![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
144 Cards in this Set
- Front
- Back
- 3rd side (hint)
|
Wbc range |
4.6 to 6 female 4 to 5.4 male |
|
|
|
Hgb range |
Male 14 to 18 Femake 12 to 15 |
|
|
|
Hematocrit range |
Female 40 to 50 percent |
|
|
|
MCV range |
Norm is 80 to 100 fl Micro is less than 80 fl Macro is over 100 fl |
|
|
|
MCH range |
27 to 31 pg |
|
|
|
MCHC |
32 -36 |
|
|
|
Platelets |
150 to 450 times 10 |
|
|
|
RDW range |
11.5 to 14.5 High means anisocytosis If RDW is small than normal MCV. Is true If RDW is large than MCV average is not true |
|
|
|
Retics range |
0.5 to 1.5 percent |
|
|
|
Segs |
50 to 70 percent |
|
|
|
Bands |
0 to 5 percent |
|
|
|
Lymphs |
20 to 40 percent |
|
|
|
Eos |
1 to 4 percent |
|
|
|
Basos |
0 to 2 percent |
|
|
|
Pt and aptt times |
Pt is 11 to 13 seconds Aptt is 25 to 35 |
|
|
|
Fibrinogen |
200 to 400 mg /dl |
|
|
|
Thrombin time |
Less than 20 seconds ( mean is 8 to 10) |
|
|
|
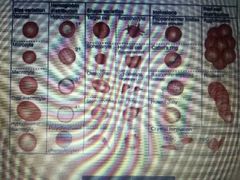
Pronormoblast is |
Rubriblast |
|
|
|
Basophollic normoblast |
Prorubricyte |
|
|
|
Polychromataphillic normoblast |
Rubricyte |
|
|
|
Orthochromic normoblast or acidophollic normoblast |
Metarubricyte |
|
|
|
Retic is retic |
Retic |
|
|
|
Erythrocyte |
Erythrocyte |
|
|
|
High rbc turnover |
Nucleated rbc Pllychromasia or polychromatic rbc Basophillic stippling Cabot rings Howell jolly bodies |
|
|
|
Left shift or bacterial infection release in severe and slight. |
Slight increase is bands and metamylocytes Severe is proliferative pool released Mylocytes and promyelocytes |
|
|
|
What u see in severe bacterial infection |
Increased wbc Increased lymph Left shift Vacuoles, toxic granulation.dohle bodies Pyknotic neutrophillia |
|
|
|
Changes in viral infection |
Normal wbc count Lymphocytosis Reverse diff *** more lymph than neutophils Reactive lymphs mono is 20 percent at least |
|
|
|
Decribe May hegglin |
Platlet disorder Giant platlets r found Inclusions similar to dohle bodies |
|
|

Name this |
May Hegglin |
|
|

Name this |
Alder reilly None specific azurophillic granules coarse dark |
|
|

|
Pelger huet or psuedo pelgeroid cellHypsegmentationDumbell shape |
|
|
Name this |
Chediak higashi Rare fatal kids In lymphs in monos !! Neuteophils have several large blue green staining mass |
|
|

Name this |
Barr body drumstick X chromosome in females |
|
|
Name this |
Reider cell. ( look like horse hoof) |
|
|

Name this |
Smudge cell Degenerated nuclei of cell 5 percent is poor slide making Can be chronic lymph leukemia |
|
|

Name this |
Auer rods Only in monos and myelo blasts Can be Aml or amol Faggot cell |
|
|

Name this |
Plasma cell think mm |
|
|
Name this |
Mott cells |
|
|

Name this |
Flame cell |
|
|
|
What is a leukoeythroblastic picture ? What cells would be present ? |
Immature red and white cells in peripheral blood Normoblast Myeloblasts Promyelocytes Myelocytes Metamyelocytes Can also see tear drop and polychromasia |

|
|

Sezary lymphs are a agressive form of what type of cells ? |
Cutaneous t cell lympoma Affect skin. Cancerous |
|
|

Name this |
Hairey cell |
|
|
|
What is the diseaee name for a cell with rod shapped inclusions and is a lipid storage disorder |
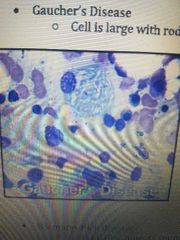
Gaucher disease |
|
|
|
Cell is round large and has evenly size lipid accumulation. |

Neimen pick |
|
|
|
No large identifiable bone marrow cells is what ? |
Tay sachs disease |
|
|
|
Just study this |
|
|
|
Stages of granulopoises |
Myeloblast promyelocyte myelocyte metamyelocte band and neutophil Eosinophils are band or eosinophils Same for baso |
|
|
|
Stages of platelets |
Megakaryocyte promegakaryocyte megakarocte then platlets |
|
|
|
Signs of anemia hint is high rbc turnover |
Poly Basophillic stippling nrbc Howel jolly bodies ( nuclear karyorrhexis) High RDW!! |
|
|
|
Micro / hypo . What is mcv and mchc as well as what type of anemia ? |
Mcv less than 75 Mchc less than 32 Problem with heme synthesis Iron deficiency anemia Tear drop cells few target cells shaggy nrbc |
|
|
|
Sideroblastic ( older pop) what will u see ? |
Siderocytes sideroblasts ( pappenheimer ) Dimophic Increased rdw |
|
|
|
What chain deletions are present with beta thalasemia major ? |
Little or no betta chains You will see polychromasia and a lot of target cells Low hgb 6 to 9 Increased RDW |
|
|
|
Chain deletion in beta thalasemmia minor ? |
1 abnormal beta gene Lots of target cells |
|
|
|
Alpha thalassemia is also called what and what are the gene deletions ? |
Barts 3 gene deletion Hgb H disease Heinz bodies |
|
|
|
Alpha silent carrier has how many gene deletionsis hetero or homo and mimics what? |
I gene deletion Hetero Mimics IDA but more target cells |
|
|
|
Hgb E is hetero or homo and u see what two types of cells ? |
Homo Target cells Microcytes |
|
|
|
Lead poisening you see what inclusion? |
Basophillic stippling |
|
|
|
Normocytic normochromic mcv and mchc |
Mcv- 80 to 100 fl Mchc 32 to 36 percent |
|
|
|
Macrocytic normochromic or hypchromic mcv and mchc ? What type of anemia ? |
Mcv is greater than 100 fl Mchc is normal or less than 32 percent B12 def / pernicious anemia / madro ovalcytes , howel jolly bodies , hyper segs , giant bands Pancytopenia MCV greater than 105 Also folic acid def. Alcoholism pregnancy hyperthrroidism Liver disease Round macro thin macro acanthocytes |
|
|
|
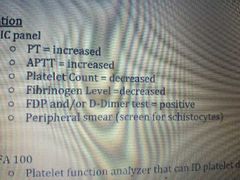
DIC explain Aptt pt Platlet count Fibrinogen level Fdp or d dimer test Perioheral smear tou see what? |
|
|
|
|
For platlet count to id platlet dysfunction you use what ? Name the cartridges |
PFA 100 collagen/epinephrine Collagen/Adp Specific for platlet dysfunction Due to asprin , resistamce. would be normal |
|
|
|
What specimen do you use for the pfa 100 |
800 ul of citrated whole blood |
|
|
|
Pfa 100 closure times for col/epi and col/ adp |
Col epi is 94 to 113 seconds Col adp is 71 to 118 seconds |
|
|
|
Reason for prolonged closure time with col epi? |
Inherited platlet dysfunction Vwd def Or platlet inhibiting agents Remember 94 to 113 |
|
|
|
Col adp reason for prolonged closure time ? |
You run this with col/ epi to differentiate medication induced dysfunction ADP would be increased *** Asprin patients show increased col/adp, if no increased the patient has asprin resistance. |
|
|
|
Prothrombin time measures what factors and is sensitive to what factors ? |
Extrinsic and common You add thomboplastin to ppp to activate extrinsic Factors are 7, 10 ,5 Prothrombin 2 Fibrinogen 1 Sensitive to vit k factors |
|
|
|
INR calculation |
Pt of patient divided by a normal pt times isi. |
|
|
|
INR measure what ? And increased values mean what? |
Normal is .9 to 1. 13 Moniters oral anticoagulants Increased means increased anticiagulation Coumadin is 2- 3.5 |
|
|
|
An INR over 2.o means what? |
Liver disease Factor 7 def Coumadin therapy Vit k def |
|
|
|
Aptt measures what ? |
Therapeutic range is 1.5 to 2.5 Measures intrinsic and common pathways Moniters heparin |
|
|
|
Explain mixing studies |
Mix patient and control . If factor defect than it will correct aptt time. If circulating anticoags are issue than it will not correct Therapeutic range is 1.5 to 2.5 times the normal |
|
|
|
Quantitative fibrinogen What is the range it shoukd be and causes of def. |
Less than 200 Caused by DIC qnd hypfibrinogenimia Fibrinogen turns into fibrin than thombin factor 2. |
|
|
|
Thrombin time determines the rate of what? Name reason for greater than 20 seconds? |
Determines rate of thrombin induced cleavage of fibrinogen to fibrin monomers. Greater than 20 seconds means Fibrinogen less than 100 mg /dl Theombin inhibits heparin Multiole myeloma |
|
|
|
Fibrin degradation products or FDP measures what? |
Tests for the product of fibrinolysis Measures x y d e You would show increased Acute and chronic DIC Systemic fibrinolysis Pulomary emboolism ****does not distinguish between DIC and systemic fibrinolysis |
|
|
|
A d dimer is specific for what ? |
DIC SYSTEMIC fribronolysis |
|
|
|
What is the difference between heparin and warafin( coumadin) |
Heparin binds antithombin enhancing neuralization of serine proteases Warfin is a vit k antagonist ( carboxylation step ) Makes non functional factors that are dependent on K 2 7 9 and 10) Protein c and s U moniter the pt and inr. |
|
|
|
Antiplatlet therapy is what med? And how does this work ? |
Inhibits cyclooxygenase blocking prostaglandin synthesis |
|
|
|
Name the hemoglobin in sickle cell DISEASE and what types of cells will be present . Is it homo or hetero ? |
Homo for hgb S most is hgb S You will see sickle cells, target cells, nrbc , howell jolly bodies
On electeophorphoresis no hgb A IS PRESENT !!
|
|
|
|
Sickle cell TRAIT has ehat type of hgb and what cells will be present. Is it hetero or homo? |
Hetero hgb S Most is hgb A which is diff form disease U see target cells not many On electeophorphoresis ull see hgb A and S |
|
|
|
Hgb C has what type of hgb and what descent of people is it from ? What cells are present ? |
Affects patients from western Africa or west african descent Cbc shows Mild to mod anemia Target cells and hgb c crystals ( bar of gold) Electrophoresis is C ( homo) A, and c ( hertero) |
|
|
|
Hgb E is prevalent in people of what descent ? The CBC shows what? |
Effects southeast asia ( thailand ) Mild anemia where C can be mild or moderate You ll see microcytes and target cells Electophoresis is postive for E. |
|
|
|
Hgb SC. What will be present on slide |
Mild anemia Target cells and hgb SC crystals ( looks like birds or fingers ) S and C on electeophorphoresis |
|
|
|
Thrombocytopenia conditions are either .... |
Immune or non immune |
|
|
|
Immune thrombocytopenia shows what? |
Neonatal alloimmune thrombocytopenia Immune thrombocytopenic purpura also thrombrotic " " Acute and chronic ITP Heparin induced thrombocytopenia |
|
|
|
Non immune thrombocytopenia |
Von willibrands disease Aptt normal to increased Vwf is decreased |
|
|
|
In factor 8 def you have what disease process and aptt is what? |
Hemophilia A Aptt is normal to increased |
|
|
|
In factor 9 def. Is what disease process? Aptt is what? |
Hemophilia B or christmas disease Aptt is normal to increased |
|
|
|
Factor 11 def is what ? Aptt is what? |
Factor 11 is hemophilia C. Aptt is normal to increased |
|
|
|
Afribringenemia is absent what ? And the pt and aptt are both what ? |
Pt and aptt are normal . Fibrinogen is absent |
|
|
|
Hypofibrinogenemia have all normal what? |
Pt and aptt and fibrinogen |
|
|
|
Vit K deficiency have what pt and aptt ? |
Pt is increased Aptt is normal Protein c and s are decreased |
|
|
|
Liver disease has what aptt and pt and fibrinogen |
Pt increased Aptt increased Fibrinogen decreased |
|
|
|
Dic aptt and pt and fibrinogen ? |
Aptt and pt increased D dimer increased Fibrinogen is decreased |
|
|
|
Fibrinolysis has a neg or postive d dimer ? |
Neg d dimer |
|
|
|
Myeloprolif means overproduction of what type of cells ? |
Granullocytic , rbc ,and platelet leading to neoplasms |
|
|
|
In chronic myelogenous luekemia u have a accumulation of all neutophil stages. Name the blast percentage, amount of wbc ? |
Blasts are less than 20 percent Wbc is over 100,000 Left shift and hypercellular marroe Elevated eos and basos |
|
|
|
In polycythemia vera you have an increase in what type of cells and what is the gene that is the mutation and then what would be the treatment for it? |
You have an increase in red blood cells granulocytes and platelets increase in red blood cell hemoglobin but the erythropoietin levels are low or decreased the gene that is present is the jak2 v617f mutation you have an elevated hemoglobin and hematocrit the red blood cell morphology is normal treatment would be therapeutic phlebotomy and you're going to have pan hyperplasia in the bone marrow |
|
|
|
Essential thrombocythemia shows an increase in what type of cells and has an increased what |
megakaryopoiesis increase platelets and platelets may not function increase platelet count older populations pan hyperplasia massive megakaryocytes increase lap score |
|
|
|
Primary myelofibrosis you will see an increase and what type of hematopoiesis and you will see what type of cells |
You going to have bone marrow fibrosis extra medullary hematopoiesis increase in megakaryocytes you have red blood cell and platelet abnormalities teardrop cells nucleated red blood cells polychromasia and a dry tap |
|
|
|
Chronic neutrophilic leukemia you're going to have an elevation and what type of cells in the absence of what type of chromosome |
Elevated white blood cell major increase in neutrophils precursors absence of Philadelphia chromosome elevated eosinophil count no eosinophilia though immature is eosinophils peripheral circulation |
|
|
|
In chronic lymphocytic leukemia or lymphocitic lymphoma you're going to have an increase in what type of mature cell it is the most common and what type of person |
You're going to have mature b-cell disorder elevated white blood cell count smudge cells DAT positive common in older adults |
|
|
|
And hairy cell leukemia you have what type of cell present |
Chronic b-cell neoplasm with limps showing hairy projections |
|
|
|
In acute lymphocytic leukemia you're going to have what percentage of blasts |
Presence of more than 20% lymphoid blasts |
|
|
|
Acute myeloid leukemia you're going to have what percentage of blasts and what type of cells and inclusions this is most common in what type of person |
Over 20% blast auer rods pseudo pelger huet cells howel Jolly bodies pappenheimer bodies basophillic stippling nucleated red blood cells most common in children |
|
|
|
Chronic myelogenous leukemia you will see what type of cells and inclusions it is the most common Mpd after the age of what what chromosome is present |
Segs and Myelocytes predominate increased eosinophils and basophils pseudo pelger huet cells nucleated red blood cells most common MPD after age 55 the Philadelphia chromosome |
|
|
|
Myelodysplastic syndromes are most common and what type of patient and is caused by exposure to what |
Most common in the elderly due to exposure to chemicals radiation chemo or viral infections can transform into acute leukemia |
|
|
|
Refractory anemia with ringed sideroblasts show what percentage of rain sideroblast |
Less than 15% ring sideroblasts no blasts in peripheral blood |
|
|
|
Refractory anemia with excessive blasts you will see a decrease in what cell lines have blast with what and decrease in what cell line. |
Cytopenias in all three cell lined may have auer rods and decreased monocytes |
|
|
|
Chronic myelomonocytic leukemia you're going to have what percentage of blasts and dysplasia and what cell line |
Elevated white blood cell count and monocytosis less than 20% blasts and pro monocytes dysplasia and one or more myeloid line |
|
|
|
In Hodgkins lymphoma he will have what type of cells |
Tumor of lymph nodes and the presence of reed-sternberg cells in the tumor they look like owl eyes or popcorn |
|
|
|
Non-Hodgkin's lymphoma you will have what type of cells and what cell line |
B cell line is most common sezary syndrome is example of T-cell lymphoma |
|
|
|
Multiple myeloma you will have what on the smear an increased what and malignant what cells |
Rouleax on blood smear bence-jones proteinuria increased ESR malignant plasma cells in bone marrow |
|
|
|
Plasma cell leukemia is a form of what and you have what two things that happen |
It's a form of multiple myeloma where plasma cells are in the peripheral blood you have pancytopenia Rouleax |
|
|
|
Waldenstroms macroglobulinemia has monocloncal gammopathy due to what? |
Increased igm Plasmacytoid lymphs or plasma cells on smear Bence jones proteinemia |
|
|
|
Burkitt's lymphoma medium-sized blasts with what it looks like what and is caused by what virus |
Medium sized blast with sharp lipid vacuoles Starry Sky appearance abdomen or jaw tumors from Epstein-Barr virus |
|
|
|
How do you calculate MCHC |
Hemoglobin / hematocrit * 100 so just remember MCHC the word hematocrit is longer so that's what you divide hemoglobin by |
|
|
|
MCH calculation |
Hemoglobin * 10 / the red blood cells remember red blood cell on the bottom three letters MCH |
|
|
|
MCV calculation |
Hematocrit * 10 / the red blood cell count |
|
|
|
Manual white blood cell equation |
Average number of cells * 10 * the dilution factor divided by 4 |
|
|
|
How are samples identified on the max M or s t k s |
Scan barcode and you get your test it's based on angles and light scatter |
|
|
|
How are white blood cells measured using Max M or stks? |
White blood cells use later light scatter nephelometry scatters off of granularity and conductivity to differentiate volume |
|
|
|
How are red blood cells measured on the max m or stks |
Volume and cell size classified based on granularity |
|
|
|
How are platelets measured on the STK s or M A x m |
Began through light scatter laser electrical impedance the current low frequency and size threshold |
|
|
|
Colter's term opacity means what |
The ability to see the internal structure |
|
|
|
What is the purpose of sweep |
prevents cells from re-entering The sensing zone on a pulse of air flow lines |
|
|
|
Sysmex is reference method not conductivity it gets into the nucleus |
. |
|
|
|
Abbott is the only one with what |
The only one that has markers that differentiate with flow cytometry |
|
|
|
What parameters are measured off of the histogram |
Platelet RDW and MCV |
|
|
|
What parameters are measured directly |
Lymphocytes hemoglobin white blood cells pmn red blood cells |
|
|
|
What measurements are computed |
Hematocrit monocytes |
|
|

|
One is blasts myeloblast to is immature Gran's and bands 3 is aged cell so aged neutrophils 4 is nucleated red blood cells 5 is platelet clumps 6 is chronic lymphocytic leukemia variant lymphocytes and 7 is varient lymohs but it would be immature 8 is blast lymphoblast and 9 is monoblasts |
|
|
|
The Coulter principle |
Particles are pulled through an orifice with electric current the change in impedance is proportional to the volume of the particle going through the office the pulse impedance originates from the displacement of electrolytes caused by the particle |
|
|
|
Fibrinogen is factor ? |
1 |
|
|
|
Prothrombin is factor ? |
2 |
|
|
|
Tissue factor thromboplastin is factor |
3 |
|
|
|
Calcium is factor |
4 |
|
|
|
Proaccelerin labile factor is factor |
5 |
|
|
|
Proconvertin stabile factor |
7 |
|
|
|
Antihemopillic factor |
8 |
|
|
|
Stuart prower factor |
10 |
|
|
|
Xmas factor |
9 |
|
|
|
Thromboplastin antecedent |
11 |
|
|
|
Hageman factor |
12 |
|
|
|
Fibrin stabilizing factor transglutinase |
13 |
|