Liver disease Hemoglobinopathies |
|
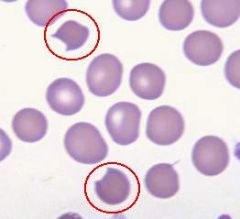
Name?
Classically seen in? |
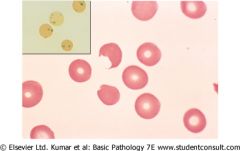
Bite cell
Seen in cases of oxidative damage (G6PD!!!!!!) (spleen bites out Heinz bodies) |
|
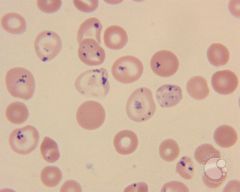
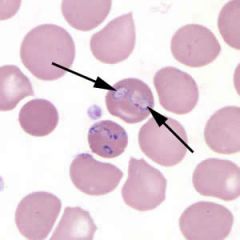
How to tell normal from pathologic?
Classically seen in? |
Basophilic stippling
- Reticulocytes have small fine blue dots; pathologic states tend to be coarser LEAD POISONING Pyrimidine 5' nucleotidase deficiency MDS Infection Sideroblastic anemia Porphyria |
|
Seen in?
|
Howell Jolly bodies
-DNA / nuclear remnant; 3D; peripheral -Spleen normally bites these out Indicate asplenia (functional or real) -SCD, neuroblastoma, IBD, GVHD, ai) |
|
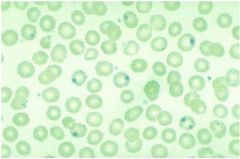
What are these made of?
|
pappenheimer bodies
multiple. See with Howell-Jolly. IRON See with asplenia; iron overload |
|
What are these and what stain is this?
|
Heinz bodies
See with reticulin stain - don't see with Wright Giemsa Represent oxidized hemoglobin: G6PD, unstable hgb, 3deletion alpha thal Bite cells have them bitten out |
|
|
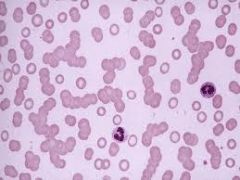
Rouleaux
secondary to large proteins: fibrinogen, immunoglobulin |
|
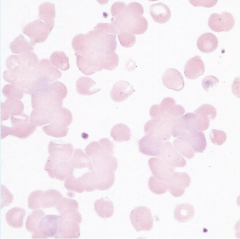
How is this different than rouleaux?
causes? How to correct? What indices will be changed? |
Autoagglutination
RBC clumping COLD AGGLUTININS (IgM autoantibody: EBV, mycoplasma) Correct by warming increased MCV, decreased RBC |
|
|
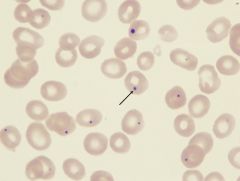
Babesia
Babesia parasites resemble Plasmodium falciparum, however Babesia has several distinguishing features: the parasites are pleomorphic (vary in shape and size), can be vacuolated, and do not produce pigment. Can be extracellular |
|
|
Vector for babesia?
|
IXODES DAMMINI (same as Lyme)
|
|
|
Fast migrating Hb?
|
J N I H Barts
|
|

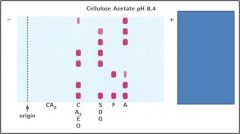
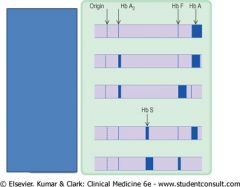
Alkaline hgb electrophoresis
What are the bands? |
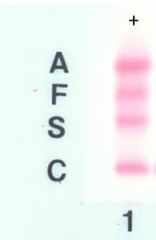
AFSC
A Fat Santa Claus |
|
|
What classically migrates with S in alkaline?
|
S D G Lepore
|
|
|
What classically migrates with C on alkaline?
|
C E O A2
Also C-Harlem |
|
What does the star represent?
|
Fast migrating hemoglobins (JNIHBarts)
|
|
|
What is a classic slow-migrating hemoglobin on alkaline?
|
Constant Spring
|
|

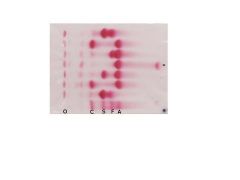
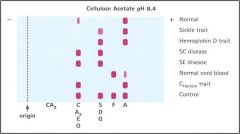
Acid hb electrophoresis. What are the bands?
|

F A S C
Lots migrate with A... |
|
The patient is in lane 1. There was an abnormal hemoglobin on alkaline gel in the C lane. What is it?
|
Hemoblobin E.
The abnormal hemoglobin migrates as Hb C on cellulose acetate and as Hb A in acid agar. Diagnosis : Hb E trait (heterozygote for Hb E) Comment : Hb E is very common among southeast Asians. |
|
|
African American with jaundice after fava beans
disease? Inheritance? Triggers? |
G6PD
10% Af Amer (wildtype is type B***) Susceptible to oxidative damage; Heinz bodies, hemolysis RETICULOCYTES ARE NORMAL XR (boys) Triggers: fava beans, sulfa drugs, antimalarials, infxn (hepatitis, pna, thyroid) COOMBS TEST IS NEGATIVE G6PD protects against malaria! |
|
|
Thal minor
Inheritance? Clues? |
One damaged Beta chain
AR chrom 11 Microcytic anemia with increased RBC (MCV/RBC<13) HbA2 > 3.5% (vs IDA!!) |
|
|
Thal major, a.k.a...?
Population? Inheritance? Clues? Clues? |
Cooley's anemia
2 damaged B chains AR, Chrom 11, Mediterranean Marked anisopoikilocytosis Splenomegaly, death < 20y |
|
|
Inheritance of alpha thal?
|
AR chrom 16
|
|
|
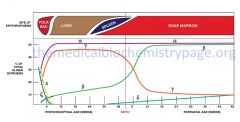
Why is beta-thal picked up in the first year of life while alpha-thal is diagnosed in utero?
|
Because B thal can make HbF, which is normal at birth. Beta chain production (and hence hgb A) is not predominant right away.
vs. Alpha thal: alpha chain is required for all types of hgb |
|
|
Hgb types in B thal minor
Major? |
HbF < 5%
HbA2 4-10% Major: HbF 90% |
|
|
1-deletion alpha thal
|
silent carrier
slight decreased MCV, MCH |
|
|
2 deletion alpha thal
Does it matter if it is -/- a/a or -/a -/a? |
"alpha thal trait"
Mild microcytic anemia -/- a/a seen in Chinese -/a -/a in African Americans matters for inheritance |
|
3-deletion alpha thal
|
get tetramers. microcytic anemia. Heinz bodies. Splenomegaly.
HbH (4 beta chains) (GOLF BALLS) and HbBarts (gamma x 4)(normally in HbF) -both have HIGH affinity for O2 |
|
|
4-deletion alpha thal
|
No alpha chains.
HbBarts (tetrameric gamma) Fatal Hydrops fetalis |
|
|
Hemoglobin that is made of 2 alpha chains and 2 delta-beta fusion chains?
What does it mimic? |
Hemoglobin Lepore
Mimics thal trait (B thal minor) |
|
|
delta-beta thalassemia
|
deletion of both delta and beta chains on chrom 11
heterozygous (~thal minor) or homozygous (~thal intermedia) also known as "F thalassemia" since there are no A or A2 hemoglobins produced (since no delta or beta), they have only F |
|
|
How to tell hereditary persistance of fetal hemoglobin vs. delta-beta thal?
|
Both have increased HbF!!!!!!
BUT delta-beta thal will have decreased total hemoglobin resulting in a low MCV, low MCHC, high normal to elevated erythrocyte counts and often low or low normal HbA2. In contrast, in HPFH the total amount of hemoglobin produced is sufficient to prevent these abnormalities |
|
|
Heterozygous beta thal
|
|
|
nice graphic
|
|
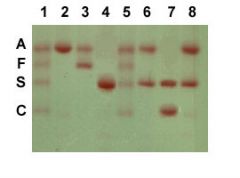
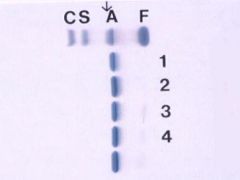
name the lanes
|
Lanes 1 and 5 are hemoglobin standards.
Lane 2 is a normal adult. Lane 3 is a normal neonate. Lane 4 is a homozygous HbS individual. Lanes 6 and 8 are heterozygous sickle individuals. Lane 7 is a SC disease individual. |
|
|
Ratio of HbA to HbS in heterozygous SA? Homozygous SS?
|
60%A, 40% S
>80%S |
|
|
Classic cause of aplastic crisis in SCD?
|
Parvovirus
|
|
|
HbS is made of what hemoglobin chains?
What would happen in S/alpha-thal? S/beta thal? |
alpha x 2
abnormal beta x 2 S/alpha thal: Decreased S (because need alpha chain) S/beta thal: Increased S (because you can't make HbA, and you can make SOME S) |
|
|
For what 2 purposes would you do iron studies in thalassemias?
|
1. To differentiate btwn Fe defic. anemia and Beta thal minor
2. To evaluate iron overload in Thal major. |
|
|
What symptoms do you see in HbE?
population? |
None.
HbE is one of the most rare variants of normal hemoglobin. COMMON IN SE ASIA |
|
HbC
|
reduces the normal plasticity of host erythrocytes causing a hemoglobinopathy.
In those who are heterozygous for the mutation, about 28–44% of total hemoglobin (Hb) is HbC, and no anemia develops. In homozygotes, nearly all Hb is in the HbC form, resulting in mild hemolytic anemia. = MILD DISEASE TARGET CELLS, CLAM CELLS, CRYSTALS |
|

What is the paradox in this disease?
|
hemoglobin SC disease
Targets, sickles, and crystals Paradox: usually have LESS sickled cells, but higher incidence of complications |
|
|
RBC lifespan in HbS?
|
30 days
|
|
|
Things that increase hemoglobin affinity for O2?
LEFT SHIFT |
HbF
Cape Town, Chesapeake, Bethesda Alkalosis Hypothermia |
|
|
Things that decrease hemoglobin affinity for O2?
RIGHT SHIFT |
Acidosis
Hyperthermia 2,3-DPG Kansas, Providence, Seattle, Beth Israel |
|
|
Unstable hemoglobins (prone to precipitate)
|
Kolu, Hasharon, Zurich
(Heinz body --> hemolysis) Dx with heat instability test, isopropanol, n-butanol test |
|
|
CO-hb
|
Increased O2 binding x 200
Cherry pink blood and skin NO CYANOSIS |
|
|
HbM mechanism
|
= methemoblobinemia
higher than normal level of methemoglobin (metHb, i.e., ferric [Fe3+] rather than ferrous [Fe2+] haemoglobin) DECREASED OXYGEN BINDING CYANOSIS |
|
|
HbM types
|
1: congenital. deficiency methemoglobin reductase (may also see with pyruvate kinase def)
2: Ingestion of oxidizing agents: MOTH BALLS, ANTIFREEZE 3: Inherited: Hg Boston, Saskatoon, Milwaukee |
|
|
Drugs that cause HbM
|
Nitrates
Benzocaine Dapsone antibiotics (trimethoprim, sulfonamides and dapsone), local anesthetics (especially articaine and prilocaine), and others such as aniline dyes, metoclopramide, chlorates and bromates. infants under 6 months of age are particularly susceptible to methemoglobinemia caused by nitrates ingested in drinking water (called blue-baby syndrome) |
|
|
HbM treatment
|
Reducing agents
methylene blue ascorbic acid |
|
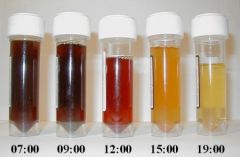
what is this test and what is it used to dx?
|
Ham test
PNH Urine passed 7am is dark containing a large amount of free haemoglobin which leaks out of PNH red-cells as they burst. The urine generally clears during the day. |
|
|
Genetics of PNH and pathophys?
|
Acquired stem cell disorder
Mutant PIG-A gene on chrom 22 Lose GPI anchor and therefore lose expression of membrane proteins loss of CD55/DAF --> complement mediated lysis Intravascular hemolysis, thrombocytosis, bone marrow failure IRON DEFICIENCY |
|
|
Anti-i seen in?
Anti-I? clinical pic? |
anti-i : EBV
anti-I: Mycoplasma pna Cold autoimmune hemolytic anemia. IgM!!!!! |
|
|
What is Donath-Landsteiner hemolytic anemia?
Classic triggers? |
PCH (paroxysmal COLD hemoglobinuria)
a polyclonal IgG anti-P autoantibody binds to red blood cell surface antigens in the cold. anti-P seen in Mumps, Measles, Mono, syphilis usually self limited |
|
|
What is anti-P seen in?
|
PCH
|
|
|
Renal abnormalities
cafe au lait spots Mental retardation Short stature NO THUMB increased risk AML & solid tumors |
Fanconi anemia
AR Pancytopenia (****) at 5-10y |
|
|
Pica, glossitis, esophageal webs
|
Iron deficiency anemia
Can cause THROMBOCYTOSIS and HYPERSEGMENTED NEUTROPHILS |
|

|
Hookworm
Ancylostoma duodenale (one of 2 that infect humans) Cause IDA by attaching to intestintal wall and sucking blood A. duod has 2 pairs of teeth, which ID it from Necator |
|

|
Necator americanus, the other hookworm that infects humans.
Cutting plates on mouth |
|
|
Elevated adenosine deaminase
Short stature, <1y.o. Malfunctioning ribosomal proteins RPS19 gene |
Diamond Blackfan anemia
RBC aplasia |
|
|
Acquired causes of RBC aplasia?
|
Thymoma
Parvovirus autoimmune drug malignancy infection |
|
|
Schilling test
|
used for patients with vitamin B12 deficiency. The purpose of the test is to determine whether the patient has pernicious anemia. many parts to it!
|
|
|
Megaloblastic anemia
Achlorhydria Sensitive test? Specific test? |
Pernicious anemia
(chronic atrophic gastritis) attack parietal cells; get low acid; get hypergastrinemia leading to achlorhydria anti-parietal cell (sens) anti-IF (specific) |
|
|
Which is better to measure folate deficiency: Serum folate or RBC folate?
|
RBC FOLATE!
sources of folate: leafy greens, EtOH, short bowel syndrome |
|
|
B12 deficiency
|
elevated homocysteine
elevated MMA can be caused by diphyllabothrium latum can cause infertility |
|
|
Anemia of chronic disease
|
Low iron
low transferrin HIGH FERRITIN |
|
|
Sideroblastic anemia treatment?
causes? |
B6
Tb drugs Pb poisoning EtOH Zinc |
|
|
Mechanism of Pb poisoning
|
Blocks ALA synthetase, ALA dehydrase, heme synthetase
increased protorphyrin |
|
|
What migrates with A on hemoglobin electrophoresis in acid?
Where does O go? What migrates with S? |
A, A2, D, E, G, M
(M also migrates with A on alkaline) O stays at the origin in acid C-Harlem migrates with S on acid (migrates with C on alk) |
|
|
Where is the origin on hemoglobin electrophoresis?
|
Alk: at the cathode (-). all flow to the (+)
Acid: in the middle. C & S flow to (+), F & A to (-) |
|
|
What is another way to identify hemoglobinopathies?
|
HPLC
Also: PCR (useful in fetal cases - don't need fetal blood can use any tissue) |
|
Name the rows
|
|
|
Name the rows
|

|
|
|
True or false: Therapeutic splenectomy is generally avoided in Hereditary stomatocytosis.
|
True - there is a marked tendency towards thrombosis following splenectomy
|
|
|
What Rh phenotype is associated with hereditary stomatocytosis?
|
Rhnull
|
|
|
The cytoskeletal disorders of RBCs are inherited in what manner?
|
AD
|
|
|
Splenomegaly is common in all chronic hemolytic disorders except?
|
Sickle cell disease
|
|
|
EPO-secreting neoplasms?
|
RCC
Hemangioblastoma Leiomyomas of the uterus HCC |
|
|
Causes of reactive erythrocytosis
|
Hypoxia
High affinity hemoglobins (Chesapeake; Denver) EPO producing tumors |